
Ironworker Foreman Crushed When Bridge Support Element Broke During Dismantling
New York Case Report 05NY013
Summary
On February 24, 2005, a 43-year-old male ironworker foreman, who was employed by a construction company, sustained fatal injuries when elements of a bridge support structure he was dismantling broke apart and he was crushed between them at a bridge construction site. On the day of the incident, the victim and a co-worker were dismantling a span of a temporary bridge support. The span was a steel framework consisting of two pairs of 77-foot-long steel W36 I-beams and several W12 I-beams. In preparation for dismantling, a triangular-shaped steel element, called a pile cap, weighing approximately 8,000 lbs., was welded and chained to the ends of the W36 beams by a steel chain. The span was then removed from the support and placed on a floating barge where the remainder of the dismantling took place. At the time of the incident, the victim and his co-worker were on the barge dismantling the third pile cap of the day. To safely dismantle a pile cap, the cap was to be rigged with a crane before cutting the welds with a torch to free the cap from the I-beams. However, prior to the incident, the victim had been seen operating a torch on top of the pile cap that was involved in the incident before the cap was rigged to the crane hoist. The victim was straddling the two sides of the cap near its tip and the co-worker was standing on the base of the cap when the cap suddenly broke away from the I-beams. The co-worker was thrown into the river and was not injured. He swam to the barge and was pulled out of the water. The victim, however, was crushed between the pile cap and the ends of the W36 beams. The cap hung on the chain above the water, with the victim lying on the pile cap partially submerged in water. The site foreman immediately called 911 while other workers got into a motor boat to rescue the victim. They moved the victim into the boat and then onto the riverbank. Resuscitation efforts were performed on the victim before EMS’ arrival. The victim was pronounced dead at the scene.
New York State Fatality Assessment and Control Evaluation (NY FACE) investigators concluded that to help prevent similar incidents from occurring in the future, employers should:
- Provide task-specific employee refresher training addressing proper dismantling procedures;
- Strictly follow construction project engineering plans and get approval from the project engineer for any deviations from the original plan;
- Perform quality control inspections on the jobs and tasks completed during each stage of a construction project;
- Ensure that all workers use fall protection equipment when there is a potential fall hazard and;
- Ensure that safe access to working areas is provided to workers at each work site.
Introduction
On February 24, 2005, a 43-year-old male ironworker foreman (the victim), who was employed by a construction company, sustained fatal injuries when elements of a temporary bridge support he was dismantling broke apart and he was crushed at a bridge construction site. NY FACE investigators learned of the incident on February 25th from an area office of the Occupational Safety and Health Administration (OSHA). On March 5th and 6th, a NY FACE investigator traveled to the incident site to conduct a fatality evaluation. During the site visits, the NY FACE investigator met with representatives of the construction company, observed the preserved incident scene, interviewed witnesses, and reviewed the company’s safety and health programs and employee training records. The case was reviewed with the OSHA compliance officer who investigated the incident. The police report and Medical Examiner’s report were also reviewed. The New York State Department of Transportation (NYSDOT), which owned the bridge, also conducted an investigation.
The victim’s employer was a large civil and heavy industrial construction company that was founded in 1949. At the time of the incident, it employed approximately 2,000 non-union workers and served southern New England and New York State. The company provided all field employees with 30-hour construction safety training. Daily crew meetings were held at each job site to discuss specific hazards and preventive measures. Workers were provided with hard hats, safety glasses, gloves, steel-toed work boots, face shields for cutting or welding, life jackets and personal fall arrest systems.
The victim had been employed by the company for eleven years. At the time of the incident, his job title was ironworker foreman. The company had strengthened its safety programs in 1987 after experiencing 14 worker fatalities during the previous 16 years. Since 1987, six employees, including the victim, have died in work-related incidents.
Back to Top
Investigation
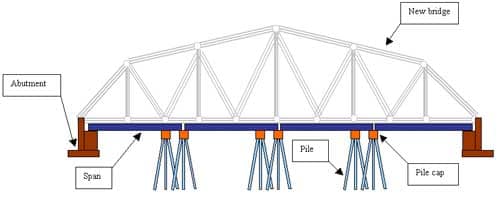
At the time of the incident, the company had been contracted by the NYSDOT as a general contractor for a multi-phase bridge construction project encompassing two construction sites. At one site, the company erected a temporary bridge support structure to provide support for assembling and erecting the new bridge. The temporary support structure was to be dismantled and removed as soon as the new bridge was erected. The fatal incident occurred during the dismantling of the temporary under-bridge.
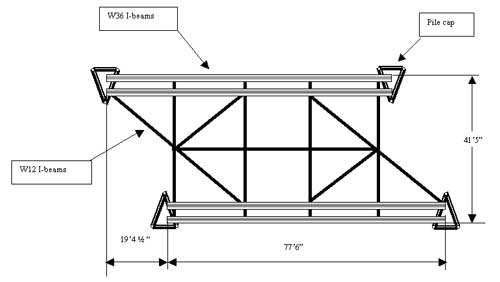
The temporary under-bridge had four spans that were supported by six steel piles and the abutments (Figure 1). There was a pile cap (Figure 2 and Photo 1), a triangular-shaped steel element weighing approximately 8,000 lbs., on top of each pile and the spans rested on the six pile caps. A span was a steel framework consisting of two pairs of 77-foot-long steel W36 I-beams and several W12 I-beams (Figure 2 ). In preparation for dismantling, the caps were welded and chained to the ends of the W36 beams by a test steel chain. The spans along with the attached pile caps were then removed one at a time from the temporary bridge support and placed on a floating barge where the remainder of the dismantling took place (Photo 2).
|
|
|
Figure 2. Overhead depiction of the third span of the temporary under-bridge.
|
On the morning of the incident, eight workers, including the victim, arrived at the site at approximately 7:00 a.m. A crew meeting was held to discuss the tasks of the day, the potential safety hazards associated with the tasks, the preventive measures, and the required personal protective equipment. The items discussed were recorded on a Daily Work Activity Hazard Analysis form and the form was signed by each of the workers who attended the meeting.

|

|
|
Photo 2. Overview of the barge and workstation where the temporary bridge span was placed and being dismantled.
|
Work started immediately following the crew meeting. Workers entered the work platform on the floating barge through a ladder that was placed against the riverbank and a catwalk (Photo 3). The ladder served as the only access to the barge and was unstable. The top of the ladder was covered with ice and snow at the time of the incident.
The major task of that day was dismantling the third under-bridge span along with the four pile caps attached to it. The span was placed on the barge approximately ten feet above the water. The company required workers to wear fall protection and to be tied to an anchorage when working ten feet in the air or higher. OSHA regulations require employees to be protected from falling if working on elevations of six feet or higher. The victim and his co-workers wore life jackets, but did not use fall protection on the day of the incident.

|
|
Photo 3. The ladder and catwalk that served as the only entrance to the barge.
|
The victim, a co-worker, and a crane operator were assigned to dismantle the caps. To safely dismantle a cap, the workers were to follow five critical steps: 1) rig the pile cap with the crane hoist cable; 2) tension the crane cable; 3) remove the steel chain; 4) cut the welds with a torch to free the cap; and 5) signal the crane operator to lift the cap and place it on the land. These steps were not included in the written engineering project plan. According to company representatives, the crew had discussed the steps during the morning meeting that day. The victim and his co-worker safely removed the first two caps following the proper procedures that morning.
By 10:00 a.m., the crew was ready to dismantle the third cap. The same crane that was used to lift the first two caps could not reach the third cap, and the crane operator had to switch to another crane that was located on the barge. At approximately 10:15 a.m., the crane operator started the second crane and waited for it to warm up. At the same time, the co-worker was on the barge setting up another torch and the victim was standing on top of the third pile cap with a torch. At least two witnesses recalled seeing the victim cutting on the cap with a torch, but no one could confirm what part of the cap he was cutting.
 |
|
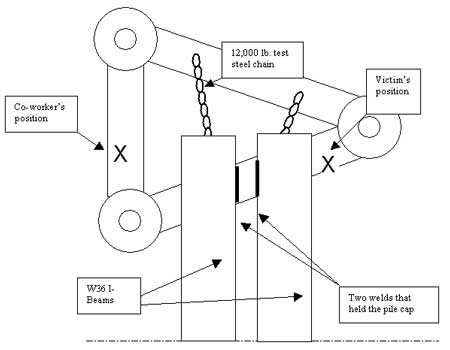
Figure 3. The victim and co-worker’s positions on the pile cap at the time of the collapse.
|
Just prior to the incident, the co-worker got on the cap to assist the victim with rigging. The victim was straddling the two sides of the cap near its tip and the co-worker was standing on the base of the cap (Figure 3). Before they were able to rig the cap to the crane cable, the cap broke apart from the W36 I-beams and swung on the chain towards the ends of the W36 beams. The victim was crushed between the swinging pile cap and the ends of the W36 beams. The cap hung on the test chain above the water (Photos 4 and 5) with the victim lying on the pile cap partially submerged in water. The co-worker was thrown into the river and was not injured; he swam to the barge and was pulled out of the water by two workers.

|

|
|
Photo 5. The pile cap hung by the test chains after it broke apart from the W36 I-beams.
|
Immediately following the incident, the site foreman called 911 to summon emergency medical service, while two workers got into a motor boat and went around the barge to rescue the victim. They moved the victim from the pile cap into the boat and then onto the riverbank. A NYSDOT-contracted engineer who was CPR certified performed resuscitation efforts on the victim. EMS arrived at the site in eight minutes. The victim was pronounced dead at the scene.
The post-incident examination revealed that the cap had been welded to the W36 I-beams with two welds. It appeared that both welds had been partially cut prior to the incident. The company’s original engineering plan dictated that all pile caps were to be bolted to the I-beams with four 7/8” A325 bolts and chained to the W36 beams with two 5,000 lb. test steel chains. Later, the job site superintendent proposed to replace the bolts with welds. The company professional engineer (PE) approved the request and specified that each cap should be welded to the W36 beams with four welds and chained to the beams with two 5000 lb. test steel chains. However the cap that was involved in the incident had been welded to the girders with only two welds instead of four, and all pile caps were chained to the W36 beams with a single 12,000 lb. test chain rather than two 5,000 lb. test chains. These deviations were not communicated to nor discussed with the PE. According to the company PE, the two welds on the cap would not have provided a sufficient safety margin to support the weight of the pile cap and the additional loads.
Back to Top
Cause of Death
The cause of death was listed by the Medical Examiner as crushing chest injuries.
Recommendations/Discussion
Recommendation #1: Employers should provide task-specific employee refresher training addressing proper dismantling procedures.
Discussion: Immediate employee retraining should be provided in the event of an incident, a near-miss incident, or changes in operational procedures or equipment. The proper procedure for safely dismantling pile caps should be included in the written project plan and reviewed with the crew. The employer should ensure that workers understand the importance of following the dismantling steps in the correct order. Workers should be encouraged to report any unsafe behaviors to the project supervisors and site superintendent. Management should increase supervision to ensure that workers follow appropriate safety procedures.
Recommendation #2: Employers should strictly follow construction project engineering plans and get approval from the project engineer for any deviations from the original plan.
Discussion: Employers should strictly follow project engineering plans and specifications and discuss any intended modifications of the plan with the project engineer (PE). No deviations from the original plan should be allowed unless reviewed and approved by the PE. In this case, the third cap that was involved in the incident was welded to the girders with two welds instead of four, as approved by the PE. Also, the steel chains connecting the pile caps to the girders were different from what was specified by the PE.
Recommendation #3: Employers should perform quality control inspections on the jobs and tasks completed during each stage of a construction project.
Discussion: Employers should perform quality control inspections on tasks completed during each stage of a construction project, and ensure that each task conforms to engineering specifications. If deviations are found, the project engineer should be immediately notified and consulted. Appropriate actions should be taken based on the project engineer’s evaluations and recommendations.
Recommendation #4: Employers should ensure that all workers use fall protection equipment when there is a potential fall hazard.
Discussion: The victim and his co-worker were working approximately ten feet above the water on the barge at the time of the incident; neither of them was using fall protection equipment. Employers should ensure that all workers use appropriate fall protection equipment when they may be exposed to a fall hazard as required by OSHA. However, using fall protection equipment in this case may not have prevented the fatal injury.
Recommendation #5: Employers should ensure that safe access to working areas is provided to workers at each work site.
Discussion: Employers should provide workers with safe access pathways to each work site. Unsafe work site. access is a potential hazard for workers. In this case, a ladder was placed between the riverbank and the work platform to serve as the only access to the barge. Workers may have fallen while climbing the ladder. Unsafe access pathways may also hinder and delay rescue efforts during an emergency situation. Following this incident, the company removed the ladder and built a catwalk with railings for fall protection for workers to access the barge.
Back to Top
References
General Safety and Health Provisions
29 CFR 1926.20. Code of Federal Regulations, Washington, D.C., U.S. Government Printing Office, Office of the Federal Register.
Ladders
29 CFR 1926.1053. Code of Federal Regulations, Washington, D.C., U.S. Government Printing Office, Office of the Federal Register.
Marine Operations and Equipment
29 CFR 1926.605. Code of Federal Regulations, Washington, D.C., U.S. Government Printing Office, Office of the Federal Register.
Fall Protection
29 CFR 1926.500. Code of Federal Regulations, Washington, D.C., U.S. Government Printing Office, Office of the Federal Register.
29 CFR 1926.501. Code of Federal Regulations, Washington, D.C., U.S. Government Printing Office, Office of the Federal Register.
29 CFR 1926.502. Code of Federal Regulations, Washington, D.C., U.S. Government Printing Office, Office of the Federal Register.
Back to Top
New York FACE Program
The Fatality Assessment and Control (FACE) program is one of many workplace health and safety programs administered by the New York State Department of Health (NYS DOH). It is a research program designed to identify and study fatal occupational injuries. Under a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), the NYS DOH FACE program collects information on occupational fatalities in New York State (excluding New York City) and targets specific types of fatalities for evaluation. NYS FACE investigators evaluate information from multiple sources. Findings are summarized in narrative reports that include recommendations for preventing similar events in the future. These recommendations are distributed to employers, workers, and other organizations interested in promoting workplace safety. The FACE program does not determine fault or legal liability associated with a fatal incident. Names of employers, victims and/or witnesses are not included in written investigative reports or other databases to protect the confidentiality of those who voluntarily participate in the program.
To contact New York State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.