
Logger Crushed While Felling a Tree
Case Report: 02NY013
SUMMARY:
On March 20, 2002, a 36-year-old male logger died as a result of being crushed by a fallen oak tree. The victim had been working by himself in a remote area felling trees on the day of the incident. As the logger finished making the final cut on the oak tree he was felling, he began to walk away from the area. As the oak tree was falling, it hit another tree that horizontally crossed another standing tree. As the falling tree hit this crossed tree, the butt of the falling tree was thrown up into the air and backwards away from the stump. The logger was knocked down by the falling tree, and was subsequently crushed underneath the weight of the tree. When the logger did not return home, his wife became concerned and called a co-worker. The co-worker was able to find the logger after some searching, and called for Emergency Medical Services (EMS) with his cell phone. EMS responded and transported the victim to the hospital where he was pronounced dead by the county coroner.
New York State Fatality Assessment and Control Evaluation (NY FACE) investigators concluded that to prevent similar incidents from occurring in the future, loggers should:
- Utilize proper notching techniques when felling trees;
- Fell trees in areas clear of hazards;
- Work in teams while felling trees.
INTRODUCTION
On March 22, 2002, the New York State Department of Health FACE program received notification of a logging related fatality through a newspaper article. The victim was a 36-year-old male logger who was felling an oak tree at the time of the event. After making the felling cut, and as the tree was falling, the butt of the tree rebounded, knocking the logger over and crushing him to death.
On June 14th, 2002, a NY FACE investigator, who is also an agricultural safety specialist, visited with the OSHA compliance officer who had investigated this incident. In addition to the OSHA related investigation materials, materials were reviewed from the New York State police and coroner. Additional information was gathered from media reports.
The victim was the owner and operator of a small logging company that cut trees in the Adirondack region of New York State. In addition to himself, the victim had employed a fulltime worker for the past three years. Usually the two workers worked together on a site; however, on the day of the incident the owner was working by himself logging trees on a remote piece of private property for a client.
INVESTIGATION
On March 20, 2002 the logging company owner, working by himself, was beginning to cut oak trees on a piece of mountainous property approximately 1 mile removed from the roadway. As the logger began his work, the conditions were winter-like with heavy snow falling that continued throughout the day. At approximately 9:00am, as the logger was felling a large oak tree approximately 18 inches in diameter, the logger cut an angled wedge from one side of the stump of the tree. He then made a cut from the backside of the tree meeting the wedge shaped cut in an effort to fell the tree. He cut almost cleanly through leaving approximately ½ inch section of connected wood in the center of the stump of the tree whereby the tree would hinge and rotate as it fell. As the tree began falling, it struck a standing tree with another tree that was crossed horizontally. The falling oak tree hit the two obstacle trees at approximately its balance point. This threw the butt of the falling tree up into the air and backwards away from the stump. The logger was approximately 15 feet away from the stump, heading away, as is the practice once the final cut has been made. At that time, the butt of the falling tree rebounded, and he was knocked down and crushed underneath the weight of the tree.
When the logger did not return home that evening, his wife became concerned and at approximately 9:30pm she called the co-worker to see if he could help locate the logger. The employee went to the area where he knew the logger had been cutting that day, but due to the approximately 12 inches of heavy snow that had fallen during the day, he was unable to immediately find the victim. He did discover fresh cut trees, and after digging down through the snow, discovered that the logger was crushed under one of these trees.
The employee immediately called the wife and the emergency rescue squad, who also notified the state police. Both the police and the fire rescue squad responded to the incident location where the victim was found dead. Inspection of the scene revealed that the logger was wearing the recommended personal protective equipment and that his logging helmet was immediately in front of him on the ground and had been knocked from his head. He was wearing logging safety chaps, a safety vest and proper boots. His chainsaw was also found next to him on the ground. The location where the victim was located was approximately 15 feet from the stump of the tree he had last cut. Rescue personnel also discovered that the log skidder the logger used was sitting in the woods with the engine still running after 12 ½ hours.
The victim was removed from the location and transported to the local hospital where the county coroner pronounced him dead.
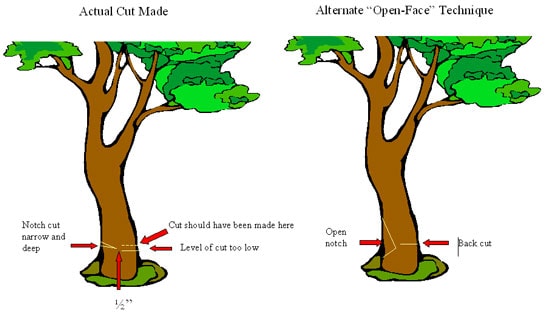
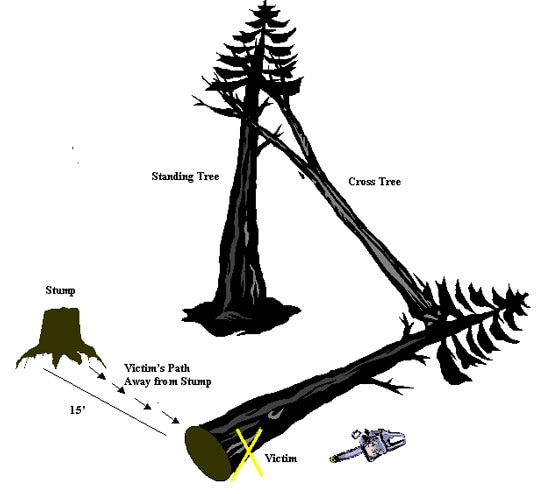
Upon reconstructing the scene and looking at the surrounding trees and the cutting technique used on this tree, it is believed that the cutting technique for felling the tree was not performed in a way that would leave a sufficient hinge section of wood in the stump to control the tree as it fell (Figure 1). There was approximately ½ inch hinge of wood across the stump; there should have been a hinge more in the range of 1-2 inches in width to help control the tree as it fell. Additionally, the tree was felled in the direction of a snag, or crossed tree that was horizontal in the woods (Figure 2). As the tree fell, it struck both this crossed tree and the standing tree it was leaning against. At the point of contact, it created a pendulum effect that increased the pressure on the base of the tree throwing the butt section, or the bottom of the tree, out away from the stump. Since there was a not sufficient hinge section of wood connecting the stump to the butt of the tree, the butt of the tree shot out backwards away from the direction of the fall, allowing the butt to strike the logger as he vacated the cutting area. The logger appeared to be retreating in the correct path; unfortunately, he was struck and knocked down by the base of the tree during the unexpected kick-out. An alternate escape path would not have helped in this situation since the tree swung out so quickly, not allowing any reaction time.
 |
|
Figure 1. Tree Trunk Cuts: Comparison of Actual Cut Made and Alternate “Open-Face” Technique
|
|
Figure 2. Forest Layout
|
CAUSE OF DEATH
The cause of death was determined to be crushing injuries to the chest and upper abdomen.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Loggers should utilize proper notching techniques when felling trees.
Discussion: In this case the victim made a very shallow angle notch, and then made the back cut too low and almost completely through the tree. The proper notch directs the tree’s fall and the hinge wood keeps the tree under control as it falls. OSHA Regulation 29 CFR 1910.266(h)(2)(vi) requires that a back cut be made leaving sufficient hinge wood to hold the tree to the stump during most of its fall. In this case, the ½” hinge section that was left easily broke. Professional loggers are instructed in the proper use of 3 differing felling techniques that help to eliminate the above hazards.
Recommendation #2: Loggers should fell trees in areas clear of hazards.
Discussion: The forest area surrounding the tree to be felled should be cleared of all crossed/suspended trees and other obstacles that may interfere with the fall of the tree. Any surrounding obstacles should be cleared from the area prior to felling, and trees should then be dropped in a direction towards safety. OSHA Regulation 29 CFR 1910.266 (h)(1)(vi) states “each danger tree shall be felled, removed or avoided. Each danger tree, including lodged trees and snags, shall be felled or removed using mechanical or other techniques that minimize employee exposure before work is commenced in the area of the danger tree. If the danger tree is not felled or removed, it shall be marked and no work shall be conducted within two tree lengths of the danger tree unless the employer demonstrates that a shorter distance will not create a hazard for an employee.”
Recommendation #3: Loggers should work in teams while felling trees.
Discussion: Working alone in the woods can be hazardous due to the remote areas and the multitude of obstacles. Co-workers can help to assess surrounding hazards and direct safe felling locations. In addition, co-workers can provide assistance in the event of injury.
REFERENCES
- CDC/NIOSH. NIOSH Alert. Request for Assistance in Preventing Injuries and Deaths of Loggers. December 1994.
- CFR. Code of Federal Regulations [2003]. 29 CFR 1910.266, Logging Operations. Washington, D.C.: U.S. Government Printing Office, Office of the Federal Register.
- West Virginia FACE Report No. 99WV026. Tree Feller Dies After Being Struck by Tree Being Felled in West Virginia.
- West Virginia FACE Report No. 97WV05. Hog Farmer/Logging Company Owner Dies After Being Struck by a Falling Tree—West Virginia.
The Fatality Assessment and Control (FACE) program is one of many workplace health and safety programs administered by the New York State Department of Health (NYS DOH). It is a research program designed to identify and study fatal occupational injuries. Under a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), the NYS DOH FACE program collects information on occupational fatalities in New York State (excluding New York City) and targets specific types of fatalities for evaluation. NYS FACE investigators evaluate information from multiple sources. Findings are summarized in narrative reports that include recommendations for preventing similar events in the future. These recommendations are distributed to employers, workers, and other organizations interested in promoting workplace safety. The FACE program does not determine fault or legal liability associated with a fatal incident. Names of employers, victims and/or witnesses are not included in written investigative reports or other databases to protect the confidentiality of those who voluntarily participate in the program.
To contact New York State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.