
Two Feedlot Workers Suffocated in Grain Bin
Nebraska FACE Investigation 99NE016
June 28, 1999
SUMMARY:
A 23-year-old mill operator and a 20-year-old maintenance technician were killed when they were engulfed in corn in a 6,000 bushel cone bottom gravity feed bin at a feedlot. The two individuals had been “knocking down” soy bean meal in a gravity feed bin next to the corn bin prior to the incident. For some reason, after their work in the soy bean meal bin they went to the corn bin and both individuals became engulfed in cracked corn. Both of these bins were active, flowing soy bean meal and cracked corn into a “clam” approximately once every five to ten minutes. The “clam” was then emptied into feed trucks. When the corn flowed from the bin, this pulled the victims under the corn. When others at the feedlot realized the two were trapped in the corn, they cut openings in the bottom of the bin to release the corn and rescue the victims. Both individuals died from suffocation.
The Nebraska Department of Labor Investigator concluded that to prevent future similar occurrences employers should:
- ensure a permit is issued prior to entering bins.
- ensure all equipment which presents a danger to employees is locked-out, blocked-off, or otherwise prevented from operating.
- ensure employees are wearing appropriate fall protection anytime they are exposed to a fall into a bin or silo.
- provide and have in place equipment for rescue operations which is specifically suited for the task being conducted.
- develop, implement and enforce a comprehensive safety program that includes, but is not limited to, training in all hazard recognition and abatement.
- consider installing locks on all accesses to bins and silos and controlling the keys to the locks.
- consider installing phones in close proximity to bins and silos which are normally entered, or providing teams entering bins and silos with cell phones or two-way radios to provide communications to the mill operator.
PROGRAM OBJECTIVE:
The goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent work-related deaths or injuries in the future by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact.
This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries.
INTRODUCTION:
On April 13, 1999, at approximately 11:00 a.m., a 23-year-old mill operator (worker 1) and a 20-year-old maintenance technician (worker 2) were killed when they were engulfed in corn in a 6,000 bushel cone bottom gravity feed bin at a feedlot. The Nebraska Department of Labor became aware of the fatality on April 13, 1999, via the radio and a phone call from an individual representing the company. The Nebraska FACE Investigator, in conjunction with OSHA Compliance Officers, conducted a site visit on April 14-15, 1999. Interviews were conducted with the feedlot manager and the victim’s supervisor.
The feedlot has been in business for 20 years. The 23-year-old victim had been employed by the company for 16 months and the 20-year-old for 8 months. The number of employees in the company is 35. The company does not have a full-time safety manager. The safety responsibilities are handled by the feedlot manager. The company does have a written safety program. These were the first fatalities at the feedlot, however one of their truck drivers was killed in a traffic accident in the past.
INVESTIGATION:
On the morning of the incident, worker 1 began work at 6:00 a.m. and worker 2 began work at 7:00 a.m. The incident location is a feedlot which feeds approximately 44,000 head of cattle. During the workday (6:30 a.m. to 5:00 p.m.) feed trucks are filled approximately once every 10 minutes throughout the day. The trucks then distribute the feed into troughs for the cattle. The feed is a mix of cracked corn and soy bean meal. There are two bins (one for corn and one for soy bean meal) which empty into a clam which in turn is dumped into the feed trucks. The clam holds a load for one truck and therefore it is filled approximately once every 10 minutes during the workday.
On the morning of the incident worker 1 and worker 2 had been “knocking down” soy bean meal in one of the bins that feed into the clam. The soy bean meal tends to clump up and workers enter the bin to loosen it. Workers 1 and 2 were taking turns “knocking down” the meal with a scraper or shovel. Their supervisor had visited with them a couple of times the morning of the incident and said the worker in the bin each time was wearing a safety harness and tied off with a lifeline.
While workers 1 and 2 were supposedly working in the soy bean meal bin the mill operator noticed a “corn bin full” indicator lighted on his control panel. The corn bin had corn flowing from it approximately every 10 minutes and should not have been full. The flow rate out of the corn bin is approximately 80 bushels per minute and the clam holds 250 bushels (the mix of corn and soy bean meal at the time was approximately 240 bushels of corn and 10 bushels of soy bean meal). Therefore, each time the corn flowed from the bin, it flowed about three minutes. The normal level for the corn bin at the time of the incident would have been about half full. Corn was being rolled into the corn bin from larger storage silo that kept it approximately half full. The mill operator turned off the rollers so the corn bin would stop filling up. He then contacted the yard supervisor on his cell phone that something didn’t seem right. The yard supervisor had driven into a nearby town to get some supplies and said he would come back to the yard and check out the situation. He arrived back at the feedlot approximately 20 to 30 minutes after the call.
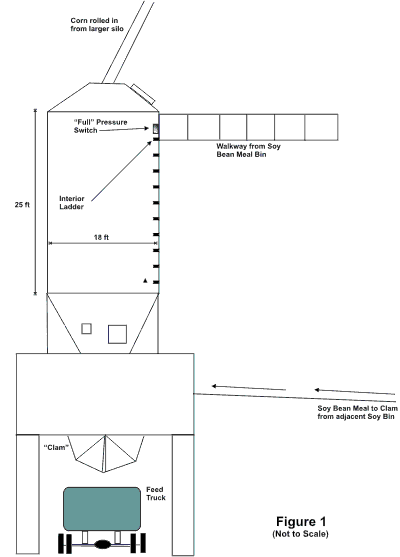
The yard supervisor immediately went up the stairs to the soy bean meal bin and the corn bin, which were side by side. He looked in the soy bean meal bin, which was the first bin he came to, and noticed that it had been “knocked down”. While he was looking in the soy bean meal bin he heard worker 1 yelling. He ran over to the corn bin and he saw the harness and rope on the walkway. He looked in the bin and saw worker 1 waist deep in the corn. Worker 1 told him that worker 2 was below him (buried in the corn). The yard supervisor then got the rope and threw it to worker 1. While this was happening the bin began emptying corn into the clam. He threw worker 1 the rope and he caught it but he couldn’t hold on, as he was being engulfed in the corn as a result of the bin emptying into the clam. At this point the yard supervisor came back down the steps and told the mill operator to shut everything down. Personnel immediately called emergency rescue personnel and individuals on site began efforts to extricate the two victims from the bin. The corn bin is a 6,000 bushel cone bottom gravity feed bin (see Figure 1). It was approximately half full at the time of the incident. Three holes were cut in the bottom of the bin. One was large enough to remove the victims and the two others were to allow the corn to flow out. The fire department arrived on the scene about the time the corn had finished flowing from the bin. Firemen went into the bin, through the hole that had been cut, scooped out some more corn and removed the victims. Neither victim could be resuscitated.
There were no witnesses to the incident and after interviewing coworkers and visiting the site it is this investigator’s opinion that the following is a probable scenario of the incident:
On the day prior to the incident both victims had been “knocking down” the soy bean meal in the soy bean bin. Sometime during the day their supervisor told them that the corn bin would need to be cleaned out before the weather gets too hot. The younger victim had never been in or cleaned out the corn bin before. It is probable that on the day of the incident, after “knocking down” the soy bean meal, the victims decided to look in the corn bin to see what was going to have to be done in regards to the cleaning. They probably opened the hatch (see Figure 1) to look into the bin. Corn was probably being rolled into the bin from the top causing the bin to be filled with dust, thus obscuring visibility in the bin. There is a pressure switch towards the top interior of the bin on the side wall near the ladder. Worker 1 knew if this switch was pressed the mill operator would think that the bin was full and he would shut off the corn being rolled into the bin. This would allow the dust to settle so they could see into the bin. It is probable that worker 2 leaned through the hatch to press the switch and lost his balance and fell into the bin. Worker 1 then probably entered the bin in an attempt to rescue worker 2. It is highly unlikely that they would have intentionally entered the bin, knowing that the bin was active and corn was flowing out approximately every 10 minutes. No one at the feedlot instructed the workers to enter the corn bin on the day of the incident and the workers did not inform anyone they were going to open the hatch to look in the bin.
CAUSE OF DEATH:
The cause of death, as stated on the death certificates, was suffocation for both individuals.
RECOMMENDATIONS/DISCUSSION:
Recommendation #1: Employers should ensure a permit is issued prior to entering bins.
Discussion: Had a permit been issued in accordance with CFR 1910.272(g)(1)(I), precautions should have been taken which could have prevented these fatalities. A permit was not issued for entry into either the soy bean meal bin or the corn bin.
Recommendation #2: Employers should ensure all equipment which presents a danger to employees is locked-out, blocked-off, or otherwise prevented from operating.
Discussion: In accordance with CFR 1910.272(g)(1)(ii), “All mechanical, electrical, hydraulic, and pneumatic equipment which presents a danger to employees inside grain storage structures shall be deenergized and shall be disconnected, locked-out and tagged, blocked-off, or otherwise prevented from operating by other equally effective means or methods.” When the victims were in the soy bean meal bin it was active, that is, it was emptying meal onto a conveyor which carried it to the clam under the corn bin. Also the corn bin was active and it was the flowing corn that engulfed the victims.
Recommendation #3: Employers should ensure employees are wearing appropriate fall protection anytime they enter a grain storage structure from a level at or above the level of stored grain products.
Discussion: Had proper fall protection been worn when entering the corn bin (assuming worker 2 went into the bin to press the pressure switch to stop the flow of corn into the bin) this could have prevented worker 2 from falling. Also, fall protection would have aided in the rescue of worker 2. 29 CFR 1910.272(g)(2) states in part, “Whenever an employee enters a grain storage structure from a level at or above the level of stored grain or grain products, or whenever an employee stands on or in stored grain of a depth which poses an engulfment hazard, the employer shall equip the employee with a body harness with lifeline, or a boatswain’s chair…” The bin was approximately half full of corn which posed a significant engulfment hazard. The bin was approximately 25 feet high and 18 feet in diameter.
Recommendation #4: Employers should provide and have in place equipment for rescue operations which is specifically suited for the task being conducted.
Discussion: According to 29 CFR 1910.272(g)(4), “The employer shall provide equipment for rescue operations which is specifically suited for the bin, silo, or tank being entered.” No equipment for rescue operations (such as a tripod with winch or a fixed or portable support arm with a winch). This company stated they had a support arm with a winch that slips into a channel for rescue operations at one of their other feed lots. Recommend rescue equipment such as this (or a tripod system) be procured for all locations requiring rescue equipment.
Recommendation #5: Employers should develop, implement and enforce a comprehensive safety program that includes, but is not limited to, training in all hazard recognition and abatement.
Discussion: A comprehensive safety program should have addressed the hazards associated with entering bins without a permit being issued. Had a permit been properly issued, areas such as lockout/tagout, fall protection, and rescue would have been addressed. NOTE: This company had bin entry procedures available but they were not being followed. Proper procedures must be implemented and consequences enforced for noncompliance.
Recommendation #6: Employers should consider installing locks on all accesses to bins and silos and controlling the keys to the locks.
Discussion: Installing locks on the hatches/doors to bins and silos and controlling access to the keys would help ensure that unauthorized access to bins and silos does not happen. Recommend locks be installed and only the yard supervisor and the feedlot manager be authorized to provide keys to workers. This would ensure that management knows where their employees are planning to work and they should notify the mill operator of planned entry into bins and silos so appropriate systems can be shut down prior to entry. Control of the keys MUST be maintained at the management level. Making extra copies of the keys to give to workers would totally defeat the intent of keeping the hatches/doors locked.
Recommendation #7: Employers should consider installing phones in close proximity to bins and silos which are normally entered, or providing workers entering bins and silos with cell phones or two-way radios to provide communications to the mill operator.
Discussion: Effective communications could have prevented these fatalities. Had a phone been available in the area of the soy bean mill and corn bins, the victims could have called the mill operator to let him know they intended to look in the corn bin. They could have asked him to stop the corn flowing into the bin so they could see into the bin. Furthermore, when worker 2 fell in the corn (assuming this is what happened), worker 1 could have immediately called the mill operator to shut down everything and call for help. Two-way radios (with a 2-mile range) are available from many sources for under $100 for two.
References:
Office of the Federal Register, National Archives and Records Administration, code of Federal Regulations, Labor, 29 CFR 1910.272, July 1998.
To contact Nebraska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.