
Hydrogen Sulfide Poisoning Kills Two
Nebraska Case Report: 96NE005
Report Release Date: March 22, 1996
Summary
A 30 year-old male (worker 1) and a 52 year-old male (worker 2) died as a result of exposure to hydrogen sulfide vapors. They were both working at an oil field water injection plant and in the process of replacing a water transfer pump when the incident occurred. It appears worker 1 removed a clamp on the wrong side of an isolation valve and water containing hydrogen sulfide (H2S) was released. Both were overcome by the H2S vapors. They were discovered by a coworker who called for help. They were pronounced dead at the scene.
The Nebraska Department of Labor (NDOL) Field Investigator concluded that to prevent future similar occurrences employers should:
- Develop, utilize and enforce a comprehensive 1ockout/tagout program to protect individuals from potentially hazardous conditions.
- Develop and utilize written standard procedures for removal and installation of major system components.
- Consider redesigning the ventilation systems in water injection plants to more effectively exhaust hydrogen sulfide vapors.
- Develop, implement and enforce a comprehensive safety program that includes, but is not limited to, training in all hazard recognition.
Program Objective
The goal of the workplace investigation is to prevent work-related deaths or injuries in the future by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact.
This report is generated and distributed solely for the purpose of providing current, relevant education to the community on methods to prevent occupational fatalities and injuries.
Introduction
On February 28, 1996, a 30 year-old male (worker 1) and a 52 year-old male (worker 2) oil field worker died as a result of exposure to hydrogen sulfide vapors. The Nebraska Department of Labor heard about the fatality from OSHA on February 29, 1996. The Nebraska FACE Investigator went to the incident site the morning of March 7, 1996, at which time the employer, an employee, and representatives from the company that owned the incident site, were interviewed.
The employer was a small construction company which employed three individuals at the time of the incident. The company had been in business for 18 years and these were their first fatalities. Although this company had been in business for 18 years they had only been involved in this type of work (oil field maintenance) for about six months. The company did not employ a full-time safety individual and although they had a limited written safety program they did not have written procedures for the task being performed at the time of the incident. When the incident occurred the victims were working inside a water injection plant (WTP) by themselves. There were no witnesses to the incident. The company that owns the WIP where the incident took place has also been in business for 18 years. At the time of the incident the company that had the fatalities was working as a sub-contractor to the company that owns the WIP.
Investigation
Worker 1 had been employed by the company for four months and worker 2 for five months. Worker 2 had been employed at this particular work site for the past two years but with a different employer. This incident took place at a water injection plant (WP) on an oil field.
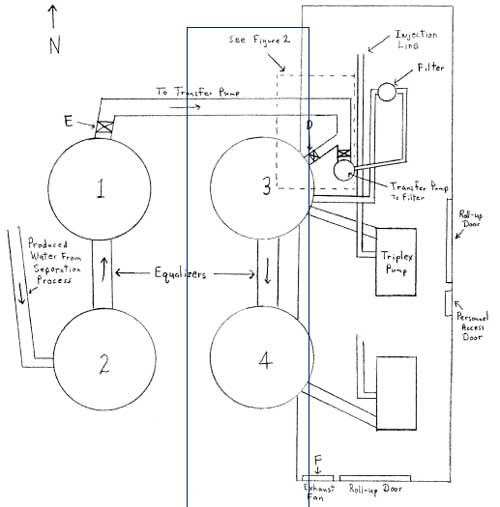
The WIP at which this incident occurred includes a building approximately 24′ x 60′ which houses pumps and piping. There are four 400 barrel water tanks outside the building as shown in figure 1. The purpose of the WIP is to inject water into oil wells to force out oil. The subsequent water and oil that is forced out of the wells is then separated. The water from the separation process is then recycled though the water injection plant, where it is filtered and injected back into the wells. The water used in this process sets up a natural growth environment for bacteria which excrete hydrogen sulfide. Hydrogen sulfide is a normal by-product of the separation process and the individuals working at the facility, with whom the investigator spoke, were well aware of the hazards associated with H2S.
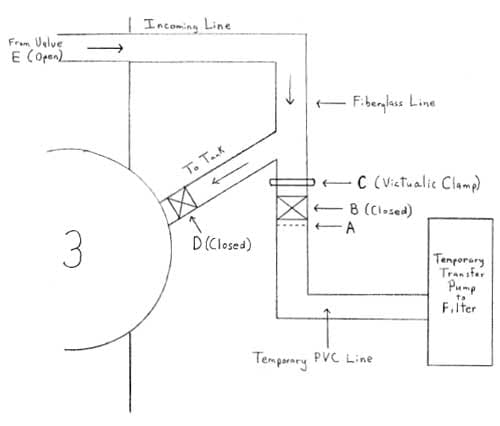
Workers 1 and 2 had been assigned the task of replacing a water transfer pump in the WIP. They were given a pre-task briefing by another employee (worker 3) of the company. Worker 3 advised workers 1 and 2 to cut the temporary PVC pipe (intended cut area indicated by A in figure 2) on the dead side of the valve (B in figure 2) in the WIP and hook up the pump to the dead side of the valve. There were no written procedures for ‘this operation. The temporary PVC pipe was used to install a temporary transfer pump until a replacement pump was ready. These same two workers had removed the original transfer pump and put in the PVC piping to the temporary transfer pump the week before.
figure 1 shows the normal setup with the permanent transfer pump installed. figure 2 shows the site setup at the time of the incident.
Worker 3 dropped workers I and 2 off at the WIP at approximately I :3Q pm.
From the physical evidence it appears worker 1 removed a victualic clamp (C on figure 2) on the live side of the valve which allowed water containing hydrogen sulfide to flow freely inside the building. The water was coming from a 400 barrel tank (tank 1 in figure 1) which was slightly over half full at the time of the incident. The pipe was three inches in diameter. From the position of the victims, it appears worker 1 was overcome by the H2S vapors and when worker 2 attempted to rescue him he was also overcome. Worker 3 had been working outside the water injection building and at approximately 5:15 pm went inside the building. When he opened the personnel access door to the building he could barely see because of the H2S vapor in the air. He opened the east overhead door to the WIP and when the vapors cleared he saw worker 2 slumped over some pipes and water running out of the pipe where the clamp had been removed. Worker 3 then ran outside the building to shut off the valve (E on tank 1 in figure 1) at the water tank which was allowing the water to flow inside the WIP. Valve D on tank 3 was in the closed position when worker 3 entered the building. We then returned to the building md pulled worker 2 to the east overhead door and opened the south overhead door. He called for an ambulance at approximately 5:30 pm and then tried to move worker 1 but was unable to lift the body. The ambulance arrived at the incident scene at 5:42 pm. Both workers were pronounced dead at the scene at 6:19 pm and the coroner’s report listed the time of death at approximately 5:10 pm.
Cause of Death
The cause of death, as stated in the coroner’s report, was accidental poisoning caused by hydrogen sulfide.
Recommendations/Discussion
Recommendation #1: Develop, utilize: and enforce a comprehensive lockout/ltagout program to protect individuals from potentially hazardous conditions.
Discussion: Had a lockout/tagout program been in effect for this particular operation, the shutoff valve on water tank 1 (E on figure 1) should have been shut off. Then, even though the water line was disconnected at the wrong place, the consequence should not have been fatal due to the fact that the water in the tank would not have been allowed to continue flowing into the water injection plant producing the hydrogen sulfide vapors. Also had the operation been performed property and the isolation valve (B in figure 1) had malfunctioned, having valve E (the valve closest to the water source) closed would have provided an extra margin of safety. Also the line from valve E to the pump should have been purged.
Recommendation #2: Develop and utilize standard written procedures for removal and installation of major system components,
Discussion: Written procedures to be followed when performing a pump removal/installation in the WIP should address areas that may have prevented these fatalities. The lockout/tagout procedure should be addressed which would include electrical as well as water isolation; specifics on where to cut/disconnect the water line; ventilation of the WIP; the hazards of hydrogen sulfide and what to do in the event of a release of toxic vapors and the use and availability of personal protective equipment. Worker 3 said it was normal procedure to have the large overhead doors in the WIP open when performing operations such as pump removal/installation. Had the doors been open it should have decreased the buildup of toxic vapors.
Recommendation #3 : Consider redesigning the ventilation systems in water injection plants to more effectively exhaust hydrogen sulfide vapors.
Discussion: The current ventilation system for this WIP is an electric exhaust fan mounted at the top of the south wall (F on figure 1). It is on a timer and runs for 15 minutes and then is off for 30 minutes. H2S vapors are 1.19 times heavier than air and therefore would build up at ground level. The addition of a floor mounted ventilation system would be more effective in removing H2S vapors. Also, when individuals are working in water injection plants the ventilation system should be in the constant operation mode.
Recommendation #4: Develop, implement and enforce a comprehensive safety program that includes, but is not limited to, training in all hazard recognition.
Discussion: A comprehensive safety program should have addressed all the hazards involved with the pump removal/installation procedures. Worker 1 should have been aware of the consequences of removing the clamp on a live water line. Scheduled and unscheduled safety inspections should be conducted by a competent person1 to ensure that job sites are free of hazardous conditions and to verify proper procedures are being followed.
1 Competent person: One who is capable of identifying existing and predictable hazards in the surrounding or working conditions which are unsanitary, hazardous, or dangerous to employees, and who has the authority to take prompt corrective measures to eliminate them.
Figures
|
|
|
Figure 2. Configuration at time of incident. (Not to scale)
|
The Nebraska Department of Labor, in conjunction with the National Institute for Occupational Safety and Health (NIOSH), conducts investigations on the causes of work-related fatalities. The goal of this program, known as Nebraska Fatality Assessment and Control Evaluation (NE FACE) is to reduce future traumatic occupational fatalities within the state of Nebraska. NE FACE plans to achieve this goal by identifying and studying the risk factors that contribute to workplace fatalities, by recommending intervention strategies, and by disseminating prevention information to employers and employees.
NIOSH funded state-based FACE Programs include: Alaska, California, Colorado, Indiana, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, Missouri, Nebraska, New Jersey, Wisconsin and Wyoming
To contact Nebraska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.