
Standup Forklift Operator Asphyxiated by Warning Chain
October 17, 2002
Nebraska FACE Investigation 02NE011
SUMMARY:
A 45-year-old forklift operator was killed when the standup forklift he had been operating ran into a steel link warning chain, pinning him against the Plexiglas mast shield. The victim had started his shift approximately 45 minutes earlier. He was responsible for moving frozen food products on pallets into and out of the ‘X’ freezer. This freezer was designated as the “withheld product Area” for product awaiting test results, etc. It is believed the victim placed a load into a bin, then backed out into the aisleway with the forks trailing, striking the steel chain. The chain had been placed there as a reminder to all operators that no Withheld Products were to be placed past that point. The chain came up over the back of the lift, catching the victim across the left side and back. The force pulled him off of the foot brake control and lift floor, pinning him chest first into the Plexiglas shield. Another worker noticed that they had not seen or heard the victim for several minutes and went to investigate, finding the victim pinned on the forklift. The employee ran for help while several more employees arrived on scene and tried to move the chain. The tension was too tight, bolt cutters were obtained and the chain was cut. The victim was removed and CPR was initiated by the company’s first responders. Emergency personnel arrived within minutes and the victim was taken to a local hospital where he was pronounced dead.
The Nebraska Workforce Development, Department of Labor’s Investigator concluded that to help prevent future similar occurrences, employers should:
- Ensure that warning devices themselves do not create a greater hazard.
- Develop, implement and enforce a forklift training program for all employees that may operate such equipment.
- Ensure that all equipment has an established maintenance program as recommended by the manufacturer.
- Develop, implement and enforce a comprehensive safety program that includes, but is not limited to, training in all hazard recognition.
PROGRAM OBJECTIVE:
The goal of the Fatality Assessment and Control Evaluation (FACE) workplace investigation is to prevent future work-related deaths or injuries, by a study of the working environment, the worker, the task the worker was performing, the tools the worker was using, and the role of management in controlling how these factors interact.
This report is generated and distributed solely for the purpose of providing current, relevant education to employers, their employees and the community on methods to prevent occupational fatalities and injuries.
INTRODUCTION:
On March 21, 2002, at approximately 10:45 a.m., a 45-year-old forklift operator died after the standup forklift he was operating contacted a steel link chain, pinning him against the Plexiglas mast shield of the forklift. The Nebraska Department of Labor was notified of the fatality the same day by the Occupational Safety and Health Administration (OSHA). The Nebraska FACE Investigator met with the investigating OSHA Compliance Officer (COSHA), company officials and employees on March 22 and 25-27 at the mishap location.
The victim’s employer is a multiple location frozen foods distribution company that has been in business for over 25 years. At the time of the mishap the company employed 29 employees at the incident location, including the victim. The company does have a written safety program and a full time safety consultant. All training given to employees was documented and those documents were provided for the investigation. The employer had no previous history of fatalities at this location.
INVESTIGATION:
Victim: The victim was a 45-year-old male. He had been employed by this company for over 24 years in two different locations, 14 years at the incident site. His primary job was to move frozen food product on pallets into and out of drive-in freezers.
Training: The victim had operated different types of forklifts during his employment with this company. He was qualified to operate motorized pallet jacks/dollies, sit-down Hysters and the stand-up Crown forklifts. Documentation provided by the company showed he had been formally trained using the National Safety Council’s forklift safety course in 1996, again in 1999 and was due to receive refresher training later this year. The company also supplemented that training with their own program which included videos specific to the Crown forklifts. Visual spot checks were also conducted by supervision.
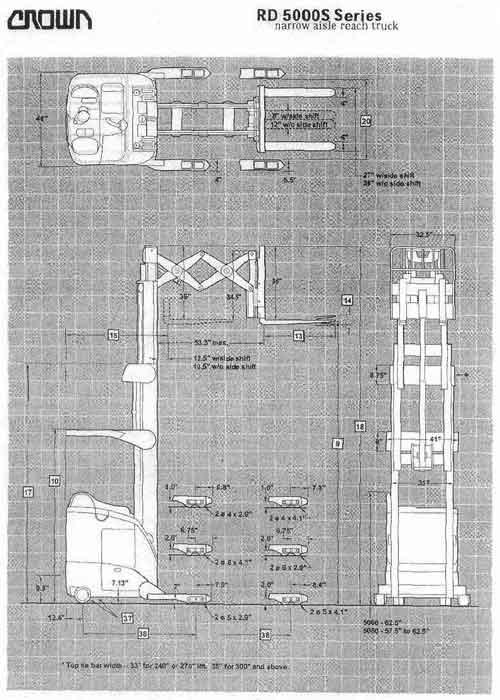
Equipment: The forklift is a Crown model RD Narrow-Aisle Rider. This particular forklift had been in use at the company since 1995 and was the forklift the victim normally operated. At the time of the incident it had 5,618 total usage hours. There were routine maintenance and daily pre-operational check off records on file including on from the day of the accident. These did not indicate any current mechanical problems with this forklift.
This forklift is designed to be operated from a side stance stand-up position. The operator’s right hand controls the multi-function control handle (joystick). This handle controls the travel direction and speed, all hydraulic functions, the horn and travel direction. Travel direction is determined by forward or backward movement of the handle. Neutral is in the center position. The handle is spring loaded to return automatically to the neutral position when released. Pushing the handle forward or away from the operator will move the forklift forward, or forks first. Pulling the handle back or toward the operator reverses travel. The further the handle is moved from the center neutral position, the faster the forklift will travel. The left hand operates the steering tiller arm. The forklift steers from the rear wheels and will pivot on the load wheels. The floorboard of the forklift is spring-loaded and designed to slope back, allowing the operator to comfortably rest against the padding on the inside. When stepping onto the spring-loaded floorboard, a switch is energized which turns on the power steering. That switch also allows the operator to operate the load handling functions of the truck. The brake pedal is also located on the floorboard. It works just the opposite of the way a car brake does. The operator applies the brakes by releasing the pedal, not by stepping down on it. If you quickly release the pedal, the braking will be hard. Gradually releasing the pedal will generate a slower but smoother stop. Travel can only be resumed by pushing the brake pedal to the floor.
Shortly after the incident the forklift was driven back to the maintenance area and locked out of service. The following day, March 22, 2002 representatives from FACE, OSHA, the victim’s employer, the building owner, the forklift servicing company and affected insurance companies met to determine what type of testing/teardown should be done to the forklift. Since the braking system was determined to be the most critical component at this time, it was decided to conduct braking tests using both the accident forklift and another identical model. ASME/ANSI standard B56.1-1993 requires this type of forklift to stop when traveling at full speed (5-7 mph) within a 6-foot distance. This distance is permanently marked in solid red lines along an aisle adjacent to the maintenance area. Crown operators are required to test the brakes as part of the pre-operational checklist. The company’s forklift mechanic conducted the tests with all representatives present, first with the accident forklift, then with a like machine. He would proceed at full speed down the aisle, cross the first red line, and release the foot pedal to activate the brakes. The following were the recorded distances, all within the required specifications:
| 1st | 2nd | 3rd | 4th | 5th | |
| Incident forklift #17 | 70” | 83” | 108 ¼” | 81 ½” | 88” |
| Forklift #10 | 65” | 50” | 55” | 69 ½” | 69 ½” |
Even though 4 out of the 5 tests conducted were “out of range”, this was attributed to the reaction time of the operator and where he released the pedal, not bad brakes. The incident forklift was then driven back to the maintenance area and again locked out-of-service. It was then determined by all present that a physical tear down of the brakes should be accomplished either by or with a third party present.
On March 27th all parties again assemble, joined by an independent mechanical engineer. The brakes are a hydraulically released, mechanically applied system. Both sets of brakes were torn down by a Crown certified mechanic exposing the hubs and brake shoes. No abnormalities were found. All appeared to be in operating shape.
Worksite: The incident occurred inside the ‘X’ freezer, a drive-in freezer at a cold storage locker facility which maintains a constant –15 Fahrenheit temperature. The floor is concrete, level and smooth. Overhead lighting is available and adequate. CFR 1910.178h standard states the minimum foot candles required for this storage area are 2 lumens/foot-candles. The OSHA Compliance Officer used a Weston Instruments Model 615 Illumination Meter to measure available lighting at the accident site. The following were the results:
At floor level = 16 foot candles.
At approximately 4’ high = 20 foot candles.
At approximately 6’6” high = 20 foot candles.
Chain: Chains have been used to isolate this and other company facility Withheld Product Areas since a directive was received from a government agency in 1983. Attempts to obtain a copy of this directive to see if chains were specific as the sold barrier media were not productive. The chain was moved to the current location approximately 1 ½ months ago from the rear of the aisle. It is constructed of ¼” stainless steel links, 128” in length and stretched across the aisle at a slight angle. It was wrapped and padlocked around the square shelf tubing on either side at a height of approx. 60 inches. The chain drooped in the middle to 34” above the floor level. It was placed at these heights to ensure it wasn’t a tripping hazard and to be visible to forklift operators. Attached in the middle was a metal sign approximately 12” by 10”, painted red with the words WITHHELD PRODUCT AREA in white capital letters. The key to this chain is kept in the Withheld Product Coordinator’s desk, outside of the freezer area on the loading dock. There are normally three chains across aisleways in the X freezer to essentially “box in” the Withheld Product Area: one across the entrance, one across a center aisle, and the other across the rear of the aisle where needed. At the time of the mishap, the entrance chain was down to allow access and the other two were in place. Employees interviewed stated they remember both plastic “crime scene tape” and plastic chain being used for short periods, but it was continually backed into and broke, so the stronger metal chain was used. Two employees indicated that they had become “entangled” in the metal chain on previous occasions. One received only a ripped coat, but the other had become pinned very similar to the victim. Although that operator was unable to move his right hand, he was able to work his left hand onto the joystick and slowly move the forklift back away from the chain. Neither of these two told their supervisors or other management personnel about the incidents.
ANALYSIS/SYNOPSIS:
On the morning of the accident the victim started his shift at 9:30 a.m. He went to the maintenance area and used the pre-operational check list to evaluate his forklift. He indicated on the checklist he conducted a brake test, but there were no witnesses to verify that. He proceeded to the ‘X’ freezer where he normally worked and began combining palletized frozen product in the Withheld Product Area, such as beef with other beef, chicken with other chicken, etc. After moving the product, a “location sheet” is filled out by the operator. The victim had filled his sheet out for some of his first product transfers, but had not filled it out for the task he was doing just prior to the accident. It is believed that he placed some pallets in a bin, then reversed the forklift out of the bin and into the aisle. He was traveling in reverse, with the forks trailing. Normally he would have turned towards the entrance of the freezer, but this time he turned towards the rear and the forklift made contact with the barrier chain. It is unknown how fast he was traveling, or if brakes were applied. It is believed that due to the height of the chain on the posts, the looseness/slack of the chain, the round rear shape of the forklift and the angle of the chain across the aisle, that the chain ”rode up” over the forklift as pressure was applied. It initially caught the operator across his left side, lifting him up off the floor board which would have applied the brake system. The pressure from the chain forced his shoulders and face flat against the Plexiglas mast shield. An employee mentioned that they had not seen the victim for a few minutes, so his supervisor went to locate him. As he approached from the center aisle, he saw the stopped forklift, but didn’t notice the victim. Upon closer examination he noticed the victim with his arms dangling at his sides and the chain across his shoulders. He ran outside the freezer to the dock area and told other employees to summon help. Six employees ran inside the ‘X’ freezer and attempted to remove the chain, but could not budge it due to the extreme tension. They yelled at the supervisor to get bolt cutter from the maintenance area while another employee summoned local rescue personnel. The bolt cutters were brought to the scene and the chain cut. The employees stated the chain had a “sling shot” effect when cut. The two company first responders lowered the victim to the floor and covered him with their coats. They started performing CPR and continued until the rescue personnel arrived. The victim was removed from the scene and taken to a local hospital where he was pronounced dead.
CAUSE OF DEATH:
According to the death certificate, the cause of death was Mechanical Asphyxiation.
RECOMMENDATIONS/DISCUSSION:
Recommendation #1: Ensure that warning devices themselves do not create a greater hazard.
Discussion: The sole intent of the “warning chain” was to let forklift operators know that this area was set aside from a specific reason, not to prevent employees from entering. The “withhold products” do have bright orange stickers which differentiate them from other product. Plastic “police tape” and plastic chain link were utilized in the past, but removed because they were being constantly broke. Employees indicated that they have backed into the steel chain on numerous occasions. This should have been an indicator that other methods should be tested and the safest used. ¼” steel chain link has a minimum vertical pull breaking point of 5000 lbs. It is recommended that an elastic cord (such as bungee cord) be utilized in lieu of a chain. This would not break during incidental contact, but should allow operators to know they had entered a restricted area. (CFR 1910.176(a) & Thomas J. Glover Pocket Reference, 2nd Edition, August 1998)
Recommendation #2: Employers should ensure that each powered truck operator is competent to operate a powered industrial truck safely.
Discussion: The victim had received formal training in the proper operation of the incident forklift from his current employer. He was up-to-date with all requirements. This training was given under the direct supervision of a person that had the knowledge, training and experience to train operators and evaluate their competence. This training consisted of a combination of formal instruction (e.g. lecture, discussion, interactive computer learning, video tape, written material), practical training (demonstrations performed by the trainer and practical exercises performed by the trainee) and evaluation of the operator’s performance in the workplace. This training included operating the forklift according to manufacturer’s specifications. (CFR 1910.178(l))
Recommendation #3: Employers should establish a routing maintenance program for all equipment to meet or exceed regulatory requirements.
Discussion: The employer had a well established maintenance program. This machine was examined prior to being placed in service at the beginning of every shift. Any time the exam showed any condition(s) adversely affecting the safety of the forklift, it was documented and the lift removed from service. Records for the accident forklift and all other company equipment were readily available during the investigation. (CFR 1910.178(q)(7))
Recommendation #4: Employers should provide a safe and healthful workplace, free from recognized hazards by developing, implementing and enforcing formal safety programs.
Discussion: The victim’s employer does have written, formal safety programs. Hazards associated with particular jobs were in writing, verbally discussed, and documented. The employer instructs each employee in the recognition, reporting procedures and avoidance of unsafe conditions and the regulations applicable to their work environment to control or eliminate any hazards or other exposure to illness or injury.
ATTACHMENTS:
|
|
|
Incident forklift specifications.
|
|

|
|
|
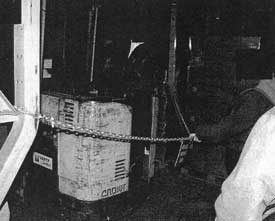
Two pictures taken showing incident chain in relationship to rear of forklift.
|
|
REFERENCES:
- Thomas J. Glover Pocket Reference, 2nd Edition, August 1998
- CROWN RR, RS and RD Training Guide for the Narrow-Aisle Rider
- American Society of Mechanical Engineers (ASME)/American National Standards Institute (ANSI) Standard B56.1-1993
To contact Nebraska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.