
Maintenance Technician Dies After Falling Eight Feet From Ladder
MN FACE Investigation 98MN06401
DATE: June 2, 1999
SUMMARY
A 51-year-old male maintenance technician (victim) died of injuries he sustained after he fell approximately eight feet at a food processing facility. The victim and a coworker were preparing to modify chemical lines in a room that contained liquid chemicals used to clean and sanitize food processing equipment. One end of a catwalk that was used to access service valves in the chemical lines was fastened to a wall of the room. The other end of the catwalk was supported by stainless steel framing resting on the floor. A fixed stainless steel ladder was fastened to the end of the catwalk to provide access to it. A stainless steel pipe was mounted horizontally near the ceiling of the room. The pipe was located 40 inches above the surface of the catwalk and 16 inches out or away from the top of the ladder.
The coworker briefly left the room to get a saw and other tools while the victim climbed the ladder to access the catwalk. When he neared the top of the ladder, he apparently struck his head on the stainless steel pipe mounted overhead. The collision with the pipe caused him to fall to the base of the ladder where he fell backward and sustained an injury to the back of his head. The coworker reentered the room and found the victim lying on the floor near the base of the ladder. On-site emergency medical personnel were immediately called to the scene. A call was placed to local emergency personnel who arrived at the scene shortly after being notified. They transported the victim to a nearby hospital for treatment. He was transferred to a major medical center where he died approximately five hours after the incident. MN FACE investigators concluded that, in order to reduce the likelihood of similar occurrences, employers should ensure that the following guidelines are implemented and followed:
- ensure all fixed ladders are designed and built in accordance with established safety standards and regulations;
- whenever possible, employers should provide stairs instead of ladders as a means of access to elevated work platforms;
- ensure employees wear appropriate head protection in all work areas; and
- ensure all elevated platforms are equipped with adequate guardrails.
INTRODUCTION
On December 4, 1998, MN FACE investigators were notified of a work-related fatality that occurred on December 2, 1998. On April 9, 1999, a site investigation was conducted by a MN FACE investigator. During MN FACE investigations, incident information is obtained from a variety of sources such as law enforcement agencies, county coroners and medical examiners, employers, coworkers and family members.
The employer associated with this incident is a large food processing facility. The food processing facility has been in operation in it’s present capacity since 1989. The number of employees at the location where the fatality occurred is in the range of 200-499 [1]. The company employs a full time safety manager who is responsible for administering the company’s comprehensive employee health and safety plans. All employees attend monthly general safety training and review sessions. During these sessions, employees watch videos that cover a variety of general topics related to employee safety and safe work procedures. Employees whose work exposes them to specific hazards such as confined spaces, etc. are given advanced safety training and periodic training updates that cover specific topics related to their work.
The victim had worked for the employer for approximately 19 months and was considered an experienced maintenance technician based on his current employment and on similar previous employment. This was the first work-related fatality that occurred at the company.
INVESTIGATION
On the day of the incident, the victim and a coworker were preparing to modify chemical lines in an area of the facility known as the Clean In Place (CIP) room. Located in the room were various tanks and drums containing cleaning chemicals that were used to clean and sanitize the equipment at the food processing facility. Located along one wall of the room were two 2100 gallon tanks that were used to store sodium hydroxide. Located between and slightly above the tops of the tanks was a stainless steel catwalk that was used to access service valves in the chemical lines (Figure 1). One end of the catwalk was fastened to the concrete block wall of the room. The other end of the 94 inch high catwalk was supported by steel framing setting on the floor of the CIP room. The sides of the catwalk were equipped with guard rails that had a top rail that was 37.25 inches above the surface of the catwalk. The guard rails however did not have mid-rails between the surface of the catwalk and the top of the guardrail.
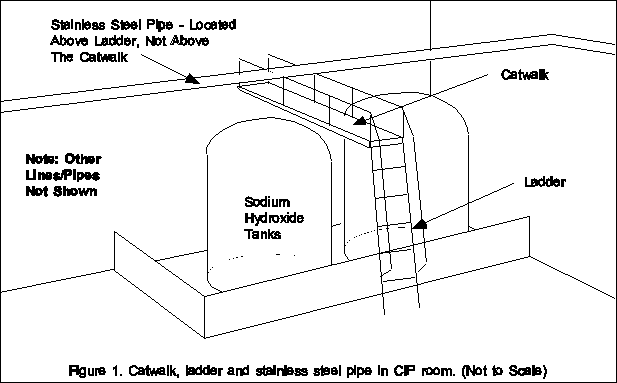
A fixed stainless steel ladder was fastened to the end of the catwalk to provide access to it. The ladder was not vertical but was inclined at an angle of 70 degrees when measured from the floor of the room to the back side of the ladder. The ladder was 24.5 inches wide and had five rungs that were 16 inches apart. The bottom rung was 31.25 inches above the floor. A 7 foot long handrail was fastened to one side of the ladder. A 2.5 inch diameter stainless steel pipe was located horizontally near the ceiling of the room. The pipe was located 40 inches above the surface of the catwalk and 16 inches out or away from the top of the ladder. The location of the steel pipe was nearly directly above the head of workers whenever they climbed the ladder.
The victim and the coworker entered the CIP room, reviewed the existing layout of several chemical lines and discussed the work associated with modifying the lines. The coworker had briefly left the room to get a saw and other tools when he heard a noise come from the room. He reentered the room shortly after leaving it and discovered the victim unconscious and lying on his back on the floor near the base of the ladder. On-site emergency medical personnel were immediately called to the scene. A call was placed to local emergency personnel who arrived at the scene shortly after being notified. They transported the victim to a nearby hospital for treatment. He was transferred to a major medical center where he died approximately five hours after the incident.
During the investigation, it was learned that the victim sustained blunt force injuries to both the top and the back of his head. Based on the location of the injuries and the configuration of equipment in the room, it is thought that the following scenario most probably occurred. The victim climbed the ladder to reach the catwalk after the coworker left the room. The 16 inch spacing of the ladder rungs may have caused the victim to exert greater force while ascending the ladder. When he neared the top of the ladder, he apparently struck the top of his head on the stainless steel pipe mounted overhead. The collision with the pipe caused him to fall to the base of the ladder where he apparently fell backward and sustained an injury to the back of his head.
Prior to the site visit conducted by the MN FACE investigator on April 9,1999, the employer had completed several safety improvements in the CIP room. The catwalk and stainless steel ladder associated with this incident had been disassembled and completely removed from the room. In addition, the service valves in the chemical lines that were near the top of the room and accessible from the catwalk were lowered so workers could reach them from the floor.
CAUSE OF DEATH
The cause of death listed on the death certificate was blunt force craniocerebral injuries due to fall from height.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Ensure all fixed ladders are designed and built in accordance with established safety standards and regulations.
Discussion The fixed stainless steel ladder that provided access to the catwalk was not designed and built in accordance with established safety standards and regulations. The ladder rung spacing of 16 inches exceeded by four inches the maximum allowed spacing of 12 inches for fixed ladders. In addition, the ladder did not have enough clearance on the climbing side as required in OSHA Standard 29 CFR Part 1910.27. Current OSHA regulations require that the perpendicular distance from the centerline of the rungs to the nearest permanent object on the climbing side of the ladder shall be at least 30 inches. In this case, a horizontally mounted stainless steel pipe was located 40 inches above the surface of the catwalk and 16 inches out or away from the top of the ladder. The location of the pipe was nearly directly above the head of workers whenever they climbed the ladder. If the ladder dimensions had been in compliance with established standards and if adequate clearance had existed on the climbing side of the ladder, this fatality probably would have been prevented.
Recommendation #2: Whenever possible, employers should provide stairs instead of ladders as a means of access to elevated work platforms.
Discussion: Workers are provided an added degree of safety whenever fixed industrial stairs are provided instead of ladders as a means of access to frequently used elevated work platforms. The use of fixed ladders designed, built and installed in accordance with established safety standards is acceptable, however the use of fixed industrial stairs may reduce the risk of injury to employees due to falls. All fixed industrial stairs should be designed, built and installed in accordance with OSHA Standard 29 CFR Part 1910.24 with regard to stair strength, width, angle of rise, treads, platforms, railings/handrails and vertical clearance. The existence of fixed stairs instead of the ladder that existed in this case may have prevented this fatality and it is recommended that whenever possible, employers provide stairs instead of ladders as a means of access to elevated work platforms.
Recommendation #3: Ensure employees wear appropriate head protection in all work areas.
Discussion: General industry employers such as the employer in this case should ensure that all employees wear appropriate head protection while working in or passing through all work areas. Head protection such as hard hats and bump hats are designed to prevent workers from being injured by falling objects or from striking their head against work place structures and machines. It is recommended that appropriate head protection, based on work tasks performed, be provided to and worn by all general industry employees. Since the occurrence of this incident, the employer now requires and enforces the wearing of appropriate head protection, hard hats or bump hats, throughout the food processing facility.
Recommendation #4: Ensure all elevated platforms are equipped with adequate guardrails.
Discussion: Although the guard rails on the stainless steel catwalk did not directly impact or contribute to the occurrence of this incident, the railings were not in compliance with established regulations. All elevated walking and work platforms should be equipped with guardrails that are not less than 36 inches or more than 42 inches high as required in OSHA Standard 29 CFR Part 1910.27. In addition, a mid-rail should be provided that is half way between the surface of the platform and the top of the guardrail. Although individual situations may prohibit the installation of guardrails that are higher that 36 inches, for an added degree of worker safety it is recommended that guardrails be 42 inches high whenever possible.
REFERENCES
1. Office of the Federal Register: Code of Federal Regulations, Labor, 29 CFR Part 1910.27 U.S. Department of Labor, Occupational Safety and Health Administration, Washington, D.C., July 1, 1998.
2. Office of the Federal Register: Code of Federal Regulations, Labor, 29 CFR Part 1910.24 U.S. Department of Labor, Occupational Safety and Health Administration, Washington, D.C., July 1, 1998.
[1] The following employment ranges, 1-4, 5-19, 20-49, 50-99, 100-199, 200-499, 500 or more are used to provide greater employer confidentiality.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.