
Worker Dies After Being Crushed By A Soft Drink Palletizer Lift
MN FACE Investigation 96MN02801
DATE: July 9, 1996
SUMMARY
A 42-year-old male industrial worker (the victim) died after being crushed by a soft drink palletizer lift. The palletizer fills pallets with cases of beverages. The palletizer’s rollers and turn tables are equipped with photo-electric sensors that cause the palletizer to automatically shut down if a light beam is broken. The hazardous areas of the palletizer are positioned behind safety screens. Access to the hazardous areas of the palletizer was possible by use of an interlocking gate, located near the lift section of the palletizer. If the gate was opened during operation, the palletizer would automatically shut down. Access was also possible by removal of two safety chains across an opening located near the beginning of the palletizer process.
At some point during the process, the palletizer shut down automatically. The victim investigated and discovered that a layer of cases had been deposited on a pallet, but the lift had not lowered it far enough for the next layer. He left the palletizer in the automatic mode, removed the safety chains, and climbed over the pallet conveyors to an area directly under the lift. The victim removed a piece of debris that had been blocking one of the photo-electric sensors and the lift immediately descended on top of him.
A coworker discovered the victim and called a company emergency response team. A 911 call was placed and emergency medical personnel responded. The victim was removed from underneath the lift and transported to a local hospital where he was pronounced dead. MN FACE investigators concluded that to reduce the likelihood of similar occurrences, the following guidelines should be followed:
- employers should ensure that employees access restricted production areas only by means of interlocking safety doors or gates;
- employers should ensure employees shut down equipment when they need to access restricted hazardous production areas; and
- employers should design, develop, and implement a comprehensive safety program.
INTRODUCTION
On March 26, 1996 MN FACE investigators were notified of a factory work-related fatality involving a 42 year-old male worker that occurred on March 22, 1996. During MN FACE investigations, incident information is obtained from a variety of sources such as law enforcement agencies, county coroners and medical examiners, employers, coworkers, and family members. A site investigation was conducted by MN FACE investigators on May 17, 1996.
The employer was a manufacturer of canned and bottled beverages that had been in business for 26 years. The company employed about 130 workers and had a safety officer on staff. The safety officer was responsible for safety programs and procedures. Employee training was conducted on-the-job. Only one other employee was present at the site at the time of the incident. The victim had worked for the employer for over 2 years and at the incident site for 18 months.
INVESTIGATION
The beverage manufacturing company produced soft drinks using automatic production equipment. The soft drinks were produced by mixing water with various flavored syrups. The beverages were automatically dispensed and sealed into cans or bottles. The cans or bottles were then packaged into cases. The cases moved along a conveyor belt to the section of production equipment the victim had been operating, known as a palletizer. The palletizer stacked cases of beverages onto pallets. It consisted of a pallet stacker, five series of rollers, a conveyor belt, a lift, a split table, two turn tables, and a wrapper (Figure 1).
Stacks of empty pallets were transported by forklift to the beginning of the palletizer process line. Individual empty pallets moved across a turntable and a series of rollers toward the palletizer lift. The lift raised the empty pallet approximately six feet and held it directly below a split table located at the end of the conveyor belt. Cases of soft drinks were transported to the end of the conveyor belt and were arranged to form one layer of cases for placement on the pallet. After the layer of cases was automatically pushed onto the split table, the split table opened and the cases dropped onto the pallet. The lift lowered layers of cases far enough to allow the split table to close as the next layer of cases was arranged. The filled pallet was transported by another series of rollers and a turn table to the wrapper. After the filled pallets were wrapped in cellophane they were transported by forklift to a warehouse area for shipment.
On the evening of the incident, the victim had been operating the palletizer for about two hours before he took a break. Although the palletizer operated automatically, it was the victim’s responsibility to make sure that there were no problems with the operation of the system. He used an industrial data terminal to monitor the progress of the palletizer. The industrial data terminal is a computer terminal that notifies the palletizer operator of any problems occurring with the palletizer. The conveyor belts and turn tables are equipped with photo-electric sensors that use light beams to indicate proper operation of the palletizer. The palletizer automatically shuts down if a light beam is broken due to an obstruction that was not a part of the production process. The hazardous areas of the palletizer were positioned behind safety chains and safety screens. An interlocking gate was located near the lift section of the palletizer. If the gate was opened during operation, the palletizer automatically shut down.
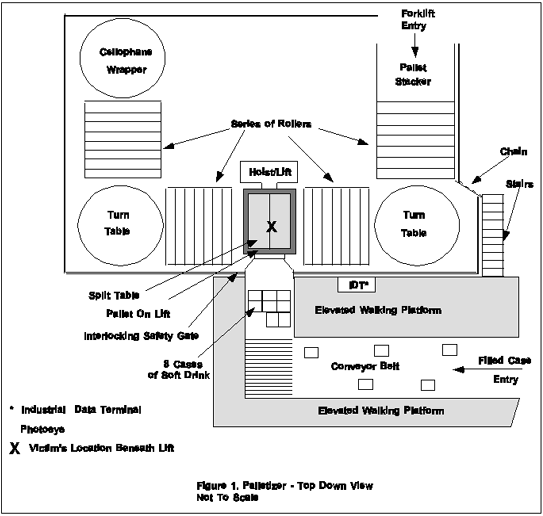
Sometime after the victim returned from his break the palletizer automatically shut down. The victim investigated and discovered that a layer of cases had been deposited on a pallet, but the lift had not lowered it through the split table. Apparently, a piece of cellophane had come off of the wrapper roll and formed a small ball which blocked a photo-electric sensor immediately downstream of the lift (Figure 1). He left the palletizer in the automatic mode, removed the safety chains, and climbed over the pallet conveyors to an area directly under the lift. The victim apparently removed the debris and the two thousand pound lift immediately descended on top of him. This occurred because once the condition that caused the lift to stop was corrected, the lift recycled to the lowest point of travel. As a result of the victim being under the lift, the lift jammed and was unable to lower completely. The motor eventually overloaded and the lift stayed in position on top of the victim.
The victim’s coworker, who was operating a forklift, drove to the palletizer to make sure it wasn’t backed up with full pallets. The forklift operator observed a red warning light flashing. He was not able to see the victim from the forklift. The forklift operator got off of the forklift and saw the victim under the pallet lift. He could see that the victim was pinned under the lift with one layer (10 cases) of beverage on top of the lift. He ran to the intercom and called for help which arrived within 2 minutes. A code red was announced over the intercom, which meant that a serious accident had occurred. A company emergency response team reported immediately. A 911 call was placed and emergency medical personnel responded. The victim was transported to a local hospital where he was pronounced dead.
CAUSE OF DEATH
The cause of death listed on the death certificate was traumatic asphyxiation .
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that employees access restricted production areas only by means of interlocking safety doors or gates.
Discussion: Modern production systems may have hazardous areas of operation that are restricted from employee access. However, due to equipment malfunction and maintenance, employees may need to enter these areas on occasion. When employees need to access such areas, they should be required to do so by means of interlocking safety doors or gates. Interlocking safety doors and gates are used to cause equipment to shut down when they are opened. In this incident, employees were separated from the hazardous areas of the palletizer by means of chains in one section and safety screens and an interlocking safety gate in the lift area. If the entire hazardous area had been restricted from employee access by means of safety screens and another interlocking safety gate the palletizer would have shut down when the victim entered the restricted area. With the palletizer shut down, the lift would not have descended on top of the victim, and this fatality may have been prevented. Since the incident occurred, the chains have been replaced by an interlocking safety gate.
Recommendation #2: Employers should ensure employees shut down equipment when they need to access restricted hazardous production areas.
Discussion: When hazardous areas of production equipment need to be accessed by employees, the equipment should be shut down prior to entry. Industrial production equipment often has an emergency stop device that will completely shut the equipment down. The emergency stop device should be designed to prevent the restart of the equipment until an employee activates a restart device located outside of the restricted area. In this case, when employees need to access the lift area of the palletizer, they should first activate the emergency stop button. If the emergency stop button had been activated before the victim entered the lift area, the lift would not have descended on top of the victim and this fatality may have been prevented.
Recommendation #3: Employers should design, develop, and implement a comprehensive safety program.
Discussion: Employers should ensure that all employees are trained to recognize and avoid hazardous work conditions. A comprehensive safety program should address all aspects of safety related to specific tasks that employees are required to perform. OSHA Standard 1926.21(b)(2) requires employers to “instruct each employee in the recognition and avoidance of unsafe conditions and the regulations applicable to his work environment to control or eliminate any hazards or other exposure to illness or injury.” Safety rules, regulations, and procedures should include the recognition and elimination of hazards associated with tasks performed by employees.
REFERENCES
1. Office of the Federal Register: Code of Federal Regulations, Labor, 29 CFR Part 1926.21 (b) (2), U.S. Department of Labor, Occupational Safety and Health Administration, Washington, D.C., July 1, 1994.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.