
Sawmill Foreman Dies of Injuries After Legs were Severed by a Saw Blade
MN FACE Investigation 95MN00501
DATE: June 9, 1995
SUMMARY
A 34-year-old male sawmill foreman (victim) died of injuries sustained after his legs were severed by a saw blade. The incident occurred at the location of a log home manufacturing facility while the victim and three co-workers performed a non-routine timber saw maintenance operation. The timber saw consisted of a four-foot diameter saw blade and a metal carriage used to hold and transport logs during the sawing operation. The carriage movement was controlled by a continuous cable system driven by a horizontal rotating drum located slightly forward of the saw blade. Drum rotation moved the carriage forward or backward along the carriage track-way.
On the day of the incident, the cable had shifted laterally off of the drum (travelled) during it’s use which required maintenance to re-install the cable. The procedure for cable re-installation required manual rotation of the saw blade while the drum transmission mechanism was activated. This allowed the drum to be rotated while the cable was guided back onto it. The victim and co-workers de-energized the saw and locked-out the main electrical power switch. The workers attempted to install the cable by turning the saw blade until the victim decided to reactivate power to the saw. The lock was removed from the main power switch, the electric motor started, and the drum transmission engaged allowing the drum to rotate. The victim positioned himself in the center of the carriage track-way and proceeded to guide the cable onto the drum. When the final portion of loose cable wrapped onto the drum, cable tension was re-established causing the drum to pull the carriage down the track-way towards the victim and saw blade. The victim attempted to move out of the carriage path but was contacted by the carriage which pushed the victim through the saw resulting in the amputation of the victim’s legs.
MN FACE investigators concluded that to reduce the likelihood of a similar incident, the following activities should be performed:
- prevent the carriage cable from travelling off of the drum;
- develop and enforce performance of approved maintenance and lock-out/tag-out procedures for cable re-installation;
- design the saw blade and cable drum to operate independently; and
- install emergency shut-off switches at locations where personnel may be expected to work or perform routine maintenance.
INTRODUCTION
On March 3, 1995, MN FACE investigators were notified of a machine-related fatality that occurred on February 27, 1995. The county sheriff’s department was contacted and releasable information was obtained. This information included photographs of the accident site, the initial complaint report, and the autopsy report. A site investigation was conducted by MN FACE investigators on March 15, 1995. During the site investigation, information concerning the incident was provided by an owner of the company employing the victim.
INVESTIGATION
The incident occurred at a log home manufacturing facility. The victim and three co-workers under his supervision had been preparing to perform a non-routine timber saw maintenance operation (performed approximately two to three times per year) following a mid-day break. The victim was a supervisor at the company; however, at the time of the incident the victim was working as the sawyer, a position for which he had been trained and was qualified to perform.
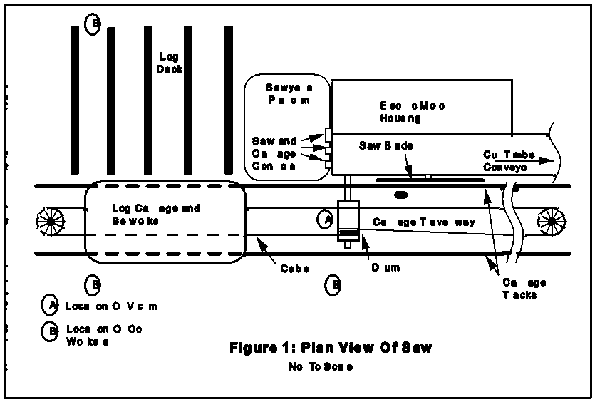
The timber saw consisted of a four-foot diameter saw blade and a metal carriage used to hold and transport logs during the sawing operation (see Figure 1). The carriage moved along the carriage track-way parallel to the saw blade on two tracks. The carriage is propelled by a continuous cable system driven by a horizontal rotating drum located between and below the tracks and slightly forward of the saw blade. A wire cable wrapped around the drum, traveled around pulleys located at either end of the carriage runway, and connected to both ends of the carriage. Rotation of the drum clockwise or counter-clockwise moved the carriage forward or backward along the carriage track-way. The drum was grooved to inhibit the cable from “traveling” horizontally on the drum. Both the saw blade and the drum were powered by one electric motor. The saw blade was directly linked to the motor and rotated when the motor was activated while rotation of the drum was controlled by a clutch which allowed the sawyer to control the speed and direction of drum rotation. Saw controls were located at the sawyer’s platform located forward of the saw and adjacent to the cable runway.
On the day of the incident, the cable had “traveled” off of the drum and required maintenance to re-install the cable. At this time the carriage was located five to six feet ahead of the saw blade. The victim and co-workers de-energized the saw and locked-out the main electrical power switch located approximately 50 feet from the sawyer’s platform. The Company lock-out procedure required each individual in the vicinity of the saw to place a lock on the power switch; however, only one lock was used by the workers during this maintenance operation. All workers had been trained to the Company lock-out procedure approximately one month prior to the incident.
The recommended procedure for cable re-installation required the pulleys to be loosened and the cable tension relieved. The cable would then be manually wrapped onto the drum and the pulleys adjusted to re-establish cable tension. A second, commonly utilized method involved the manual rotation of the saw blade while the drum transmission mechanism was activated. This allowed the saw blade and drum to turn in unison while the cable would be guided onto the drum.
The workers attempted to install the cable by manually turning the saw blade until the victim decided to reactivate power to the saw and use the electric motor to turn the drum while he guided the cable onto the drum. The single lock was removed from the main power switch, the electric motor started, and the drum transmission engaged allowing the drum to rotate. The victim positioned himself in the center of the carriage track-way between the rotating saw blade and the carriage and guided the cable onto the drum. At this time, one worker was located adjacent to the victim but outside of the carriage track-way, a second worker was near the carriage, and a third worker was loading logs onto the log deck.
When the final portion of loose cable wrapped onto the drum, cable tension was re-established causing the cable to pull the carriage, holding a log approximately 15 inches in diameter, down the track-way towards the victim and saw blade. The victim attempted to move out of the carriage path by moving toward the sawyer’s platform but was unable to clear himself. The worker adjacent to the victim moved away from the location while the worker located near the carriage attempted to manually restrain the carriage from moving forward. The log carriage contacted and pushed the victim through the saw. This resulted in the amputation of the victim’s legs.
Immediately following the incident, power to the saw was cut and assistance given to the victim. Emergency medical personnel were summoned to the site and the victim transported to a hospital where he died approximately one hour after arrival.
CAUSE OF DEATH
The cause of death stated in the autopsy report was exsanguination due to traumatic amputation of the legs.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Prevent the carriage cable from traveling off of the drum.
Discussion: Failure of the cable to remain on the drum resulted in the subsequent maintenance operation. Methods of preventing this occurrence include:
- Retrofit existing drums and redesign new drums to include raised edges on both ends of the drum to physically restrict the cable from lateral travel.
- Verify proper alignment of the cable on a routine basis. The drum and pulleys should be aligned to prevent the cable from traveling toward either edge of the drum.
- Install a spring on the pulleys or on the cable where it attaches to the carriage to maintain cable tension during carriage operation.
Recommendation #2: Develop and enforce performance of approved maintenance and lock-out/tag-out procedures for re-installing the cable.
Discussion: The recommended procedure for re-installation of the cable requires the cable tension to be relieved by loosening the pulleys, manually wrapping the cable onto the drum, and re-establishing cable tension by adjusting the pulleys. Some safety practices which could be incorporated into this procedure include:
- Prohibit employees from entering or working in the carriage track-way unless power, controls and/or equipment has been locked-out (see below)
- Position the carriage away from the location of the drum and in a location such that any carriage movement will be in a direction away from the saw blade
- Remove the saw blade whenever personnel will be required to perform maintenance work in it’s vicinity
Lock-out/tag-out of power, controls, and equipment needs to be incorporated into the procedure. Possible lock-out options include:
- Lock-out of electrical power
- Lock the carriage control lever in a neutral position
- Lock the carriage to either end of the track-way
Recommendation #3: Design the saw blade and cable drum to operate independently.
Discussion: Separate power sources or transmission mechanisms for both the saw arbor and the drum axle would allow each to be operated independently. During maintenance operations, power to the saw blade could be disengaged while still allowing the drum to be rotated and the carriage moved.
Recommendation #4: Install emergency shut-off switches at locations where personnel may be expected to work or perform routine maintenance.
Discussion: Emergency shut-off switches installed at various locations would allow immediate shut-down of equipment from areas other than the sawyer’s platform. Power to the saw was controlled by two switches: the main power switch and the control at the sawyer’s platform. However, the operation and size of the saw (approximately 50 feet in length) requires personnel to work at locations away from these switches. Emergency shut-off switches should be easily accessible by being of sufficient size, not recessed, and uncovered.
REFERENCES
- Safety Suggestions for Sawmill Operators, Employers Mutuals of Wausau, Wausau, Wisconsin.
- Sawmill Head Rigs – Data Sheet 460, National Safety Council, Chicago, Illinois.
- Health and Safety Guide for Sawmills and Planing Mills, 1977, National Institute for Occupational Safety and Health.
- Milton, Dr. Thomas, Ph.D., (Interview) Extension Specialist and Associate Professor, Department of Forest Products, University of Minnesota, Minneapolis, Minnesota.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.