
Male Machinist Dies After Falling From the Top of a Disc Screen Machine
Minnesota FACE 93MN004
SUMMARY
A 60-year-old male machinist (victim) died of injuries he received after falling from the top of a disc screen machine, through a discharge chute, and onto a conveyor 18 feet below. He was working with four others on a project which involved removing disc screen rollers from four identical machines for disc space modification. They were working on the third machine when the incident occurred; it was not operational at this time. Machine housing assemblies were removed to expose the roller deck. This process also exposed a 5 x 10-foot discharge chute opening at the end of the deck. Modification work was taking place on the deck so the workers constructed a catch platform over the opening to prevent falling into it. Six 2 x 4’s, which served as platform supports, rested on the machine frame on one side of the opening and were wedged between a metal pipe brace and the last disc screen roller on the other side. A 4 x 8-foot, ¾-inch board was placed on top of the 2 x 4’s to cover the opening. None of the platform components were secured to the machine or to each other. When the roller holding the 2 x 4’s in place was removed from its deck position for modification, the compression it provided on them was relieved. The victim stepped onto the platform at this point and the entire structure collapsed into the discharge chute opening. He fell approximately 18 feet to the conveyor below and died approximately ten weeks later of his injuries. MN FACE investigators concluded that, in order to prevent similar occurrences, the following guidelines should be followed:
- temporary platforms used to prevent falls into holes should be secured against accidental displacement; and
- employers should provide training for workers in hazard recognition and avoidance, and safe work policies including task specific procedures.
INTRODUCTION
On March 23, 1993, MN FACE personnel were notified of a November 3, 1993, work-related fall that resulted in death on January 16, 1993. MN OSHA was contacted and the incident report was requested. The president of the company employing the victim was interviewed by telephone. A site investigation was conducted at the plant where the incident occurred on April 8, 1993.
The victim worked as a machinist for a small engineering and manufacturing company whose main enterprise was hydraulics, machine shop, and steel fabricating. The company had been hired as an outside contractor to modify four identical machines in a local lumber plant during a plant shutdown. The victim, two other employees, and one plant employee completed work on the first two machines during the week prior to the incident. A service technician for the machine manufacturer joined them soon after work on the third machine began. The platform had, at that time, already been installed. The incident occurred near the end of the second day of work on this machine.
INVESTIGATION
Five workers were making modifications to the disc screen rollers of a large three-story high machine used to separate long pieces of wood from short pieces. Rollers were approximately 10 feet long with discs evenly spaced along their lengths; disc spacing was adjustable so, at any given time, various sized wood pieces could be screened. The machine’s roller deck consisted of 20 of these one-ton disc screen rollers. The motor driven rollers were stationary on the deck but rotated in place at high speed. As the rollers rotated, the discs acted as filters, or screens, to separate different sized wood pieces. The rollers were situated over one discharge chute (#1) and ended at another final discharge chute (#2). Short pieces of wood were deposited into chute #1, and long pieces of wood were deposited into chute #2. Separate conveyors, 18 feet below the roller deck, received these products. See Figure 1.
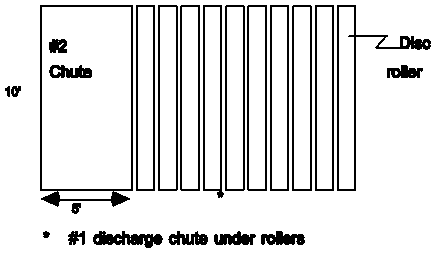
Figure 1. Overhead view of roller deck and #2 discharge chute opening.
The job consisted of hoisting each roller from its deck position with a crane, placing it on boards placed on top of rollers still in position on the deck, modifying its disc spacing, and finally reinstalling it into its original position. This process proceeded from the input end of the machine to the output (#2 discharge chute) end.
To expose the roller deck, upper housing assemblies at the third level of the machine were removed. This process also exposed the 5 x 10-foot #2 discharge chute opening at the output end of the machine. The workers, who were working on the roller deck level, constructed a catch platform over the discharge chute opening to prevent falling into it. Six 2 x 4’s, evenly spaced, spanned the 5-foot wide opening. They were supported on one side of the opening by the frame of the machine. They were wedged under the last roller of the machine and a metal pipe brace beneath it on the opposite side of the opening. A slight downward angle toward the machine frame caused jamming of the 2 x 4’s beneath the roller and helped hold the boards in place. A 4 x 8-foot, ¾-inch thick board was laid over the 2 x 4’s to cover the opening. The platform components were in no way secured to the machine or to each other. After platform construction, work continued for the day without incident.
The next morning, the same five people resumed work on the machine. The last roller was eventually removed for modification near the end of the day. This action relieved the compression on the 2 x 4 boards which was, in large part, holding the platform in place. The victim walked onto the platform at this point and it slid downward on its resting points on the machine’s outer frame, allowing the 2 x 4 ends resting on the metal pipe brace to drop off. The entire structure and the victim fell 18 feet to the conveyor below. It is probable, from witnesses accounts, that the victim hit his head on the pipe brace as he fell; he was unconscious and sustained various broken bones after the fall.
Plant emergency personnel responded and an ambulance was dispatched. Covers surrounding the collector conveyor were removed and medical treatment initiated. After arrival of the ambulance, he was removed from the conveyor, transferred to a hospital, and subsequently underwent surgery for internal injury. He remained in a coma for about ten weeks before dying from his injuries.
CAUSE OF DEATH
The cause of death listed on the death certificate was complications of multiple blunt force head, chest, and upper extremity injuries due to or as a consequence of a fall.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Temporary platforms used to prevent falls into holes should be secured against accidental displacement.
Discussion: Covers over holes should be strong enough to support the maximum intended load. They should also be installed and adequately secured to prevent accidental displacement. Under the existing conditions, constructing a catch platform over the #2 discharge chute opening was a reasonable protective measure to implement. Failure to adequately secure the platform, however, was a factor that may have contributed to this fatality.
If it was not possible to secure the platform to the machine frame, other options to cover the chute opening could have been considered. A viable option was used during modification of the fourth machine, after the incident occurred. Housing assemblies over the #2 chute opening were left in place, and boards were bolted over openings where falling into the opening was still possible. This solution greatly reduced the potential for a fall to occur. In addition, even though a catch platform is an intermittent and temporarily required structure, permanent fixtures or attachment points could be installed on machines for securing a temporary platform if adjustment is necessary in the future.
Recommendation #2: Employers should provide training for workers in hazard recognition and avoidance, and safe work policies including task specific procedures.
Discussion: The need for some type of fall protection while performing disc modification was obviously recognized because the catch platform was designed and installed. However, securing it against displacement, even though it was not intended as a work platform, was necessary to provide fall protection. Employers should ensure that employees have been adequately trained to recognize and avoid unsafe work conditions. Measures employees should take to protect themselves from work-related hazards during task specific procedures should be included as part of employee training.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.