
Paper Mill Maintenance Employee Dies After Being Pinned By The Arm Of A Control Mechanism In A Roll Wrap Machine
MN FACE Investigation 03MN039
Date: September 23, 2004
SUMMARY
A 47-year-old male employee died after he was injured in a roll wrapper machine at a paper mill. The operator of the wrapper had contacted maintenance because the wrapper was not cycling. A mechanic who responded determined that there was not a mechanical problem so he called the Electrical & Instrumentation (E&I) Technicians.
Three E&I Technicians responded and began to troubleshoot the wrapper. While troubleshooting the system, the wrapper was left in its operational mode, a normal procedure since it would be nearly impossible to determine the problem if the system were shut down. After troubleshooting the wrapper, it was suggested that it be cleared of all rolls of paper and the system be shut down and rebooted to reset it. While the E&I Technicians were troubleshooting the system, operations personnel were reviewing the lockout/tagout procedures for the wrapper.
After the system was rebooted, one roll of paper was transferred to the first of two roll stop positions. The roll stop again failed to release the roll. Without notifying any of his co-workers, the victim went to the side of the wrapper opposite the computer control room. He crawled under the wrapper platform apparently to look for a switch called the ejector down switch. The switch senses the position of the wrapper’s two roll stops and either allows or prevents rolls from moving across the wrapper platform. A diagram in the computer control room clearly indicated that the switch was located outside the wrapper frame.
A steel plate that activates the ejector down switch is located beneath and near the center of the wrapper. The victim apparently proceeded to look in the area underneath and near the center of the wrapper. While he attempted to locate the switch, he was eventually guided by following the switch arm to the switch location on the outside of the wrapper frame. After locating the switch, he put his upper body through an opening in the side of the wrapper such that his torso was above the roll wrapper frame and directly below a raised control arm for one of the roll stoppers. A co-worker who happened to walk around the wrapper saw the victim at the moment he reached up and struck the switch with his fist. When the switch was struck, the wrapper immediately cycled.
When the wrapper started, the roll of paper was released and it rolled forward to the raised bumper that was above the victim. The bumper descended as the roll came against it and crushed the victim between the wrapper frame and the bumper arm.
A call was immediately made to emergency personnel who responded to the scene. The victim’s co-workers immediately began to try to free the victim. He was eventually freed and removed however he had sustained traumatic crushing injures and was pronounced dead at the scene. MN FACE investigators concluded that, in order to reduce the likelihood of similar occurrences, the following guidelines should be followed:
- employers should ensure that employees access restricted “areas” only by means of interlocking safety doors or gates.
- employers should ensure that employees shut down and lockout/tagout equipment before they enter any restricted hazardous areas.
- employers should securely install permanent barriers on all non-essential equipment “openings” that may pose a hazard risk to employees, and;
- employers should continuously stress the importance of strict adherence by all employees to established safe work procedures.
INTRODUCTION
On November 12, 2003, MN FACE investigators were notified of a work-related fatality that occurred on November 11, 2003. A site investigation was conducted by a MN FACE investigator on April 19, 2004. During the site investigation, the employer’s safety manager was interviewed. During MN FACE investigations, incident information is obtained from a variety of sources such as law enforcement agencies, county coroners and medical examiners, employers, coworkers and family members.
The victim’s employer is a Minnesota paper pulp and fine paper mill that is part of a global company located on several continents. The North American division is a major producer of high quality coated paper with an annual capacity well in excess of one million tons per year from several paper mills. The Minnesota mill was established and built in 1898 and began operation as a mill that produced paper for news print. Chemical paper pulping was added to the facilities about twenty years later. During the 1960’s, the mill began to produce a variety of high-grade coated papers to meet the expanding and changing needs for paper suited to modern printing processes. The mill was acquired by the global paper company shortly after expansion and equipment modernization in 2002 more than doubled its previous production capacity.
The local facility has two primary production components or operations. Its initial operation results in the production of bleached paper pulp from logs brought to the mill. The paper pulp that is produced is primarily for its own use in the production of paper although a small portion of it is sold to other paper producers. Its second operation is the production of fine printing paper that is produced from the bleached paper pulp. The mills annual production capacities are in excess of 400,000 tons of paper pulp and in excess of 225,000 tons of fine printing paper.
The victim was an Electrical & Instrumentation Technician who had been employed by his current employer for 14 years, 12.5 years while the company was owned by its previous owner and 1.5 years since the company was purchased by its current owner. He was one of twelve company employees with this job title. Their job responsibilities were to perform electrical and instrumentation maintenance and repair on all equipment that was associated with the production of paper.
The mill where the incident occurred has a total of approximately 760 employees working in all areas from plant management to actual paper production. Paper production occurs continuously 24 hours per day and seven days per week. The actual paper production portion of the mill employs approximately 70 employees per 12 hour work shift. Employees in the paper production area work 12 hour shifts and typically are scheduled to work four consecutive days followed by four days off.
The employer has a complete and comprehensive written safety program that includes both formal and hands on training for all production employees. This extensive program has been developed, maintained and is continually updated in an effort to insure that it remains in total compliance with and either meets or exceeds all government established safety regulations and standards.
INVESTIGATION
The machine associated with this incident was a machine called a roll wrapper. It is located after the paper production line and is used to wrap large rolls of finished paper with a brown wrapping paper to protect them during storage and shipment to end-users. The paper mill has only one roll wrapper. The finished rolls of paper vary in size but generally are approximately 44 inches in diameter, approximately 50 inches long and weigh approximately 750 pounds.
The roll wrapper is a computer-controlled machine that has an operator station at which an operator is stationed to monitor the operation of the wrapper. The wrapper has an elevated platform that is approximately 30 inches above the floor. Finished rolls of paper arrive from the production area via a conveyor and slowly roll onto the wrapper platform. The wrapper has three positions at which each roll of paper stops as it moves through the wrapping process. The first two stations are equipped with a device known as a bumper that stops each roll in the proper position while the wrapper performs certain functions.
The first position on the wrapper platform where each roll of paper stops is known as the #206 roll stop. At this position each roll of paper is weighed. The second position on the wrapper platform is known as the #210 roll stop and is shown in Figure 1. At this position the length and diameter of each roll is measured and the roll is properly positioned horizontally or along the length of the roll for wrapping. Proper positioning is necessary to ensure that the roll is centered as it rolls into the final position of the wrapper where the roll is wrapped with protective paper. After each roll is wrapped, the rolls are automatically moved off the wrapper to a storage and handling area from which they are shipped to customers.
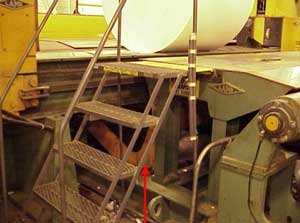 |
| Figure 1. Roll stop bumper #210. The E&I Technician was positioned with his head and shoulders to the outside of the machine frame and lower body to the inside underneath the orange roll stop arm which can be seen behind the stairs. |
The three positions of the roll wrapper are sequenced positions such that up to three rolls of paper can be on the platform at the same time. The rolls of paper, when in the first two positions, the #206 roll stop and the #210 roll stop are held in place by devices known as roll stop bumpers. The bumpers are mounted beneath the roll wrap machine platform. The ends of the bumper arms are connected at a pivot point located beneath the platform. The pivot points enable the bumpers to move up and down through long narrow openings or spaces in the roll wrap machine platform. When three rolls of paper are on the roll wrap platform, one roll is being wrapped, the roll at the #210 roll stop is being measured and properly positioned to be wrapped next and the roll at the #206 roll stop is being weighed. After the roll in the wrapping position is wrapped, the wrap machine automatically removes it from the platform by moving it perpendicular to the direction that the rolls travel across the platform.
After a wrapped roll of paper is removed from the wrapping platform, the #210 and the #206 roll stop bumpers operate in sequence to advance the next two rolls. The #210 stop bumper first recedes to its lowered position beneath the wrapper platform and allows the next roll of paper to roll forward to the wrapping position. The #210 roll stop bumper then moves to its raised position while the #206 roll stop simultaneously lowers and allows the roll that was at the #206 stop to move to the #210 stop position. After the roll of paper that was held at the #206 stop bumper moves to the #210 stop bumper, a new roll of paper rolls onto the platform and is stopped at the #206 stop position and the wrap machine again performs the necessary functions at all three positions.
On the day of the incident, the operator of the roll wrapper contacted shift maintenance regarding a problem at the #206 roll stop position which is where rolls of paper are measured and properly positioned for wrapping. The shift mechanic who responded to the call determined that the malfunction was not a mechanical problem so he called the Electrical & Instrumentation (E&I) Technicians.
Three E&I Technicians, including the victim responded and arrived at the roll wrapper where they began to troubleshoot the problem. While troubleshooting the system, the roll wrapper system remained in its operational mode and the technicians moved between the computer control system and the two roll stops of the wrapper in an attempt to determine why it would not properly cycle. After some time troubleshooting the wrapper, one of the E&I Technicians suggested that the wrapper be cleared of all existing rolls of paper and the entire wrapping system be shut down and rebooted to reset the system. While the E&I Technicians were troubleshooting the system, operations personnel were reviewing the lockout/tagout procedures for the wrapper.
After the computer system was rebooted and the roll wrapper restarted, one roll of paper was transferred to the first position, the #206 roll stop. The #206 roll stop again failed to release the roll and allow it to move to the #210 roll stop position. The E&I technicians again reviewed the logic in the computer control system in an attempt to identify the problem. The victim then suggested that the problem might be associated with one of several control switches that sense the position of the roll stops and control the movement of rolls through the wrapper.
The victim did not indicate to his co-workers which specific switch might be causing the problem. Without notifying any of them, he went to the side of the wrapper opposite the computer control room and descended the steel stairs shown in Figure 1. He then crawled under the wrapper platform apparently to look for a switch called the ejector down switch. The ejector down switch senses the position of the two roll stops and either allows rolls to move or prevents them from moving across the wrapper platform. A diagram in the computer control room clearly indicated that the ejector down switch was located outside the wrapper frame.
A steel plate that activates the ejector down switch is located beneath and near the center of the wrapper. The victim apparently proceeded to look in the area underneath and near the center of the wrapper. While he attempted to locate the switch, he was eventually guided by following the switch arm to the switch location on the outside of the wrapper frame. After locating the switch, he put his upper body through an opening in the side of the wrapper shown in Figure 2 such that his torso was above the roll wrapper frame and directly below a raised control arm for one of the roll stoppers. A co-worker who happened to walk around the wrapper saw the victim at the moment he reached up and struck the switch with his fist. When the switch was struck, the wrapper immediately cycled.
 |
| Figure 2. Roll stop bumper #210, bumper in raised position. Same as Figure 1 except with the stairs removed to more clearly show incident site and the roll stop in relation to the machine frame. |
When the wrapper started and began to cycle, the roll of paper that was at the #206 stop position was released and it rolled forward to the #210 roll stop bumper. The #210 roll stop bumper descended nearly all the way as the roll came against it. When it descended, the victim was crushed between the wrapper frame and the large arm of the bumper as the bumper lowered.
After the incident occurred, a call was immediately made to emergency personnel who responded to the scene and arrived shortly after being notified. The victim’s co-workers immediately began to try to free the victim. In order to free and remove him, the wrapper had to be shut down and the roll of paper that was now against the #210 stop bumper had to be manually rolled back and away from the bumper in order for the bumper to be manually raised. The victim was eventually freed and removed however he had sustained traumatic crushing injures and was pronounced dead at the scene.
CAUSE OF DEATH
The cause of death on the death certificate was suffocation due to mechanical compression.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that employees access restricted “areas” only by means of interlocking safety doors or gates.
Discussion: Modern production systems may have hazardous areas of operation that are restricted from employee access. However, due to equipment malfunction and maintenance, employees may need to enter these areas on occasion. When employees need to access such areas, they should be required to do so by means of interlocking safety doors or gates. Interlocking safety doors and gates can be used to cause equipment to shut down when they are opened. In this incident, there were no barriers to prevent employees from crawling under the wrapper platform while it remained in its operational mode. If the area under the wrapper platform had been restricted from employee access by means of safety screens and interlocking safety gates, the wrapper would have shut down when the victim crawled under the platform. With the wrapper shut down, it would not have started and the bumper arm would not have descended on the victim and this fatality probably would have been prevented.
Recommendation #2: Employers should ensure that employees shut down and lockout/tag out equipment before they enter any restricted hazardous areas.
Discussion: When hazardous areas of production equipment need to be accessed by employees, the equipment should be shut down and locked out/tagged out prior to entry. In this instant, the computerized nature of the roll wrapper required that it remain in its operational mode while the technicians attempted to determine why the wrapper would not properly cycle. After the technicians determined that there might be a problem with a control sensor, the wrapper should have been shut down and locked out/tagged out before the victim crawled under the wrapper platform and attempted to locate the switch that was causing the problem. If proper lockout out/tag out procedures had been followed following the technicians troubleshooting efforts but before the victim began to look for the ejector down sensor, this fatality probably would have been prevented.
Recommendation #3: Employers should securely install permanent barriers on all non-essential equipment “openings” that may pose a hazard risk to employees.
Discussion: The large opening in the frame of the roll wrapper is a non-essential opening in that it is not necessary for it to be unguarded for the machine to properly operate. However, the up and down movement of the bumper stop arm creates a dangerous pinch point for anyone or anything that enters the opening. Since the opening is a non-essential opening, a permanent rigid guard or plate should be securely bolted to the frame of the roll wrapper to prevent workers from reaching through the opening or positioning themselves in the opening as happened in this incident. If this opening and all similar non-essential openings had been covered with rigid grates or guards, the victim could not have positioned himself where he did and this fatality probably would have been prevented.
Recommendation #4: Employers should continuously stress the importance of strict adherence by all employees to established safe work procedures.
Discussion: The employer has a complete and comprehensive written safety program that includes both formal and hands on training for all employees. As previously stated, this program has been developed, maintained and is continually updated in an effort to insure that it remains in total compliance with and either meets or exceeds all government established safety regulations and standards. Effective safe work procedures required that all employees adhere to all established safe work procedures at all times. Employers should continuously stress the importance of strict adherence by all employees to established safe work procedures and should routinely monitor employees in an effort to ensure employees adhere to all established procedures.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.