
Worker Dies After Being Crushed Between Rock Spreader And Pneumatic Roller in Minnesota
MN FACE Investigation 00MN03001
DATE: April 25, 2001
SUMMARY
A 36-year-old male worker (victim) died of injuries he sustained when he was pinned between a pneumatic roller and a rock spreader. On the day of the incident he was working as a member of a road resurfacing crew. His employer had been contracted to apply a surface seal coat to 16 miles of paved road. The seal coat consisted of liquid asphalt sprayed on the road and crushed rock spread over the liquid asphalt. Equipment involved in this incident included a rock spreader and a pneumatic roller. The spreader had a computer rate control (CRC) unit that controlled the rate of application of crushed rock. The roller was a nine-wheel pneumatic roller equipped with hydraulic brakes that were activated via a foot pedal. The unit was also equipped with a hand operated emergency brake.
The workers began by applying a layer of seal coat to a “test area” of the road. A liquid asphalt tankers was used to spray liquid asphalt to the test area. A dump truck filled with chipped rock was backed up to the rock spreader. The spreader operator drove the spreader forward pushing the gravel truck across the test area. After crossing the test area, the workers realized that the layer of crushed rock coming from the spreader was not uniform. The spreader operator disengaged the unit and backed it off the test area. After the operator parked the spreader, he dismounted and walked to the front of the unit to a computer control panel. While he attempted to determine what was wrong with the CRC unit, an operator of a pneumatic roller packed the rocks that had been spread over the test area.
The operator drove his roller onto the test area with the unit facing away from the parked spreader. Due to the incline of the road the roller traveled up a slight incline and was backed down the incline as the operator packed the seal coat in the test area. As the operator approached the end of the test area near the parked spreader, the roller’s manual transmission slipped out of gear and the roller began to roll toward the spreader. The operator stepped on the hydraulic brake foot pedal but was unable to stop the roller. He attempted to pull the emergency brake while he also yelled to workers to clear the area. Other workers ran from the area however the victim apparently did not hear the call to clear the area. The victim was crushed when the roller struck the front of the spreader.
The roller operator immediately shifted it into gear and drove the roller forward. The victim fell to the ground and other workers immediately placed a call to emergency personnel. Emergency personnel arrived at the scene shortly after being notified. They transported the victim to a local hospital where he died shortly after he arrived. MN FACE investigators concluded that, in order to reduce the likelihood of similar occurrences, the following guidelines should be followed:
- employers should designate an on-site worker who is responsible for warning pedestrian workers in the event of an emergency involving nearby mobile equipment;
- employers should ensure that equipment is always maintained in the proper working condition; and
- employers should design, develop, and implement a comprehensive safety program.
INTRODUCTION
On May 26, 2000, MN FACE investigators were notified of a work-related road construction fatality that occurred on May 16, 2000. The county sheriff’s department was contacted and releasable information obtained. Information obtained included a copy of their report of the incident, and copies of statements taken from other workers who were at the site at the time of the incident. A site investigation and employer interview was conducted by a MN FACE investigator on December 18, 2000. During MN FACE investigations, incident information is obtained from a variety of sources such as law enforcement agencies, county coroners and medical examiners, employers, coworkers and family members.
The employer in this incident was an asphalt paving company that had been in business since 1985. The number of company employees varied from approximately 100 during the spring, summer and fall to as few as 12-15 during the winter months. The company had a comprehensive written safety program and conducted employee safety meetings at the beginning of each new job.
The company provided machine specific “on-the-job” training for all machine operators. This training was provided to inexperienced employees by more experienced senior employees. The victim had worked for the employer for seven years and was one of their most experienced employees. He had operated the rock spreader in the past and because of his knowledge and experience he was assigned to operate it during the paved road resurfacing project that was begun on the day of the incident.
INVESTIGATION
On the day of the incident the victim was working as a member of a crew of about 25 workers at a paved road resurfacing site. The victim’s employer was a bituminous seal coat contractor and had been contracted by the county to apply a surface seal coat to 16 miles of an existing paved county road. The seal coating project was being done as part of the county’s annual road maintenance program. The project was also the employer’s first seasonal road maintenance project for the year 2000. Due to below freezing temperatures during winter in Minnesota, road maintenance projects are conducted from the beginning of spring through the end of fall each year. The seal coat being applied to the paved road consisted of a layer of liquid asphalt sprayed on the surface of the road. A thin uniform layer of crushed rock was then spread across the liquid asphalt. Before the liquid asphalt cooled and dried, heavy compaction rollers were used to compact and bond the crushed rock and liquid asphalt to the existing paved surface.
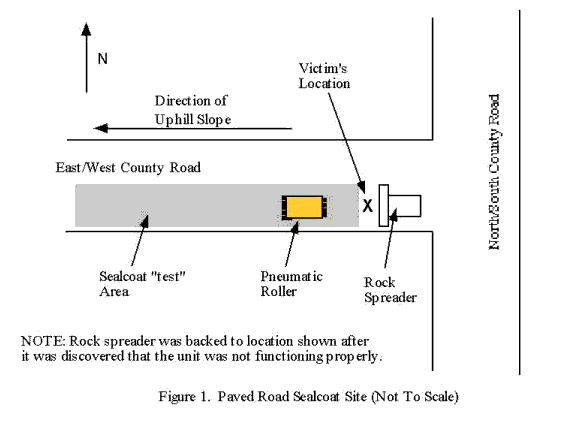
The incident occurred on the first day that a crew of workers arrived to begin the 16 mile resurfacing project. The incident site (Figure 1) was within 150 feet of a T-intersection created by an east/west paved county road and a north/south paved county road. The east/west road was being resurfaced beginning at the point of it’s junction with the north/south road and continuing west/south-west for 16 miles. The east/west road had a slight up-hill slope of approximately 10-12 degrees beginning at it’s junction with the north/south road and continuing for approximately one-quarter mile.
Equipment in the vicinity of the incident site included a chip “rock” spreader, three pneumatic rollers, two liquid asphalt tankers and several gravel trucks filled with crushed rock. The spreader, rollers, and tankers had not been used since the previous season but had been serviced in the contractor’s maintenance facility prior to being brought to the incident site. General service performed on the equipment included replacing engine oil and oil filters in each unit, checking fluid levels such as engine coolant and hydraulic oil, lubrication of grease fittings and a visual inspection of hoses, belts, etc. for signs of wear and need for replacement.
The spreader was a self-propelled BearCat unit that had been purchased new by the employer in 1998. It had an operator’s seat and control platform that was occupied by one worker when the machine was in use spreading crushed rock. However, the spreader also had an on-board computer rate control (CRC) unit that monitored and controlled the rate of application of crushed rock as the spreader moved forward. Since the spreader had to be in operation at a seal coating site spreading rock for the CRC unit to be functioning, the control unit could not be checked for proper operation at the contractor’s aintenance facility. The spreader had a hopper at it’s front end that allowed a dump truck to unload directly into the spreader as the spreader traveled across the road.
The roller involved in this incident was a nine-wheel pneumatic roller that weighed about 18,000 to 22,000 pounds. It was purchased new by the employer in 1994 and had been used approximately 2000 hours. The roller was equipped with hydraulic activated brakes on each wheel that were controlled by the operator via a foot pedal. The unit was also equipped with a hand operated emergency brake. The roller’s drive system consisted of a four speed manual transmission coupled with a variable speed hydrostatic drive. Movement of the roller required the operator to manually place the transmission in one of four gears while the roller was stationary. The forward or backward movement of the roller was controlled by the forward or backward movement of a lever that controlled the hydrostatic drive. Forward movement of the lever caused the roller to move forward. Backward movement of the roller was obtained by moving the control lever through its neutral position and the continued movement of the lever in the opposite direction from that required to drive the roller forward. The hydrostatic drive system enabled the operator to change the direction of travel of the roller without shifting the manual transmission between gears.
After the workers arrived at the site, they applied a layer of seal coat to a “test area” of the east/west county road. The test area was applied to the east bound lane of the road and was several hundred feet long. One of the liquid asphalt tankers was used to apply a layer of liquid asphalt to the test area. The chip “rock” spreader was positioned, with it’s front end facing west, at the east end of the test area. A dump truck filled with chipped rock was backed up to the hopper of the spreader. The spreader operator drove the spreader forward pushing the gravel truck as it traveled across the test area and spread a thin layer of rock across the test area.
After crossing the test area, the workers realized that the layer of crushed rock was not as uniform as required in the specifications for the seal coat being applied. The operator of the spreader disengaged the spreading unit, raised the hopper and backed the spreader to the east end of the test area to the location shown in Figure 1. The uneven layer of rock was caused by a problem with the spreader’s computer rate control (CRC) unit. After the operator parked the spreader, he slowed it’s engine to an idle, dismounted and walked to the front of the unit to a CRC unit control panel. While he attempted to determine what the problem was with the CRC unit, an operator of one of the pneumatic rollers was directed to pack the rocks that had been spread over the test area.
The operator drove his roller onto the test area with the unit facing west. He drove the unit forward to the west end of the test area and then backed it to the east end of the test area. Due to the incline of the road the roller was driven up a slight incline as it traveled west and down the incline as it was backed to the east end of the test area. Near the east end of the test area, the roller’s manual transmission slipped out of gear and the roller began to roll toward the spreader. The operator could no longer control the roller via the hydrostatic drive since the manual transmission was no longer in gear. He stepped on the hydraulic brake foot pedal but was unable to stop the roller. He attempted to pull the emergency brake while also yelling to workers at the site to clear the area. Other workers ran from the area however the victim who was facing the CRC unit on the spreader apparently did not hear the call to clear the area due to the noise of the spreader’s engine. The victim was crushed when the pneumatic roller struck the front of the spreader.
The roller operator immediately shifted it into gear and drove forward. The victim fell to the ground and other workers immediately called emergency personnel who arrived at the scene shortly after being notified. They transported the victim to a local hospital where he died shortly after he arrived.
CAUSE OF DEATH
The cause of death listed on the death certificate was multiple blunt force chest, abdominal and pelvic injuries due to highway construction accident.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should designate an on-site worker who is responsible for warning pedestrian workers in the event of an emergency involving nearby mobile equipment.
Discussion: Construction work zone crews are exposed to an increased risk of injury whenever any type of motorized vehicle is moving in close proximity to pedestrian workers. The risk of injury to a pedestrian worker is greater if the pedestrian worker is focused on a task that is not directly related to construction tasks being done at the work site. In this incident, the victim was troubleshooting a computer control problem on a parked rock spreader. While the victim attempted to determine the cause of the spreader problem, his attention was focused on the computer control unit and probably not on other hazards at the work site. This may have contributed directly to the victim not hearing the verbal warning to clear the area as the roller approached the victim and the rock spreader. Whenever a pedestrian worker or workers are required to focus their attention on any tasks at a work site such as the troubleshooting, service or repair of a machine, another worker should be designated to act as a spotter to warn of any hazards that the pedestrian worker may not be aware. The designation of a spotter in this instance for the duration of time while the victim was attempting to determine the cause of the spreader problem may have prevented this incident from occurring.
Recommendation #2: Employers should ensure that equipment is always maintained in the proper working condition.
Discussion: Employers should ensure that equipment is regularly inspected and maintained in proper working condition. Upon inspection, if equipment is found to need maintenance or repair, the equipment should be taken out of use until it is repaired. In this incident, the operator of the pneumatic roller was not able to stop the roller by stepping on the hydraulic brake pedal or by attempting to use the roller’s emergency brake. After the incident the roller was returned to the employer’s maintenance facility for approximately four weeks during which it’s brake system was examined to determine if a brake failure had prevented the operator from stopping the roller. The brakes were found to be in working order and the roller was returned to service without any repair work being done on the roller’s brakes. Although the brakes were found to be in working order, it is critical the all machines and equipment are properly maintained to insure the safest possible work environment for all employees.
Recommendation #3: Employers should design, develop, and implement a comprehensive safety program.
Discussion: Employers should ensure that all employees are trained to recognize and avoid hazardous work conditions. A comprehensive safety program should address all aspects of safety relate to specific tasks that employees are required to perform. OSHA Standard 1926.21(b)(2) requires employers to “instruct each employee in the recognition and avoidance of unsafe conditions and the regulations applicable to his/her work environment to control or eliminate any hazards or other exposure to illness or injury.” Safety rules, regulations, and procedures should include the recognition and elimination of hazards associated with tasks performed by employees.
REFERENCES
- Office of the Federal Register: Code of Federal Regulations, Labor, 29 CFR Part 1926.21(b)(2), U.S. Department of Labor, Occupational Safety and Health Administration, Washington, D.C., July 1, 1994.
To contact Minnesota State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.