
Iron Worker Dies When Struck By Falling Steel Header Beam
Michigan Case Report: 07MI106
Summary
On August 20, 2007, a 49-year-old male ironworker was struck by a falling steel ceiling header beam while he was removing a vertical 2- x 8-inch lumber support under one of the ends of the header beam. The decedent and a coworker had previously installed two C10 channels to sandwich a hollow cinder block wall separating a new building addition from the existing building. After the hollow wall was partially demolished for access between the addition and the existing building, the decedent installed a continual steel plate at the base of the sandwiched wall to complete the header for the access way. On the day of the incident the decedent and the same coworker arrived at the jobsite to install steel channels on each side of the access way opening from the floor to the header. The crew unexpectedly found screwed, epoxied 2- x 8-inch lumber on the north and south door walls. The coworker pried off the north board without incident. The decedent removed the screws on the south board, twisted the board, and then used a hammer to hit the base of the board, releasing it from the wall. As the decedent turned, the header beam came down, striking him in the head and landing on his legs. His coworker ran to another person on site and asked him to call 911. The coworker returned to the decedent and attempted to move the beam with a pole. Unable to move the beam, the coworker applied pressure to the decedent’s head to control the bleeding. After calling 911, the other person on site retrieved a jack from his vehicle to raise the beam. This jack could not raise the beam, and a second jack was retrieved. Using two jacks, the beam was raised from the decedent (Figure 1). He was taken by emergency response to a local hospital where he died four days later.

|
|
Figure 1. Header beam that fell onto decedent and two jacks used to raise beam from decedent. |
Recommendations:
- Professional expertise should be obtained in writing prior to contractors making structural support changes necessitated by jobsite conditions.
- Jobsite protocol should include employees reporting unexpected or new work site conditions to the home office or to the general (controlling) contractor to ensure enough information is gathered to proceed with an alternate work plan.
- General (controlling) contractors should report alterations and changes in work site conditions to appropriate subcontractors who could affect the safety of subcontractor personnel.
- General contractors should ensure that all required documentation is available on site.
- Temporary shoring (support) systems should be approved by a qualified professional engineer and identified by the contractor who installed it.
- Steel erectors should insist that the controlling contractor provide them with the required written notifications regardless of job size.
Introduction
On August 20, 2007, a 49-year-old male ironworker was struck by a falling steel ceiling header beam while he was removing a vertical 2- x 8-inch lumber support under one end of the header beam. On August 27, 2007, MIFACE investigators were informed by the Michigan Occupational Safety and Health Administration (MIOSHA) personnel, who had received a report on their 24-hour-a-day hotline that this work-related injury had occurred on August 20, 2007, and that the individual had died on August 24, 2007. On November 16, 2007, MIFACE interviewed the company owner at the company headquarters. During the course of writing this report, the police report and pictures, death certificate, medical examiner report, and the MIOSHA file and citations were reviewed. All pictures used in this report are courtesy of the MIOSHA file.
The company for whom the decedent worked conducted steel erection. The firm had been in business for 25 years. The company seasonally employed approximately 50 people; during most of the work year, 25 people were employed. The decedent was a journeyman ironworker, who worked as a full-time hourly employee. Six individuals had the same job title as the decedent; journeyman/foreman. He had worked at the company for approximately 15 years. He had 29 years of experience as an ironworker. He was a member of a union. His eight-hour workday began at 7:00 a.m.
The company had a written safety and health program. The company safety program was originally developed in conjunction with a consultant. It had been recently updated. The company owner was responsible for the safety program administration. There were no procedures in place for the task being performed by the decedent. The firm did not have a health and safety committee. The company’s safety program designated the foreman on each job site to be responsible to implement safety program requirements. The company field superintendent oversees the foreman. The firm routinely held weekly tailgate safety meetings with the employees. The company owner picked the subject and the foreman was responsible for conducting the tailgate talk. More frequent safety meetings were held if a work contract required them. The company, as well as the union hall, provided safety training for the employees.
At the conclusion of its investigation, MIOSHA Construction Safety and Health Division issued the following Serious citations to the employer:
SERIOUS:
- DEMOLITION, PART 20, RULE 2031(1)(a)(i)(ii)(iii)(iv)(b)(c)(d). No demolition survey was found at the site.
SERIOUS:
- STEEL ERECTION, PART 26, RULE 2614(1). Structural stability was not maintained during erection of steel posts on a construction site..
NOTE: MIOSHA Construction Safety and Health Division cited Company A for not following the engineering drawings.
Investigation
Companies Involved In the Work Project.
The decedent’s employer was a subcontractor for Company A, who was hired by the general contractor. The general contractor is defined within the MIOSHA Construction Safety Standard, Part 26 – Steel Erection, as the “controlling contractor.” The general contractor bid for and received the contract to construct an addition to a substation owned by Company B. Company A was contracted to provide a steel header beam assembly and install decking for the roof system for the addition. Company B also contracted for security guards on site. The new addition was to be attached to the existing structure, composed of hollow cement block walls. When the new addition was enclosed, the hollow block wall separating the new addition and existing structure was scheduled to be demolished to provide access between the new addition and the existing structure.
The decedent’s employer was contracted by Company A to unload and install the roof deck for the substation’s addition and sandwich the existing 26-foot hollow cement block wall separating the existing building and new addition with C10 steel channels. This contract included the initial installation of two C10 channels on both sides of the block wall to “sandwich” the wall. After another contractor completed the partial demolition of the wall for an access way, the decedent’s employer was contracted to install a steel plate across the base of the exposed access header.
The decedent’s employer had been subcontracted numerous times by Company A and had worked with representatives from Company A. Over the years, the course of their business relationship evolved, and the decedent’s employer would act as Company A’s “agent” on a work site.
Company B had previously hired an engineering firm to develop the building plans for the new addition. The decedent’s employer indicated that his firm, and Company A and Company B had reviewed the building plan blueprints.
July 20, 2007 jobsite meeting of the decedent and controlling contractor.
The decedent and the controlling contractor discussed the installation of the deck support angles, roof deck, and the C10 steel channels. The C10 channel could not be installed as specified by the engineering drawings because of the location of a cable tray and its associated wiring. The C10 channels were designated by drawing to be placed directly against the roof material. They could not be placed in this position because of the cable tray/wiring (Figure 2).
 |
|
Figure 2. Location of cable tray interfering with original placement of C10 channels. Also shown is location of beam breakaway from the block wall.
|
The decedent and the controlling contractor discussed options to install the C10 channels to accommodate the position of the cable tray/wiring. The discussion yielded the following installation revisions: the channels would be lowered to the fourth course of concrete block and the end holes for the C10 channel bolts would be moved 12 inches toward the middle of the wall on the north end and 18 inches toward the middle of the wall on the south end (Figure 3). The engineering firm was not consulted in this process, nor was written approval for changes from the original drawings obtained. The controlling contractor gave the decedent permission to change the position of the channel and end bolt locations. The decedent’s employer indicated during the MIFACE site visit that at the time of the discussion, the decedent and the controlling contractor did not know the dimensions of the future wall opening. The MIOSHA file indicated that there was no written demolition plan on site.
The decedent and his crew installed the angle iron for the metal decking to rest upon. The crew then installed 20 feet of channel iron on each side of the fourth course of existing block of the wall to create the header. Installation of the channel was per their usual procedure: drilling one side, then coming back through the other side so the drilled hole met in the middle of the block. The decedent and his coworker installed five bolts, one bolt at the north end, one bolt at the south end, and three bolts in the middle.
July 23, 2008
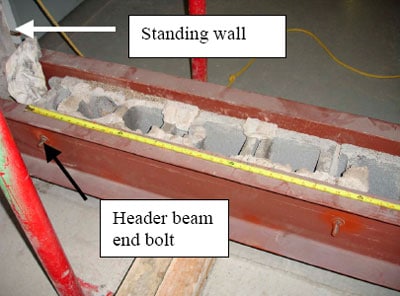
The company subcontracted to cut the opening in the wall completed its work. After the wall opening was cut, sixteen inches were left on each side, leaving the header beam suspended without support. The demolition company took out the wall past the C10 channel end bolts. It is unknown if the controlling contractor was present at the time of the demolition (Figure 3).
 |
|
Figure 3. Location of header beam’s end bolt showing end bolt not placed in standing wall.
|
July 24, 2008
The decedent’s employer was advised that the hollow wall was removed and they could now install a continual steel plate from the north edge of the wall to the south edge wall to complete the access way header.
July 27, 2008
The decedent and two coworkers installed 2-inch wide metal straps at the block mortar seams and then installed a 3/8-inch thick solid steel plate across the exposed block that had been cut away forming the base of the header beam “sandwich.” At the time of the addition of the steel plate, there were no boards supporting the header at each end of the wall opening. One of the decedent’s coworkers indicated that “somewhere about the middle of the process they wondered why the header didn’t go into the wall like a bearing pocket.”
July 27 to August 10, 2007
The substation was located near a train track where coal was being transported. The decedent’s employer indicated that building vibration was produced as the loaded coal cars were moved. Sometime after July 27, and before August 10, a Company B security guard and another worker from another company (Company C) brought a concern about the stability and safety of the header beam to the attention of the controlling contractor’s superintendent. To stabilize the header, the controlling contractor’s superintendent applied epoxy and screwed the 2- x 8-inch lumber supports to each side of the cut block from the footing to the header. Both lumbar supports were not marked in any way to indicate their use as support structures for the header beam assembly.
After installation, the controlling contractor’s superintendent contacted Company A to fabricate and install two steel channel posts to cover the lumber supports. MIOSHA could not obtain a written confirmation of this order. Company A generated a separate work order for the decedent’s employer to install the Company A fabricated steel channels on the wood-covered block wall jambs. MIOSHA was unable to locate a pre-existing written contract between the decedent’s employer and Company A for installing the channels at the wall opening edges.
In the MIOSHA file, the controlling contractor’s superintendent indicated that he informed Company A that the two steel channel posts were for both support and cosmetic purposes. The decedent’s employer stated to the MIFACE researcher that Company A did not inform him that the lumber had been positioned for support purposes and that the steel channel posts should be installed over the wood supports. He indicated to the MIFACE researcher that he thought the channel posts were to be installed for cosmetic reasons only and that the posts were to be directly over the cut block, not over wood.
Day of Incident – August 20, 2007
The decedent and his crewmember, an apprentice, received their job assignments. When they had arrived at the first job of the day, it was raining, so they were directed to the incident site to install the doorjambs. The two workers drove their own vehicles to the work site.
The decedent and his coworker arrived at job site and signed in with Company B’s security guard, who was the same guard that brought the header stability issue to the controlling contractor’s attention. The channel posts to be installed were present at the site. Upon arriving at the incident site, the crew donned arc clothing and hard hats (the required protective clothing). They noted the wood boards on each side of the opening. A representative from Company C was on site when the crew arrived. According to the decedent’s employer, the decedent decided that boards should be removed to minimize the possibility of a fire during the installation/welding of the channel posts.
The decedent returned to his vehicle and obtained a screwdriver to remove screws from the lumber. The decedent and his apprentice removed the screws from the north board. After striking it with a hammer, the board split lengthwise and the wood was pried from the block. The security guard did not inform the decedent or his coworker about the reason for the board placement.
The decedent began to remove the south board. He unscrewed the screws and started to twist the board. His coworker assisted him. They struck the board in the middle and it seemed sound. They then struck the board three times at the bottom, which caused the board to come loose.
The decedent turned to his left. The entire channel iron header assembly, including channels, bolts and the sandwiched block broke away and struck him on his hard hat, and then his shoulders. It came to rest on his legs. The 21- foot long beam weighed between 3,800 and 4,200 pounds. The south end of the assembly was the first to come loose.
His coworker, who witnessed the event ran to the security guard on site and asked him to call 911. His coworker returned to the decedent and tried moving the header assembly with a pole as the security guard called for emergency assistance. Because the decedent’s head was bleeding, his coworker ceased his efforts to move the header assembly and applied pressure to his head.
Due to the weight of the beam, a jack was required to lift the beam from the decedent. The security guard brought one jack, but the jack was unable to lift the beam. A second jack was obtained by the security guard, and was placed under the beam. Both jacks were able to lift the beam assembly, and the decedent was removed from under the assembly (Figure 4).
EMS arrived and transported the decedent to a local hospital. He died four days later from his injuries.
 |
|
Figure 4. Header beam on floor. Position of jacks to raise beam
|
Back to Top
Cause of Death
The cause of death as listed on the death certificate was blunt force head trauma and complications. Toxicology analyses performed at the time of death showed medications consistent with hospital treatment.
Back to Top
Recommendations/Discussion
Professional expertise should be obtained in writing prior to contractors making structural support changes necessitated by jobsite conditions.
The controlling contractor and the decedent did not contact nor consult with the professional engineer who engineered the structural support system prior to installing the C10 channels in a new position on the wall separating the existing building and new addition. The engineer had not designed any wall pockets to receive the C10 channels. Without the demolition survey, the size of the wall opening was unknown. The changes made to the header beam location and anchorage was not compatible with the demolition plan.
The controlling contractor should have alerted the engineering firm who designed the header support that the design plans as delivered to the site did not appropriately reflect the work site layout. The decedent’s employer indicated that although his firm had been involved in steel erection for many years, the controlling contractor was “fairly new” to the role of project coordination. Although any redesign or time spent in consultation may have delayed the progression of the work, it may have prevented this fatality.
Jobsite protocol should include employees reporting unexpected or new work site conditions to the home office or to the general (controlling) contractor to ensure enough information is gathered to proceed with an alternate work plan.
The decedent was not expecting to see wood affixed to the edge of the masonry wall. According to the decedent’s employer, commonly used dimensions of wood used for support are 4- x 4- inch or 6- x 6-inch, not 2- x 8-inch. The unmarked, unusually sized, but very securely affixed lumber did not “raise a warning flag” for the decedent. The decedent’s employer speculated that the decedent might have assumed that the wood was affixed for cosmetic purposes only and thus could be removed without incident. The decedent, according to the employer, may have determined that there was a risk of fire while welding the steel channel, so his course of action was to remove both wood supports prior to the welding process. Removing both of them, without further additional support of the beam, proved deadly.
When jobsite conditions have changed or unexpected conditions arise, the foreman is usually deemed the competent or qualified person and would be responsible for identifying and correcting the situation. MIFACE recognizes that supervisory personnel in the field must make judgment calls using their work experience and expertise. There are times, however, that situations arise when a judgment to correct the condition requires more information. MIFACE encourages employers to encourage their employees to call the office or to gather more information from other individuals on site when addressing a potential structural support issue, such as the removal of unmarked, attached boards to cut block positioned under support beams without prior authorization.
General (controlling) contractors should report alterations and changes in work site conditions to appropriate subcontractors who could affect the safety of subcontractor personnel.
An unexpected work site condition emerged in the construction process – to make the doorway, more of the wall separating the existing building and the new addition was removed. After the installation of the metal plate to complete the header assembly, other individuals on site were concerned with the header stability. Without written job orders, it is difficult to determine “who was told what” in this tragic incident. A lack of communication was a factor in this incident.
The change in jobsite conditions was not adequately documented nor communicated to affected subcontractors by the controlling contractor or by Company A). A written job order from the controlling contractor to Company A and then from Company A to the decedent’s employer could have provided the equivalent of a chain of custody, indicating the construction to be performed and alerted the downstream subcontractors that the header was perceived to be unstable. A different job procedure may have been implemented, such as supplying additional support jacks to the header while the wood supports were being removed prior to installation of the steel channels.
General contractors should ensure that all required documentation is available on site.
The decedent’s employer stated to the MIFACE investigator that neither the decedent nor the controlling contractor knew the extent of the wall demolition. The owner stated that when walls are demolished for access between rooms, the demolition usually occurs in thirds – 1/3, 1/3, 1/3 across the wall. In this incident, the usual was not the case. The demolition firm removed approximately 90% of wall leaving only 16″ of cinderblock on each side of throughway. The header beam would not have come down if the last end bolts were installed in the non-demolished section of the wall.
During the discussion with the controlling contractor, the decedent most likely assumed that the wall would be demolished in accordance with his past experience. This may have led him to a false sense of security when weighing options with the controlling contractor representative, the new placement of the end bolts.
General contractors should ensure that all necessary construction paperwork has been completed and is available on the jobsite for consultation during the construction project.
Temporary shoring (support) systems should be approved by a qualified professional engineer and identified by the contractor who installed it.
Although a steel column was not being erected at the time of the incident, Part 26 offers good guidance to controlling contractors when jobsite conditions indicate that erection stability issues are unexpectedly encountered. R 408.42626(4) states all columns shall be evaluated by a competent person to determine whether guying or bracing is needed; if guying or bracing is needed, then it shall be installed. The controlling contractor did not have a competent person evaluate the 2- x 8-inch wood support to determine if it was appropriate bracing material
The controlling contractor did not mark the wood with “Do Not Remove” to highlight it as a structural support, and did not apply yellow caution tape to indicate that the wood was being utilized as a structural support. Because the wood was not marked to indicate its use as a support, an erroneous assumption was made by the decedent. MIFACE recommends that contractors who install supports identify the supports as to their function.
Steel erectors should insist that the controlling contractor provide them with the required written notifications regardless of job size.
Steel erection activities as defined by MIOSHA Construction Safety Standard, Part 26, Steel Erection include: (a) Hoisting, laying out, placing, connecting, welding, burning, guying, bracing, bolting, plumbing, and rigging structural steel, steel joists and metal buildings; (b) Installing metal decking, curtain walls, window walls, siding systems, miscellaneous metals, ornamental iron, and similar materials; and (c) Moving point-to-point while performing these activities.
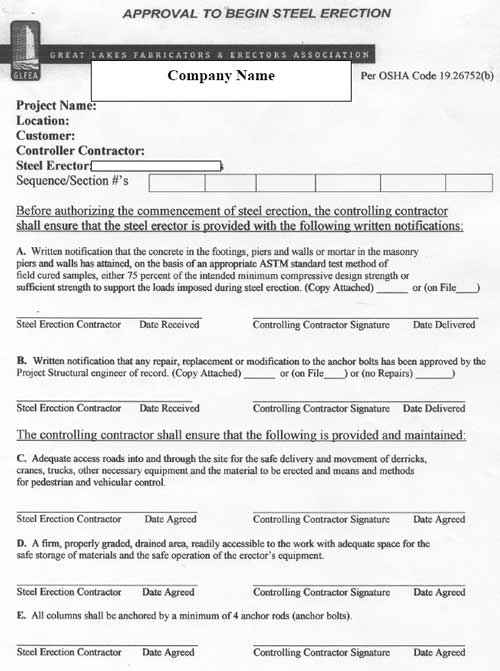
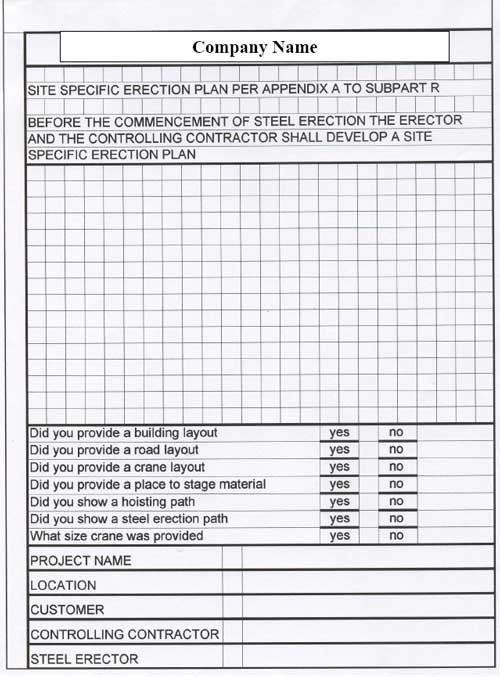
Even small steel erection jobs need the required written notifications. After the incident, the decedent’s employer, with the assistance of an outside health and safety contractor, developed a form to ensure that the controlling contractor has met all of their required written notifications to the firm. The form is attached as Appendix A. MIFACE encourages all steel erection firms to insist that the controlling contractors meet the written notification and site layout requirements of the MIOSHA Steel Erection standard. The notifications and site layout requirements protect not only employees working at the site, but also ensure that the building and surrounding land is capable of supporting the building process. Appendix A contains a copy of the company’s new Approval to Begin Steel Erection form.
References
MIOSHA standardsexternal icon cited in this report may be found at and downloaded from the MIOSHA, Michigan Department of Labor and Economic Growth (DLEG) website at: www.michigan.gov/mioshastandards. MIOSHA standards are available for a fee by writing to: Michigan Department of Labor and Economic Growth, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan 48909-8143 or calling (517) 322-1845.
- MIOSHA Construction Safety Standard, Part 26, Steel Erection.
- MIOSHA Construction Safety Standard, Part 20, Demolition.
- Industrial Accident Prevention Association (IAPA). Free downloads of health and safety informationexternal icon. http://www.iapa.ca/Main/resources/resources_downloads.aspx (Link updated 4/1/2009)
Appendix
Company’s Approval to Begin Steel Erection Form
 |
 |
Michigan FACE Program
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicineexternal icon, 117 West Fee Hall, East Lansing, Michigan 48824-1315; http://www.oem.msu.edu/MiFACE_Program.aspx. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 7/21/08 (Link updated 8/5/2009)
MIFACE Investigation Report # 07MI106 Evaluationpdf iconexternal icon (see page 14 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.