
Machine Operator Dies After Being Struck by a Shredder Grate During Shredding Machine Maintenance
Michigan Case Report: 06MI009
Summary
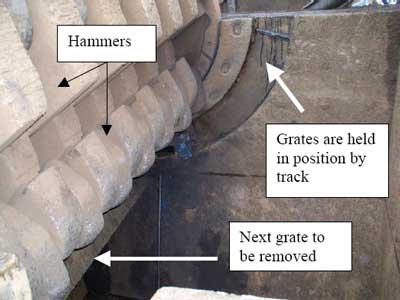
On February 16, 2006, a 42-year-old male machine operator was critically injured after being struck by a 2,500-pound iron grate that he was removing from a metal shredding machine (also known as a hammer mill). There were 13 grates that required removal. Each grate lay in a track, which held them in position in the shredder box. Five grates had been removed. To remove a grate, the decedent attached a separate steel alloy chain to each end of the grate and a mobile crane lifted the grate out of the machine via the grate track (Figure 1). The incident occurred during the removal of the sixth grate. The grate was located at a five o’clock position. The decedent had attached the chains to the grate and the hoisting process began. The grate became stuck in the grate track. To facilitate its removal, the decedent used a torch to partially cut through the grate while it was still under tension from the crane. The crane again attempted to lift the grate from the machine. Because the grate again did not move, the decedent cut through the grate end while the grate was still under tension. When the grate was cut through, the momentum of coming to center caused the grate to continue past center and strike the decedent in the side of his head. 911 was called and the decedent was transported to a local hospital where he died three days after the incident.
|
|
Figure 1. Grate and grate track in shredder box
|
Recommendations:
- Employers should conduct a job safety analysis (JSA) when performing non-routine tasks or using non-routine tools, develop a standard operating procedure for the identified tasks, and train applicable employees on the procedure.
- Employers should provide rigging training to employees involved in lifting a heavy load with load-bearing equipment.
- Employers should form a joint Health and Safety committee.
Although not a factor in this incident, MIFACE recommends:
- Employers evaluate the workplace to identify any confined spaces and develop and enforce written work procedures for entry into these areas.
- Employers establish written lockout/tagout procedures to provide employee protection from injury due to unexpected/unintended motion, energization, start-up or release of stored energy from the machine, equipment or process when working in, on, or around the equipment during repair, maintenance or other associated activity.
Introduction
On February 16, 2006, a 42-year-old male machine operator was critically injured after being struck by a 2,500-pound iron grate that he was removing from a metal shredding machine. On February 21, 2006, MIFACE investigators were informed by the Michigan Occupational Safety and Health Administration (MIOSHA) personnel who had received a report on their 24-hour-a-day hotline that a work-related injury had occurred on February 16, 2006, and that the individual died on February 19, 2006. On January 17, 2007, the MIFACE researcher interviewed the firm’s Safety and Environmental Manager. During the course of writing this report, the police report, medical examiner’s report, and MIOSHA file and citations were reviewed. Figures 3 and 4 are courtesy of the MIOSHA compliance officer. The decedent’s employer granted MIFACE permission to view and take pictures (Figure 2) of the incident site. The employer also shared pictures of the incident site (Figures 1 and 5) and the company’s Shredder Grate Change Instruction developed after the incident. The Instruction is located in Appendix A. MIFACE has removed company identifiers from the Instruction and from Figure 4.
The decedent’s employer had been in business over 100 years. They had conducted scrap recycling operations at the incident site for at least 20 years. The firm processed paper, plastic, ferrous and nonferrous metals at multiple locations in Michigan. The decedent was a full time, hourly machine operator. He had previously worked for the company for five years as a supervisor. He left the company for a period of time and was rehired as a machine operator about two and one-half years before the incident. He had nine years experience running the metal shredding machine. NOTE: MIOSHA references the metal shredding machine as a hammer mill. For the purposes of consistency with the company grate change instruction sheet, MIFACE will refer to the metal shredding machine (hammer mill) as a shredder.
The work shift began at 7:00 a.m. and ended at 5:00 p.m. The firm had a written health and safety program but did not have a specific procedure for removing and replacing the shredder grates. The company safety program, although written, was sporadically implemented and enforced. The person responsible for safety (safety and environmental manager) was not headquartered at the incident location. This person reported to human resources and had on-the-job experience. The company had a health and safety committee primarily composed of management personnel, although it did have a few hourly employees as members. The safety committee met monthly. Monthly safety meetings were held with employees at their jobsite and training records were kept. Employees took part as trainers, inspectors and problem solvers. The firm encouraged employees to report hazards. Employees also had input regarding safety and health training.
MIOSHA General Industry Safety and Health Division issued the following alleged Serious citation regarding the fatality to the company at the conclusion of their investigation.
- GENERAL PROVISIONS, PART 1, RULE 11(a).
- The employer did not provide training to each newly assigned employee regarding the operating procedures, hazards and safeguards for rigging of suspended loads on the job.
Back to Top
Investigation
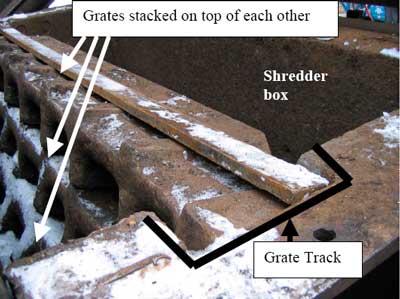
The employer had purchased the land and equipment from another company. The employer received the industrial metal (iron and steel) shredding machine (shredder) as part of the purchase. The shredder involved in the incident shredded metal from cars and sheet iron. The shredder box area was enclosed during shredder operation by a hinged cover. The inside of the shredding box area was approximately 8.75 feet wide x 11.25 feet long and 9.5 feet deep. The shredder was loaded by a conveyor that dumped the metal into the hammering process in the shredder box where it was processed into pieces determined by the size of the grates. There were 13 grates in the shredder, each 112.5 inches long, 17.75 inches in height and 8.5 to 3.0 inches in width and weighing approximately 2,500 pounds. On each side of the shredder box was a track into which the grates were placed and stacked upon each other (Figures 1 and 2). The grates track down around the hammers from approximately a 3:00 position through a 9:00 position. There was a very small space between the edge of the grate and the wall of the track that holds the grates in position. This space was filled with debris (dirt, metal shavings, etc) from the shredding operation. The debris in the track became compacted with time and the grates became “welded in” the track, which could make it difficult to remove them.
 |
|
Figure 2. Grate position in track
|
After being processed into smaller pieces, the metal fell onto an exit conveyor at the bottom of the shredder box that moved the processed material to designated places where a front loader picked it up and placed it into another area.
The shredder had a maintenance manual. The manual included how to maintain the machine and how to install the machine. The manual did not include how to do maintenance repair, such as grate changing instructions. The grate change-out schedule depended upon the types of material that was passed through the machine. Typically, maintenance was performed two to three times per year.
On the day of the incident, it was 30 degrees F with light freezing rain and 18 mph winds from the east.
The decedent was the crew leader of the five-person crew. Changing out the grates was part of his regular job duties and he had received training prior to the job assignment. The yard superintendent and the shredder supervisor were not present.
The crew consisted of the decedent, a mobile crane operator, a coworker on top of the shredder box who assisted in signaling the crane and who helped to hook up the chains to the grates, a temporary worker who unhooked the chains after the grating was set on the ground, and a temporary worker who acted as a “gopher” to perform any other needed tasks.
The chains and lifting configuration (D ring, steel alloy chains) are shown in Figures 3 and 4 . The decedent was assigned to work in the shredder box. He accessed the shredder box via the box discharge conveyor. To remove a grate from the track, the decedent stood on a ladder and hooked a chain around each end of the grate. His coworker standing on a platform at the top of the shredder box would signal the crane operator to lift the grate. After removal from the shredder box, the crane operator placed the grates on the ground nearby.
 |
 |
|
Figure 4. D Ring, chains, mobile crane
|
At approximately 8:30 a.m., the crew began to remove the grates from the shredder box. Five grates had successfully been removed. The crew was having trouble removing the sixth grate because it was “welded in” the grate track. The sixth grate was in the five o’clock position. If a grate did not come out during the initial crane lift, the decedent’s work practice was to partially cut through the end of the grate with a cutting torch while still keeping lifting tension of the grate. The decedent cut part way through the grate and stepped back out of the way to allow the crane operator to attempt to remove the grate. His coworker at the top of the shredder box signaled the crane operator to attempt to remove the grate after the decedent was clear. The grate remained wedged and it could not be removed. The decedent made the decision to make further cuts on the grate. The mobile crane maintained tension on the chains attached to the grate. The decedent stepped back into the swing area of the grate and used a cutting torch to completely cut through the grate. After the grate was completely cut, the grate swung out and struck him in the head and chest area. He was pushed into the back wall of the shredder box.
The coworker standing on the platform at the top of the shredder box witnessed the incident and immediately jumped into the shredder box to help the decedent. He yelled to his coworkers to call 911. The decedent was taken to a local hospital where he died three days later.
After the incident, the company management convened a special group consisting of several departments to develop specific procedures to remove the grates. The resulting procedure addresses grate securement, cutting the grate, and a flow of command if the grate does not come out without cutting. There is now an approval process a crew must follow if the grate needs cutting for release. The company gave MIFACE a copy of the procedure that was developed. MIFACE has made modifications to the procedure. The modifications are shown in italics. The modified procedure is attached in Appendix A.
Back to Top
Cause of Death
The cause of death as listed on the death certificate was blunt craniocerebral trauma. A blood ethanol was drawn on admission to the hospital; results were negative.
Recommendations/Discussion
Employers should conduct a job safety analysis (JSA) when performing non-routine tasks or using non-routine tools, develop a standard operating procedure for the identified tasks, and train applicable employees on the procedure.
After the incident, the company performed a JSA for this job task and is planning to continue to identify job tasks and perform a JSA for each of these tasks. A JSA is a procedure used to review each job, identify potential hazards, and design actions and procedures to eliminate or control the hazards. Establishing proper job procedures is one of the benefits of conducting a job safety analysis. To conduct a JSA, determine the job tasks, what could go wrong, what the consequences could be, how the hazard could arise (are the tools and equipment right for the job and are they in good condition?), what other potential contributing factors could be, and how likely it is that the hazard could occur.
For each new and/or non-routine activity, a determination of whether or not a JSA is needed should be made. Ask “what are the hazards?” If several hazards can be identified, then a JSA should be performed.
Both MIOSHA and Federal OSHA have resources for employers to learn about JSA. MIOSHA Job Safety Analysis Publication SP#32 explains what a job safety analysis is and contains guidelines for conducting your own step-by-step analysis. A sample of a completed job safety analysis and a blank job safety analysis form are included at the back of the publication. SP#32 can be found on the MIOSHA website at: http://www.michigan.gov/documents/cis_wsh_cetsp32_137664_7.docword iconexternal icon. Another job safety analysis resource is available from Federal OSHA and may be found on the OSHA website at: https://www.osha.gov/pls/publications/publication.htmlexternal icon. (Link updated 12/11/2007)
After the JSA has been performed and a standard operating procedure developed, employers should train their employees on the procedure.
Employers should provide rigging training to employees involved in lifting a heavy load with load-bearing equipment.
MIFACE uses the term rigging to signify any type of connective and load-bearing equipment involved in lifting heavy loads. Among the elements of a basic rigging plan and topics a rigging course may cover is risk management, basic rigging principles and load control, job site safety, hand and voice signal communications, proper use of rigging hardware and lifting devices, determining load weights and calculating sling angles, rigging plan procedures, and how to conduct inspections of rigging, hardware and lifting devices.
The decedent did not have rigging training. The employer grate change out procedure does not contain a provision stating that only personnel who have rigging training are permitted to change out the grates. The employer procedure specifically includes inspection of the rigging, hardware and lifting devices. Personnel involved in the grate change out procedure should be trained in proper rigging methods and techniques for rigging loads safely. MIFACE has modified Appendix A to include a reference for rigging training.
Employers should form a joint Health and Safety Committee.
The decedent’s employer had a Health and Safety (H&S) Committee, but the majority of committee members were from management. A joint H&S Committee, comprised of both management and hourly employees provides a forum for management and employees to regularly discuss health and safety issues in the workplace. A joint H&S Committee is an important way for employees to help manage their own health and safety, assist the safety manager in providing a safer, healthier workplace, and heighten employee involvement in the company safety program. Employee input is a critical part of a successful safety program; management would become more aware of potential recurring safety hazards in the field and employees can participate in developing safe work procedures. The formation of the Committee provides a process for open communication on health and safety issues and enhances the ability of employees and management to resolve safety and health concerns reasonably and cooperatively.
Much of the potential value of H&S Committees can be lost without careful development of the purpose, functions and activities of the committee. The committee will function effectively only after the need for the committee is recognized and employees, supervisors and managers welcome its services. At their worst, Health and Safety Committees can be a “negative-minded” group confining their approach primarily to (after-the-fact) placing of blame. However, at their best, they can become an effective tool to help prevent unsafe practices and conditions, reduce the risk of injury and illnesses and to help motivate employees and supervisors to become actively involved the road commission’s health and safety program.
MIOSHA has several resources that can be accessed for development of a health and safety committee.
- Good Safety and Health Programs are Built with Good Safety Committees brochure details the advantages of having an effective safety and health committee. Internet Address:
www.michigan.gov/documents/cis_wsh_cet0140_103132_7.pdf. (Link no longer available 4/21/2009) - MIOSHA Safety and Health toolbox: contains ideas, activities, and materials that focus on the major components of a safety and health system. Module 2 of the toolbox focuses on employee involvement and contains several resources for health and safety committee development. Internet Address:
www.michigan.gov/lara/0,4601,7-154-61256_11407_15317-124535–,00.htmlexternal icon. (Link updated 4/1/2013)
The State of Wisconsin has developed “Guidelines for Developing an Effective Health and Safety Committee” (http://www.doa.state.wi.us/docs_view2.asp?docid=665external icon). Road commissions may wish to download this resource as well as the Canadian Centre for Occupational Health and Safety, Occupational Safety and Health Answers: Health and Safety Committees (http://www.ccohs.ca/oshanswers/hsprograms/hscommittees/external icon ). Both of these valuable resources provide a framework for selection of H&S Committee membership, purpose, function and activities.
Although not a factor in this incident, MIFACE recommends:
Employers evaluate the workplace to identify any confined spaces and develop and enforce written work procedures for entry into these areas.
The design of the shredder box met the definition of a confined space, but not the definition of a permit-required confined space. MIOSHA adopted the provisions of 29 C.F.R. §1910.146 entitled Confined Spaces as Part 90 of the General Industry Safety Standards. 1910.146 defines a confined space as a space that: (1) Is large enough and so configured that an employee can bodily enter and perform assigned work; and (2) Has limited or restricted means for entry or exit; and (3) Is not designed for continuous employee occupancy.
 |
|
Figure 5. View into shredder box from platform outside of box showing access point from outside conveyor
|
To enter the shredder, the employee used a fixed ladder to access an outside platform and then climbed up the side of a belt conveyor that was approximately 41 inches tall from the platform. The employee then walked on the platform through rubber baffles that helped keep the debris from flying out of the shredder and then crawled on another conveyor (a shaker conveyor) to access the shredder box. According to the MIOSHA case file, at the time of the incident, the firm did not have this area identified as a confined space.
The shredder box did not meet the definition of a permit-required confined space. A permit-required confined space is a space that has one or more of the following characteristics: (1) Contains or has a potential to contain a hazardous atmosphere; (2) Contains a material that has the potential for engulfing an entrant; (3) Has an internal configuration such that an entrant could be trapped or asphyxiated by inwardly converging walls or by a floor which slopes downward and tapers to a smaller cross-section; or (4) Contains any other recognized serious safety or health hazard.
Although not required by MIOSHA, a written entry procedure should be developed for non-permit confined spaces. Work performed in a non-permit confined space, such as welding, painting, or cleaning with acids or solvent, may produce hazards that could create a permit-required confined space, such as a hazardous atmosphere. When work is planned within a non-permit confined space, the supervisor and the employee(s) working in the space should discuss the entry procedure, the work to be done, all potential energy sources that may need isolation, any hazards that may arise while working in the space and necessary protective measures to be taken, such as personal protective equipment, special tools, or communication requirements.
Employers establish written lockout/tagout procedures to provide employee protection from injury due to unexpected/unintended motion, energization, start-up or release of stored energy from the machine, equipment or process when working in, on, or around the equipment during repair, maintenance or other associated activity.
Locking out machinery and equipment prior to servicing or maintenance is an essential element of protecting employees from the unexpected energization or motion, start up of the machine or equipment, or release of stored energy. In addition to the provisions of Part 85, The Control of Hazardous Energy Sources, MIOSHA also enforces separate rules for working on or near exposed energized or de-energized parts. These rules, which include provisions for lockout of electrical systems, are contained in MIOSHA General Industry Safety Standard Part 40, Electrical Safety-Related Work Practices.
MIOSHA requires the employer to plan for the control of energy during servicing and/or maintenance of machines and equipment by doing the following:
- Establish an energy control program:
- Develop, document and utilize lockout/tagout procedures;
- Provide employees appropriate training;
- Provide, at no cost to employees, equipment required by the lockout/tagout
procedures. - Continuing competency through training.
Potential hazardous energy sources must be identified, isolated, and locked or tagged out before starting a service and /or maintenance task. Typical tasks requiring lockout/tagout procedures include:
- A task requiring an employee to place any part of their body into an area on a machine’s point of operation or where an associated danger zone exists during a machine’s operating cycle;
- Cleaning, repairing, and maintaining machinery with moving parts;
- Clearing jammed mechanisms;
- Removing or bypassing a guard or other safety device;
- Repairing electrical circuits.
Energy sources include electrical, pneumatic, hydraulic, mechanical, thermal and chemical. There may also be stored energy that may remain once the primary energy source is shut down. Stored energy may result from steam, air pressure, compression of springs, electrical capacitors, or gravity.
Employers can find assistance in developing their lockout/tagout program from MIOSHA. Part 85 may be found on the MIOSHA website as well as a number of MIOSHA CET lockout/tagout publications to guide development of a lockout/tagout program. The CET lockout/tagout resources may be found by accessing the MIOSHA website, then clicking on the “Publications, Forms, and Media” link.
References
MIOSHA standards cited in this report may be found at and downloaded from the MIOSHA, Michigan Department of Labor and Economic Growth (DLEG) website at: www.michigan.gov/mioshastandardsexternal icon. MIOSHA standards are available for a fee by writing to: Michigan Department of Labor and Economic Growth, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan 48909-8143 or calling (517) 322-1845. MIOSHA Consultation Education and Training Division has posted many resources on the MIOSHA website that employers may use to assist in complying with MIOSHA Safety and Health standard requirements. The MIOSHA CET materials may be found at: http://www.michigan.gov/lara/0,4601,7-154-61256_11407_30453—,00.htmlexternal icon. (Link updated 4/1/2013)
- MIOSHA General Industry Safety Standard, General Provisions, Part 1.
- MIOSHA General Industry Safety Standard, Confined Space, Part 90.
- MIOSHA General Industry Safety Standard, Floor and Wall Openings, Stairways, and Skylights, Part 2.
- MIOSHA General Industry Safety Standard, Control of Hazardous Energy Sources, Part 85.
- MIOSHA Consultation Education and Training. Good Safety and Health Programs are Built with Good Safety Committees. Brochure #0140. Internet Address: http://www.michigan.gov/documents/cis_wsh_cet0140_103132_7.pdf (Link no longer available 4/21/2009)
- MIOSHA safety and health toolbox. Internet Address: http://www.michigan.gov/lara/0,4601,7-154-61256_11407_15317-124535–,00.htmlexternal icon (Link updated 4/1/2013)
- State of Wisconsin “Guidelines for Developing an Effective Health and Safety Committee”. Internet Address: http://www.doa.state.wi.us/docs_view2.asp?docid=665
external icon - American Riggers Supply Inc. 1010 Kansas Avenue, Kansas City, KS 66105. Catalogue available on Internet. Internet Address: http://www.thomasnet.com/external icon (Link updated 3/25/2013)
- Canadian Centre for Occupational Health and Safety, Occupational Safety and Health Answers: Health and Safety Committees.
Internet Address: http://www.ccohs.ca/oshanswers/hsprograms/hscommittees/
external icon - MIOSHA CET materials for Permit-Required Confined Spaces.
Internet address: http://www.michigan.gov/lara/0,4601,7-154-61256_11407_30453-94707–,00.htmlexternal icon (Link updated 4/1/2013) - OSHA Confined Space Advisor.
Internet Address: http://www.dol.gov/elaws/confined.htmexternal icon (Link updated 4/91/2015)
Appendix A
Shredder Grate Change Instructions
Date of Development
Approved By:
Purpose: To detail the essential responsibilities for changing grates on a shredder.
Responsibility and Authority: Shredder Supervision, Crane operator, Shredder Employees, Company Supervision and Company Employees.
Instructions:
- Before starting any work, on the machine all lock out/tagout procedures must be followed as written in procedure ABC.
- Before starting grate change, have new grates laid out in the order of replacement.
- Only a designated employee who has received rigging training may visually inspect the chains and attach rigging chains.
- Before changing or pulling grates, inspect lifting chains, D-ring, clevis, and crane; for any wear, cuts, leaks, stretching, etc. Before rigging, the chains should be visually inspected to ensure that: the clips are in place, the hooks are not bent, or the links are not pinched, stretched, or damaged in any way. Any items that are found to be in need of repair should be directed to Maintenance before the job can be performed. Any items that cannot be repaired should be replaced before the job can be performed.
- The chains must be 1/2”, with all safety latches and hooks in good condition. Chains must be certified with serialized tag present.
- When working above the mill deck and exposed to the open mill cavity, fall protection equipment must be used. This equipment will include a body harness, lanyard and anchor point.
- After all lock out and corresponding inspections have been completed; the grates can be pulled out one at a time. CAUTION! CHAIN LENGTHS MUST BE EQUAL AND PULLED EVENLY TO PREVENT THE GRATE FROM BINDING. SLIP HOOKS MUST BE POSITIONED SO THE CHAIN IS NOT PULLING ON THE OPEN END OF THE HOOK. EVERY EFFORT SHOULD BE MADE TO PREVENT THE GRATE FROM BINDING.
- To pull grate, one chain should be wrapped around each end of the grate.
- The crane jib should be centered over the middle of the grate to ensure an even pull.
- After the grate has been chained, all personnel that are located on the shaker table below the mill must move off the shaker to a safe area before the grate is lifted.
- One person on the mill deck or adjacent area must be in visual contact with the crane operator and the grate being pulled. The spotter will instruct the crane operator to begin pulling the grate using proper hand signals or radio communication. All other personnel will move to a safe area.
- All foreign material should be removed from mill sides (grate troughs) prior to pulling the next grate.
- Each grate will be pulled one after the other in the same manner as described above until all grates being changed are removed.
- If any grate will not pull out as described make sure that all dirt and foreign material is cleaned away from grate ends then try again.
- If grate still does not come out, then use a porta-power to evenly jack loose the grate until the crane can resume pulling and removal.
- If the grate still does not come out, contact the company or an experienced Supervisor to determine if cutting the grate is the only option or if other options exist such as cutting the side liners, etc. Cutting the grate should be viewed as an option of last resort.
- If it is determined that cutting the grate is necessary the following safety precautions must be observed:
- A platform will be placed across the mill opening to stand above and behind the grates. When possible, the grate being cut should be chained to the hoist or crane from the feed side of the rotor. This will allow the cut pieces to be lowered in a controlled manner to prevent damage to the shaker. If this is not possible, wood or timbers should be placed on the shaker pan to minimize the impact of the falling grate.
- The employee that is torching should make every attempt to cut the grate from above. Depending on the grate location, the employee may have to cut from the feed side of the rotor in order to stay above the grate. During extreme circumstances it may be necessary to cut the grate from an even height or from below (while standing on the shaker). In this case, the grate must be chained to another grate or (solid immovable object) to prevent the grate from swinging after it is cut free. In addition, the grate should be attached to the hoist or crane to support it vertically.
- THE EMPLOYEE TORCHING SHOULD NEVER BE IN A POSITION WHERE THE GRATE COULD FALL, OR SWING TOWARDS THAT PERSON.
- When possible, the employee will use a 4-foot straight head torch to reach the grate.
- After the grate has been chained, all personnel that are located on the shaker table below the mill must move off the shaker to a safe area before the grate is cut.
- After the grate has been cut, it may be necessary to lift the grate in order to unhook the safety chains. The lifting chains should be attached from the feed side of the rotor. The employee unhooking the safety chains should reach down from the feed side of the rotor to undo the safety chains. The employees need to stay above the cut grate at all times. When free, the grate pieces can be lowered to the shaker. From this point the grate pieces can be safely lifted from the mill by attaching the lifting chains on the discharge side of the rotor.
- After the grate has been chained, all personnel that are located on the shaker table below the mill must move off the shaker to a safe area before the grate pieces are lifted.
- After all grates and lower breaker bar (if needed) have been removed and areas have been cleaned and inspected for cracks or excessive wear, new grates can then be installed.
To install new grates, one chain should be wrapped around each end of the grate. One grate is slid into mill at a time. When grate is in the top channel of the side liners all relevant personnel should move to a safe location and one person in visual contact with crane operator will give appropriate hand signal to release tension on chains to allow grate to slide around into position. DURING THE INSTALLATION NO ONE IS ALLOWED IN THE SHAKER UNDER THE MILL.
Michigan FACE Program
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 6/8/07
MIFACE Investigation Report # 06MI009 Evaluation (see page 15 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.