
Quality Control Operator Dies After Falling Into Cherry Processing Brine Tank
Michigan Case Report: 05MI066
Summary
On July 12, 2005, a 38-year-old female quality control operator fell into a brine tank being filled with cherries and drowned. She was the primary tank room supervisor responsible for supervising the loading station employees, monitoring the incoming levels of cherries into the brine tank, recirculation of excess brine from the tank back to the loading station, and moving cherry/brine supply and brine recirculation hoses when the tank was full. Each cherry holding tank has two access ports each covered with a wood cover. One port contained a 4-inch cherry/brine supply hose and a 2-inch brine recirculation hose. The other port contained another 2-inch recirculation hose. Her fall into the cherry holding tank was unwitnessed. It appears she rotated the cover on the port with the one 2-inch recirculation hose, and using an overhead portable utility light, was kneeling on the deck when she fell into the tank. Employees found her floating in the tank, and after one unsuccessful rescue attempt due to the brine fumes, were able to pull her out of the tank. They took her to fresh air, initiated CPR and called 911. Emergency response arrived and took her by ambulance to a local hospital where she was pronounced dead.

|
|
Figure 1. Brine recirculation hose in cherry tank filled with brine and cherries.
|
Recommendations:
- Employers should develop, implement, and enforce a comprehensive written safety program for all workers, which include training in hazard recognition and the avoidance of unsafe conditions.
- Employers should develop and present to workers an annual refresher safety training program for seasonal job tasks.
- Employers should develop, implement, and enforce a comprehensive written program for work in permit-required confined spaces, such as the processing brine tanks.
- The employer should develop a tank opening cover that will allow sightline into the tank, hose access, prevent workers from falling into the tank opening, and allow for proper sulfur dioxide (SO2) ventilation.
- The employer should develop and implement a personal protective equipment (PPE) program, including a respiratory protection program; train employees about PPE (including respirators) use, and enforce employee use of designated PPE.
- The employer should reevaluate its organizational commitment and leadership in regards to its safety program.
- The employer should establish a joint health and safety committee.
- The employer should consider the feasibility of establishing a mode of escape from inside the cherry holding tank.
MIFACE recommends that the company’s safety and health program include:
- Air monitoring during the brining operations to evaluate employee exposure to SO2 to determine whether mechanical ventilation for the brine house is necessary.
Introduction
On July 12, 2005, a 38-year-old female quality control operator fell into a brine tank being filled with cherries and drowned. On July 13, 2005, the Michigan Occupational Safety and Health Administration personnel who had received a report on their 24-hour-a-day hotline (1-800-858-0397) that a work-related fatal injury had occurred that day notified MIFACE investigators of the fatality. On August 23, 2005, the MIFACE researcher interviewed the president and an employee of the company. MIFACE reviewed the autopsy results, death certificate, police report and pictures, and the MIOSHA file and citations for preparation of this report. Figures 1, 3, 6, and 8 are pictures taken by MIOSHA at the time of their investigation. Figure 2 and Figure 4 are pictures taken by the responding police agency, and Figures 5, 7, and 9 are pictures taken at the time of the MIFACE investigation. Pictures were modified as necessary to remove identifying information.
The company for whom the deceased worked was a fruit processing/handling company. The company also provided cold storage for some fruits. The company had been in business for over 50 years and regularly employed approximately 20 people year-round. Seasonal workers were added as necessary. The deceased was a full-time worker and had been with the company for four years. At the time of the incident, the company was processing tart cherries. There were no written safety rules or procedures for monitoring the loading of brine/cherries into the holding tanks and the brine recirculation. Employee safety and health training was conducted by the employer while the employee was on-the-job. The company did not have a health and safety committee.
Although decedent’s official job title was quality control operator, due to the time of year, she was assigned to manage activities associated with one of the company’s a brine tank storage areas. Her job responsibilities as primary tank room supervisor included monitoring the loading of the cherries at the loading station outside of the brine tank storage area, ensuring that the raw fruit evenly entered the brine tanks located within the building, and the brine was re-circulated from the tanks back to the loading station.
The deceased had been given a half-mask, air-purifying respirator to wear when inside the building and as necessary outside at the loading station. Her clothing consisted of flannel shorts, polo shirt, anklet socks and tennis shoes. The company owner stated that regularly, the deceased and other persons who had the same job title would attach the back strap of the respirator so that the respirator would hang around their neck. Because of the frequency of entering the brine tank storage areas, instead of securing the respirator on their face with the upper strap and performing a field fit test, employees would hold the respirator up to their face over their mouth and nose with one hand when they entered the buildings to do the quick checks on the brine tank loading process.
The cherry brining process involves soaking the cherries in the brine mixture of water, hydrated lime (Ca(OH)2), sulfur dioxide (SO2), calcium carbonate (CaCO3), and calcium chloride (CaCl2). The SO2 acted as a preservative in solution. Approximately 34 inches of water was pumped into the wooden holding tank, and then approximately 10 inches of the other brine ingredients were added. The tank held approximately 5200 gallons of the brine solution. The brine solution had an initial pH of 2.5-3.0. After mixing, the holding tank had approximately 44 inches of liquid. The pH was adjusted, and then the tank was ready to be filled with cherries and brine solution from the loading station. The brine solution temperature on the day of the incident was approximately 68 degrees Fahrenheit.
MIOSHA issued 10 Serious citations and 5 Other citations to the employer at the conclusion of their investigation. The Serious citations were for violations of the following standards:
- Personal Protective Equipment, Part 433 – Four citations.
- Rule 5(1) – employer did not assess the workplace to determine if hazards are present, or are likely to be present that necessitate the use of personal protective equipment.
- Rule 6(1) – employer did not train each employee who is required by these rules to use personal protective equipment on the choice, use, limitations and maintenance of the equipment.
- Rule 8(1) – employer failed to ensure that each affected employee use appropriate eye or face protection when exposed to liquid chemicals and air contaminants at the cherry brining operation.
- Rule 10 – employer failed to ensure that each affected employee used appropriate hand protection when exposed to irritating materials at the cherry brining operation.
- Permit-Required Confined Spaces, Part 490, 1910.146- Three citations.
- 1910.146(c)(1) – employer did not evaluate the workplace to determine if any spaces are permit-required confined spaces (brine tanks).
- 1910.146(c)(2) – employer did not inform exposed employees, by posting danger signs or by any other equally effective means, of the existence and location of and the danger posed by permit spaces such as the brine tanks.
- 1910.146(c)(4) – the employer did not develop and implement a written permit space program in accordance with 29 CFR 1910.146, after deciding that its employees will enter permit spaces (an outside brine tank was entered by employees).
- MIOSHA indicated that “as an alternative, the employer may implement alternate entry procedures in accordance with section (c)(5) or the employer may classify the space as a non-permit required confined space in accordance with section (c)(7). In either case, the basis for controlling or eliminating all the hazards must be documented and the space must be certified as safe for entry.”
- Act 154 PA of 1974 – One citation
- Sec 11(a) – employer failed to furnish to each employee employment and a place of employment which is free from recognized hazards that are causing or are likely to cause death or serious physical harm to the employee in that the employer allowed employees to work in and around 10-foot high cherry vats in the brine tank storage area without providing employees with fall protection, exposing the employees to fall hazards.
- Floor and Wall Openings, Stairways & Skylights, Part 2– One Citation
- Rule 213(5) – employer did not guard open-sided runway with a standard barrier and toeboard when four feet or more above an adjacent level (no mid-rails and standard barriers in several building areas).
- Medical Services and First Aid, Part 472 – One Citation.
- R325.47201(3) – employer did not provide suitable facilities for quick drenching or flushing of the eyes and body within the work area for immediate emergency use, where the eyes or body of any person may be exposed to injurious corrosive materials (i.e., employees are exposed to corrosive chemicals including, but not necessarily limited to, sulfur dioxide and hydrated lime at the brine mixing tank and herbicide/desiccant at the pesticide sales/receiving area).
The five Other citations were for violations of the following standards:
- Hazard Communication Standard, Part 430, 1910.1200 – Two citations:
- 1910.1200(f)(5) – employer did not ensure that each container of hazardous chemicals in the workplace was labeled, tagged or marked with the identify and appropriate hazard warning of the hazardous chemicals contained therein (i.e., including, but not necessarily limited to, the brine mixing tank, the brine holding tanks, the gasoline storage tank, and the brine dump station tank).
- 1910.1200(h)(1) – employees were not provided effective information and training as specified in 29 CFR 1910.1200(h)(1), (2), and (3) on hazardous chemicals in their work area at the time of their initial assignment (i.e., newly hired production workers were not provided information and training on hazardous chemicals in the workplace).
- Respiratory Protection, Part 451, 1910.134 – Two citations:
- 1910.134(c)(2) – employer did not establish and implement those elements of a written respiratory protection program necessary to ensure that any employee using a respirator voluntarily is medically able to use that respirator, and that the respirator is cleaned, stored, and maintained so that its use does not present a health hazard to the user. Also, employees were not provided the information contained in Appendix D to the standard (i.e., the employer provided full face-mask and half-mask negative pressure respirators for voluntary use by employees)
- 1910.134(e)(1) – employer did not provide a medical evaluation to determine each production worker’s and chemist’s ability to use a respirator, before each production worker and chemist was fit tested or required to use the respirator in the workplace.
- Control of Hazardous Energy Sources, Part 85, Rule 1910.147(c)(4)(i) adopted by Rule 8502- One citation
- Rule 1910.147(c)(4)(i) – emergency lockout removal was not covered in the written lockout program. MIOSHA recommended that the company install GFI circuit breakers in the main panel for electrical outlets above the brine tanks.
Back to Top
Investigation
Cherries arrived at the facility in cherry tanks filled with water and were unloaded and carried from the transport trucks via a forklift to a loading station. The cherries, after being transported by forklift to the loading station, were dumped into a dewatering tank. One or more operators skimmed the top of the dewatering tank for harvest debris, and then the cherries were pumped onto an elevator/conveyor. Operator(s) at the elevator/conveyor inspect the cherries and remove cherries from further processing as needed. The elevator moved the cherries to a free-fall into a brine-receiving tank. As the cherries free-fall, a fan further dewaters them. A worker at the brine-receiving tank skimmed the top of the tank and pushed the cherries toward the pump opening. The cherries are then pumped with the brine into a tank in a tank room via a 4-inch hose. See Figure 2 and Figure 3.

|
 |
| Figure 3. Loading station for primary tank room and location of deceased when supervising crew. |
The company had three loading stations in operation. Each loading station processed and supplied cherries to a dedicated tank room. Although the deceased was assigned to the primary tank room, she worked at both the north tank room as well as the primary tank room on the day of the incident.
The deceased was the primary tank room supervisor. Her crew size was five to six members; a forklift operator, tank skimmer(s), elevator operator(s), brine receiving tank operator, and brine pump operator. During early cherry season (when the incident occurred) crews were required to work 10-11 hour days. The deceased had recently driven to and returned from a 4-day trip to Texas, arriving home the night before the day of the incident. She was wearing a short sleeve shirt, shorts socks and tennis shoes. She wore glasses (possibly a relevant detail that may have played a role to her death).
The deceased supervised loading station employees from the deck of sunken tanks outside of the primary tank room. Additionally, her job as primary tank room supervisor entailed monitoring the filling of the primary tank tanks, adding or subtracting hoses as needed, and moving hoses to the next tank when one became full. She ascended a couple of stairs to enter the primary tank room.
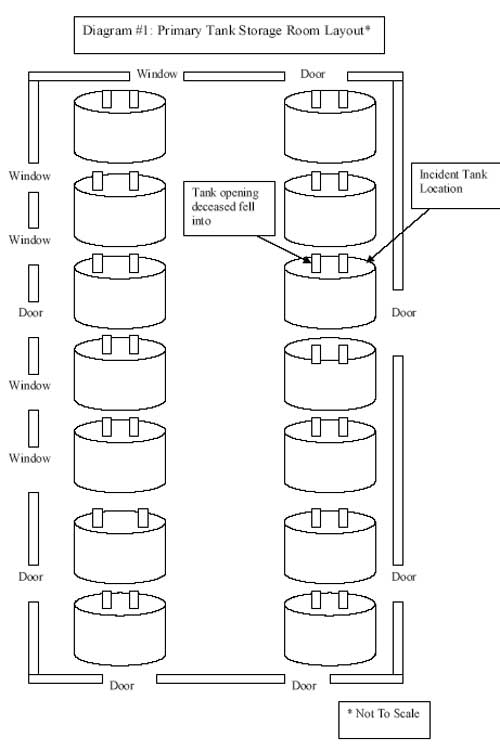
Storage Room. The primary tank room the deceased was responsible for was approximately 37 feet wide by 120 feet long by 18 feet tall (See Diagram 1). The windows and doors were open on the day of the incident. The storage room had 14 brine holding tanks that were approximately 10 feet tall and 15 feet in diameter. The primary tank room was lit by natural light and portable non-commercial utility lights that were suspended by nails from the building trusses. (See Figure 4 )

|
|
Figure 4. Inside of tank storage room-wood decking on and between tanks.
|
Cherry/Brine Tanks. Tank capacity was 65,000 pounds of cherries. The tanks had no internal safety escape mechanism, such as a ladder. Each tank was covered with wood decking that provided walking and equipment access on and between tanks (See Figure 4 ). Each tank had two openings that were approximately 49 1/2 inches by 28 inches. (See Figures 5 & 6) One opening would contain incoming cherries from the loading station and one brine recirculation hose. A second brine recirculation hose was placed in the other tank opening. Each of the openings had a 6-inch wood lip that provided the frame to support a heavy cover. The cover was approximately 55 inches long by 33 inches wide and constructed of a 3/4-inch piece of plywood attached to 2-inch by 4-inch pieces of wood. The openings allowed the operator to observe the contents of the holding tank. (See Figure 5)
Weather. On the day of the incident, the temperature was near 80 degrees and the dew point around 70. Wind speed from 11:00 a.m. to 4:00 p.m. averaged 5 miles per hour (mph). At 4:00 p.m., the wind speed dropped to 0, and at 5:00 p.m. the wind speed gradually picked up to 5 mph. Then at 6:00 p.m., the wind speed dropped to 0 mph again, and stayed at 0 mph until 10:00 p.m.
Storage tank filling process. To fill the brine tank with fruit, workers removed the tank opening cover and placed the 4-inch fruit supply hose into the inlet opening. A dumbbell was used to hold the hose in position. A 2-inch brine recirculation hose was also positioned in the same opening before the cover was replaced. (See Figure 6)

|
 |
| Figure 6. Cherry/brine supply hose held in position by dumbbell. |
A second brine recirculation hose was placed in the remaining tank opening and then that cover was replaced. The brine recirculation pump was on a cart with castors located on nearby wood decking in the storage room. The company procedure stipulated that two people move both fruit-supply and brine recirculating hoses and carts on the decking. The brine recirculating hoses siphoned off the excess brine from the holding tank and prevented a brine overflow condition in the cherry tank. The brine was returned to the loading station brine-receiving tank. Each brine recirculating hose had quick connect couplings and a metal screen to prevent the cherries from returning to the loading station. (See Figure 7)

|
|
Figure 7. Brine recirculation hose with metal screen.
|
One of the deceased’s job duties was to monitor the incoming fruit and the brine level within the tank. The size of the fruit input hose could cause the cherries to pile up on one side of the tank. If the fruit filled unevenly on only one side of the tank, the hose supplying the cherries would need to be moved to ensure that the cherries were evenly distributed within the tank. Additionally, the brine recirculation hoses could get fruit piled upon them, which could create brine recirculation problems. If brine recirculation was not adequate, the recirculation hoses would need to be repositioned. This piled fruit could make that difficult.
To check the cherries’ distribution within the tank and to ensure adequate brine recirculation, the operator would remove the covers, unhook the portable light, kneel down and place the light into the tank opening, then bend over and look into the tank opening.
The tank the deceased was filling had approximately 35,000 pounds of cherries in it when the incident occurred. The brine solution pH was 3.5-3.8. The level of the brine was approximately 25 inches below the top of the tank and approximately 41 inches to the top of the frame for the cover. It appears that the deceased had unhooked the portable utility light that was positioned over the tank opening and suspended by a nail in the building truss (previously positioned). She had rotated the tank cover to one side and balanced it on the 6-inch lip, exposing approximately 80% of the tank opening.
Coworkers initiated a search for the deceased when her day care provider called and asked when the deceased would be picking up her children. Coworkers found her within the tank with her half-mask respirator around her neck. The utility light was found under her, and the tank cover positioned on the 6-inch lip frame. The nail suspending the utility light was found to be bent. Several feet of the unplugged portable utility light’s cord was found in the brine solution. The light cord prongs were bent and found outside of the tank on the decking. It is unknown whether the light was impact coated or if the cord was a “wet” rated cord. According to the medical examiner, she may have been in the brine solution about five minutes. The medical examiner ruled out electrocution as the cause of death due to the absence of electrical current entrance/exit points.
It took two attempts by her coworkers to pull her out of the brine tank. The first attempt was unsuccessful because the coworker who was trying to remove her needed to lift his head out from below the level of the decking to get a breath of fresh air. The coworker tried again and was able to lift her out with the help of another coworker. They laid her on her side on the decking. Her glasses were not on her face. If she was wearing her respirator, it could have been dislodged from her face from the impact of a “head-first entry” into the tank. (See Figure 8)

|
|
Figure 8. Respirator deceased had around her neck when found.
|
The coworkers then took her to fresh air, called 911, and began CPR. Emergency workers arrived, continued CPR, and took her by ambulance to a nearby hospital where she was declared dead.
The event was unwitnessed, and working with company officials, several event scenarios have been developed.
Scenario #1. The deceased wore glasses, and at some time during the monitoring process, the glasses fell off or fogged up. She may have been attempting to reach down into the vat and retrieve her glasses or became disoriented when her glasses became fogged. She may have lost her balance and fell into the tank. The glasses were not found floating on the surface of the tank. The president stated that the tank would need to be emptied to determine if the glasses were in the tank.
Scenario #2. The cherries were piling up upon the brine-recirculation hose. The deceased, because it was so busy, did not want to ask for a second person to help her move the hose. When she was attempting to move the hose by herself, the suction pressure may have caused the hose to move suddenly back into the tank, causing the deceased to enter the tank.
Scenario #3. The deceased was kneeling and checking the level of the brine or cherry distribution within the tank when she was overcome by brine fumes and fell in.
The medical examiner postulated that, both from the dried brine positioning, the lack of contact bruising, and the size of the tank opening, that the decedent most likely could not fall into the tank from a standing or elevated position. There were no patterns suggestive of striking the “lip” of the 6-inch frame on entry or to suggest physical contact with another person. The medical examiner found dirt on her left knee that was consistent with kneeling, and a superficial laceration was present on her left forearm and wrist.
When the responding police arrived, they described an “overpowering” presence of brine fumes, having an irritating, pungent odor. The irritation was enough that the police needed to leave the area. One of the firm’s employees brought the officer a respirator which he donned and re-entered the building.
The deceased’s husband stated in the police report that she could swim.
As part of the MIOSHA investigation, an industrial hygienist performed limited air monitoring for sulfur dioxide (SO2) eight days after the incident occurred. Most of the seasonal cherry brining had been completed, and the air monitoring did not include the brine pumping operation. MIOSHA collected two personal breathing zone samples. The results of both samples were below the MIOSHA 8-hour time-weighted average permissible limit of 2.0 ppm (5 mg/m3) SO2. The industrial hygienist used a Drager hand-held bellows pump and SO2 detector tube to collect an air sample in the airspace above the brine inside the tank the deceased fell into. The concentration measured inside the tank exceeded the detection limit of the tube (25 ppm [65 mg/ m3 SO2]) using only four pump strokes. The detector tube was designed to use 10 pump strokes. Therefore, the atmosphere above the brine in the tank was significantly above the 25 ppm (65 mg/m3) SO2 detection limit of the tube.
After the incident, the employer developed a portable tank opening guard that allowed a sightline into the tank to place the hoses into the holding tank and to monitor cherry/brine levels. The hose openings were small enough to prevent an employee from falling into the tank. (See Figure 9)

|
|
Figure 9. Portable tank opening guard.
|
Back to Top
Cause of Death
The cause of death as listed on the death certificate was brine wet drowning due to hydrocution brine submersion and bronchial fume inflammation due to a fall into caustic brine/cherry mixture. Toxicological tests were negative for alcohol and drugs.
Recommendations/Discussion
Employers should develop, implement, and enforce a comprehensive written safety program for all workers, which include training in hazard recognition and the avoidance of unsafe conditions.
A comprehensive safety program and an annual preseason refresher training program should be developed that includes training in hazard recognition and the avoidance of unsafe conditions. Employers should not allow workers to perform any work until appropriate safety training has been provided for the tasks assigned. In this incident, the deceased had only on the job safety training. MIOSHA Part 1, General Provisions, Rule 11(a) requires that an employer provide training to each newly assigned employee regarding the operating procedures, hazards, and safeguards of the job. Conducting a hazard assessment of all tasks performed by workers is essential in identifying and ultimately controlling potential job-associated hazards. Employers should conduct a hazard assessment of all tasks performed by workers. Once potential hazards are identified, written safe work procedures should be developed that will control these hazards. Employees should then be trained in the implementation of the safe work procedures for any job they might perform.
Had an assessment been performed, the possibility of falling into the tank and the fumes from the brine/SO2 might have been identified as potential hazards.
The opening can be addressed by redesign of the opening cover, or by requiring an employee to be anchored to a suitable anchorage point by a suitable lanyard before approaching the opening with the cover off. The employer might evaluate the use of a standby person if work must be performed near the opening with the cover removed.
The fumes could be addressed by proper ventilation.
Employers should develop and present to workers an annual refresher safety training program for seasonal job tasks.
The cherry operation is a seasonal one lasting from one to three weeks and can be conducted with both long-term employees and seasonal employees. Due to the length of time between the seasons, even long-term employees may not remember what to do and /or the hazards involved. An annual preseason refresher safety training program should be developed and presented to workers to reinforce company safety policy, remind workers about the hazards involved and how to avoid of unsafe conditions.
Employers should develop, implement, and enforce a comprehensive written program for work in permit-required confined spaces, such as the processing brine tanks.
MIOSHA adopted by reference the provisions of 29 C.F.R. 1910.146 entitled “Permit Required Confined Spaces” unless they conflict with specific requirements for confined space entry in any other general industry standard. During the filling of the cherry/brine tank, the tank becomes a permit-required confined space because the tank meets one or more of the characteristics the OSHA standard definition of a permit-required confined space:
- Contains or has a potential to contain a hazardous atmosphere;
- Contains a material with the potential to engulf someone who enters the space;
- Has an internal configuration that might cause an entrant to be trapped pr asphyxiated by inwardly converging walls or by a floor that slopes downward or tapers to a small cross section; and /or
- Contains any other recognized serious safety or health hazard.
The OSHA standard defines entry to mean the action by which a person passes through an opening into a permit-required confined space. Entry includes ensuing work activities in that space and is considered to have occurred as soon as any part of the entrant’s body breaks the plane of an opening into the space. Employee interviews indicated that to check the cherry/brine levels, they would break the plane of the opening with their head to see the cherry distribution within the tank and the effectiveness of the brine recirculation hoses.
Although employees had received some on-the-job training, they had not received adequate training based on OSHA Confined Space requirements for a permit-required confined space program. Since the processing brine tanks fall within this definition, a permit-required confined space program is essential. Such a program has several requirements, which include but are not limited to:
- implement necessary measures to prevent unauthorized entry;
- identify and evaluate permit space hazards (e.g. atmospheric, mechanical, electrical, or other injury hazards) before allowing employee entry;
- establish and implement the means, procedures, and practices to eliminate or control hazards necessary for safe permit space entry operations, and allowing only qualified workers to enter the permit space;
- ensure that at least one attendant is stationed outside the permit space for the duration of entry operations;
- implement appropriate procedures for summoning rescue and emergency services, and preventing unauthorized personnel from attempting rescue;
- establish, in writing, and implement a system for the preparation, issue, use and cancellation of entry permits;
- review established entry operations annually and revise the permit space entry program as necessary.
For a complete list of requirements for written permit-required confined space programs, see MIOSHA General Industry Standard, Part 90, Confined Space Entry.
Additional recommendations regarding safe work practices in confined spaces can be found in the NIOSH Publication No. 80-106, Criteria for a Recommended Standard: Working in Confined Spaces; NIOSH Alert Publication 86-110, Request for Assistance in Preventing Occupational Fatalities in Confined Spaces; NIOSH Publication No. 87-113, A Guide to Safety in Confined Spacespdf icon; and NIOSH Publication No. 94-103, Worker Deaths in Confined Spaces: A Summary of NIOSH Surveillance and Investigative Findings. These publications may be useful in developing confined space safety programs and in training workers to identify hazards found in confined spaces. Specific information provided in these publications includes recommendations for control of hazardous energy, communication procedures, entry and rescue procedures, posted warning signs, and required safety equipment and clothing. NIOSH publications are available through the NIOSH web site at https://www.cdc.gov/niosh/ or by calling 1-800-356-4674.
The employer should develop a tank opening cover that will allow sightline into the tank, hose access, prevent workers from falling into the tank opening, and allow for proper sulfur dioxide (SO2) ventilation.
The company made a good first step to permit operators to perform their required work activities (hose placement and tank cherry/brine monitoring) and prevent the operator from falling into the tank. Engineering controls to minimize SO2 should be implemented while the holding tank is being filled with cherries and brine, as well as at other times where SO2 levels could exceed permissible exposure levels. MIFACE recommends that the company explore options to design the guard with a material that can allow proper SO2 ventilation, allow operators to see through to monitor cherry/brine levels, and not pose a further injury hazard if the employee falls onto it.
The employer should develop and implement a personal protective equipment (PPE) program, including a respiratory protection program, train employees about PPE (including respirators) use and selection, and enforce employee use of designated PPE.
MIOSHA cited the employer for not having a developed and implemented personal protective equipment program and respiratory protection program for employees who voluntarily use a respirator. Personal protection equipment is designed to minimize an employee’s exposure to occupational hazards. The deceased exhibited a skin condition on her left hand that was attributed to chronic brine contact.
The MIOSHA General Industry Standard, Part 33, Personal Protective Equipment, Rule 3308(1)(a-c) requires an employer to conduct a hazard assessment to assess the workplace to determine if hazards that necessitate the use of personal protective equipment are present, or are likely to be present. If the hazards are present or are likely to be present, then the employer is required to do all of the following:
- Select, and have each affected employee use, the types of personal protective equipment that will protect the affected employee from the hazards identified in the hazard assessment.
- Communicate selection decisions to each affected employee.
- Select the personal protective equipment that properly fits each affected employee.
The Personal Protective Equipment hazard assessment provides the employers an opportunity to evaluate the respiratory hazards that may be present in the workplace in addition to selecting an appropriate respirator as required by the MIOSHA Respiratory Protection Standard. MIOSHA adopted by reference the provisions of 29 C.F.R. 1910.134 entitled “Respiratory Protection” as MIOSHA Occupational Health Standard, Part 451, Respiratory Protection. 1910.134(d)(1)(iii) requires that employer identify and evaluate the respiratory hazard(s) in the workplace; this evaluation shall include a reasonable estimate of employee exposures to respiratory hazard(s) and an identification of the contaminant’s chemical state and physical form. Where the employer cannot identify or reasonably estimate the employee exposure, the employer shall consider the atmosphere to be immediately dangerous to life and health (IDLH). 1910.134(d)(1)(iv) requires the employer to select respirators from a sufficient number of respirator models and sizes so that the respirator is acceptable to, and correctly fits the user.
Conducting a hazard assessment of tasks performed by workers is critical to identifying and ultimately controlling occupational hazards. Controlling hazards at the source or along the path of exposure is preferable because it eliminates the exposure to the worker. If the hazard cannot be eliminated or controlled, personal protective equipment should be used to minimize employee exposure to the hazard(s). Personal protective equipment is the least effective approach for minimizing employee exposure because it relies on the worker to select and use the PPE appropriately.
There are many resources on the Internet that employers can use to begin planning a protection strategy. Some resources are:
- MIOSHA: The MIOSHA CET division has sample PPE and respiratory programs on their web site that provides instructions for workplace assessment and development of the programs. MlOSHA CET division web site http://www.michigan.gov/mioshaexternal icon will take you to the MIOSHA web page. Click on the Publications, Forms and Media link. and then click on the Sample Programs and Special Plans link.
- OSHA: OSHA has many resources, included “e-tools” that assist employers in respirator and personal protective equipment (eye and face) program development. OSHA web site: https://www.osha.gov/external icon. Click on “R” for information about respiratory protection and “P” for personal protective equipment.
- CCOHS: Canada’s National Occupational Health and Safety Resource. CCOHS web site: http://www.ccohs.ca/external icon. Click on the OSH Answers link, then click on the Prevention & Control of Hazards link, and then the Personal Protective Equipment link. There are many topics listed, including “Designing an Effective PPE program”.
The employer should reevaluate their organizational commitment and leadership in regards to its safety program.
The employer gave tacit approval to the improper use of respiratory protection. The employer knew that the employers were not properly wearing their respirators i.e., holding the respirator up to their face when they entered the building. One of the objectives of a safety program is to reduce employee exposure to hazards in their workplace. Organizational commitment, management commitment and leadership, and employee motivation and buy-in are necessary to make a safety program effective. The management, by not “saying” anything to the employees about the improper use of respiratory protection, contributed to lax safety work habits by the employees. Other PPE may not have been worn as necessary, i.e., skin and eye protection (the deceased had skin damage from brine exposure). MlFACE recommends that employers audit themselves on their management commitment to safety. There are several examples of management safety audit systems on the Internet that can be modified by for use by any employer:
- International Organization of Oil and Gas Producers: “Checklist for an audit of safety management” http://www.ogp.org.uk/pubs/160.pdfpdf iconexternal iconexternal icon (Link updated 3/20/2008)
- United Kingdom, Health and Safety Commission, Health and Safety Executive: Textile Safety Management System Audit, Parts 1-4
http://www.hse.gov.uk/textiles/audit/part1.htmexternal icon,
http://www.hse.gov.uk/textiles/audit/part2.htmexternal icon,
http://www.hse.gov.uk/textiles/audit/part3.htmexternal icon,
http://www.hse.gov.uk/textiles/audit/part4.htmexternal icon, - OHSAS 18001: OHSAS 18000 is an international occupational health and safety management system specification. It comprises two parts, 18001 and 18002 and embraces BS8800 and a number of other publications. http://www.ohsas-18001-occupational-health-and-safety.com/external icon
The employer should establish a joint health and safety committee.
A health and safety (H&S) committee that includes representatives from both management and labor can help to encourage and heighten employee involvement in the company safety program. Employee input is a critical part of a successful safety program; management can become more aware of potential recurring safety and health hazards in the field and employees can participate in developing safe and healthful work procedures. The level of involvement by employees and degree of management commitment will determine if an H&S Committee is successful.
H&S committees have many benefits; identify safety and health concerns that workers/management consider most critical, help find creative solutions, shows a good faith effort toward health and safety regulations, boosts coworker loyalty, morale and enthusiasm by getting involved in an issue that’s important to everyone, and if new safety rules are needed, an H&S committee can help make sure employees accept and follow them. Employee training needs may also be identified.
Some resources an employer may consult for more information are:
- CCOHS: Canada’s National Occupational Health and Safety Resource, CCOHS web site: http://www.ccohs.ca/external icon. Click on the OSH Answers link, then click on the Health and Safety Programs, Prevention & Control of Hazards link, and then the Health and Safety Committees.
- Industrial Accident Prevention Association (IAPA). Free downloads of health and safety information. Internet web site: http://www.iapa.ca/Main/resources/resources_downloads.aspxexternal icon (Link updated 4/1/2009)
The employer should consider the feasibility of establishing a mode of escape
from inside the cherry holding tank.
It is unknown if the employee was unconscious when she fell into the tank. If she was not unconscious, there was no mode of escape for her and she could have been overcome by SO2 vapors in the headspace of the tank. The employer should consider the feasibility of providing a means of escape from the top of the tank.
MIFACE recommends that the company’s safety and health program include:
Air monitoring during the brining operations to evaluate employee exposure to SO2 to determine whether mechanical ventilation for the brine house is necessary.
On the day of the incident, although the doors and windows were open during the cherry loading/brining operation, building ventilation was most likely deficient due to the minimal natural air movement (wind speed was 0 mph according to the National Weather Service) and the lack of mechanical ventilation provided to the brine house. Rule 3101(6) establishes that a minimum rate of exhaust for places of manufacturing, processing, assembling, maintenance and repair or storage of material be no less than one cubic foot of air per minute per square foot of floor area unless contaminant (in this case SO2) control can be accomplished with a lesser rate of ventilation. Ventilation requires the use of supply and exhaust air to control emissions. exposures, and chemical hazards in the workplace.
Before an appropriate ventilation system can be selected, employers should evaluate emission sources. worker behavior, and air movement in the area. During the cherry loading/brining operation, SO2 levels may be at the “worst-case” scenario, due to the flowing cherries/brine into the holding tanks. the open holding tank covers, the time of year (summer with potential heat, humidity and lack of wind), employee’s weather adaptation (minimal clothing, not wearing PPE properly due to heat considerations), etc. SO2 monitoring in the storage tank room during the loading/brining operation will help the employer determine the amount of ventilation required (natural and/or mechanical) as well as comply with the MlOSHA Respiratory Protection, Part 451 1910.134. The MIOSHA Respiratory Protection regulation (1910.134(a)(1)) requires employers to prevent atmospheric contamination as far as feasible by accepted engineering controls and 1910.134(d)(1)(iii) requires employers to identify and evaluate (reasonable estimation of employee exposures to) the respiratory hazard(s) in the workplace.
| Sulfur Dioxide Level in PPM | Resulting Conditions on Humans |
| Sulfur Dioxide initially detected by taste | |
| 2 | Permissible Exposure Level (MIOSHA) |
| Odor becomes easily detected | |
| 6 – 12 | Irritation of the nose and throat |
| 20 | Irritation of the eyes |
| 50 – 100 | Maximum exposure for a 30 minute period |
| 400 – 500 | Dangerous concentration can cause edema of the lungs and glottis and death from prolonged exposure |
Source: Dangerous Properties of industrial Materials (Sixth Edition) by N. Irving Sax
The Occupational Safety and Health Administration (OSHA) Ventilation web page has many resources for employers to learn about and evaluate the ventilation within their facility. (https://www.osha.gov/SLTC/ventilation/index.htmlexternal icon) Another helpful ventilation resource for general industry employers is the MlOSHA CET division’s Ventilation Control Checkpoints document, which contains questions employers can use as a checklist to evaluate and implement a ventilation system. The document may be found at (http://www.michigan.gov/documents/cis_wsh_cet5955_90295_7.docword iconexternal icon). An experienced professional ventilation engineer can assist in the ventilation system design.
One of the most effective ways of eliminating or reducing exposure to occupational hazards is the substitution of the material posing the hazard with one that is less hazardous. The brine solution poses not only a health issue (low pH, off-gassing of material within confined space) but could also pose an air quality issue due to the high concentration of SO2. MlFACE encourages cherry processors to evaluate alternative chemical options that can still perform the “work” of brining the cherries but also present less hazardous conditions to both humans and the environment. As this experimentation takes place. it is important to ensure that a substituted material does not replace one hazard for another.
References
MlOSHA standards cited in this report may be found at and downloaded from the MIOSHA, Michigan Department of Labor and Economic Growth (DLEG) web site at: http://www.michigan.gov/mioshastandardsexternal icon. MIOSHA standards are available for a fee by writing to: Michigan Department of Labor and Economic Growth, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan 48909-8143 or calling (517) 322-1845.
MlOSHA Consultation, Education and Training (CET) division provides free health and safety consultation to assist Michigan employers in their efforts to provide a safe and healthful workplace. MlOSHA CET personnel can conduct an on-site consultation without the attachment of fines or penalties but employers must agree prior to the start of the inspection to correct all serious violations found. The MlOSHA CET Self-Help Program assists employers in conducting their own evaluations of hazardous exposures in their workplaces. This free service provides limited technical industrial hygiene guidance, monitoring and measuring equipment, sample analyses and general information. For more information about these free services, contact MlOSHA CET division at 1-517-322-1809 or via their web site http://www.michigan.gov/mioshaexternal icon .
- MlOSHA Personal Protective Equipment, Part 433.
- MlOSHA Occupational Health Standard, Permit-Required Confined Spaces, Part 490, 191 0.146, General lndustry Standard Part 90.
- MIOSHA Act 154 PA of 1974 Floor and Wall Openings, Stairways & Skylights, Part 2.
- MlOSHA Medical Services and First Aid, Part 472.
- MIOSHA Hazard Communication Standard, Part 430, 1910.1200.
- MIOSHA Respiratory Protection, Part 451, 1910.134.
- MlOSHA Control of Hazardous Energy Sources, Part 85, Rule 1910.147(c)(4)(i) adopted by Rule 8502.
- OSHA [2004]. Permit-required confined spaces. Occupational Safety and Health Administration (OSHA) Publication No. 3138-01 R 2004.
- Code of Federal Regulations [2004]. 29 CFR 1910.146. Permit-required confined spaces. Washington DC: U.S. Government Printing Office. Office of the Federal Register.
- NlOSH [1979]. Criteria for a recommended standard: Working in confined spaces. Cincinnati, OH: US. Department of Health, Education, and Welfare, Public Health Service. Centers for Disease Control. National Occupational Safety and Health. DHEW (NIOSH) Publication No. 80-106.
- NlOSH [1986]. NIOSH Alert: Request for assistance in preventing occupational fatalities in confined spaces. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service. Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-110.
- NlOSH [1987]. A guide to safety in confined spacespdf icon. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 87-113.
- NlOSH [1994]. Worker deaths in confined spaces: A summary of NIOSH surveillance and investigative findings. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 94-103.
- MlOSHA Consultation, Education and Training (CET) Division. Internet Address: http://www.michigan.gov/mioshaexternal icon
- Occupational Safety and Health Administration (OSHA). Internet Address: https://www.osha.gov/external icon
- CCOHS: Canada’s National Occupational Health and Safety Resource. Internet Address: http://www.ccohs.ca/external icon
- International Organization of Oil and Gas Producers: “Checklist for an audit of safety management” Internet Address: http://www.ogp.org.uk/pubs/160.pdfpdf iconexternal icon.
- United Kingdom, Health and Safety Commission, Health and Safety Executive: Internet address: http://www.hse.gov.uk/textiles/audit/part1.htmexternal icon.
- Industrial Accident Prevention Association (IAPA). Free downloads of health and safety information. Internet web site: http://www.iapa.ca/Main/resources/resources_downloads.aspxexternal icon . (Link updated 4/1/2009)
- OHSAS 18001 Occupational Health and Safety Zone. http://www.ohsas-18001-occupational-health-and-safety.com/index.htmexternal icon
Diagram
Michigan FACE Program
MlFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicineexternal icon, 117 West Fee Hall, East Lansing, Michigan 48824-1315; http://www.oem.msu.edu/MiFACE_Program.aspx. This information is for educational purposes only. This MlFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action. equal opportunity employer. 08/31/06 (Link updated 8/5/2009)
MIFACE Investigation Report # 05MI066 Evaluation (see page 21 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached. Michigan Case Reports