
Young Adult Female Waitress Died From an Asthma Attack While Working in a Bar
Michigan Case Report: 04MI223
Released: April 17, 2006
Corrected: August 08, 2007
Summary
On May 1, 2004, a 19-year-old African-American female waitress working at a bar died from an asthma attack. The bar was divided into two separate areas, the bar area with limited seating and a room with a disc jockey (DJ) booth (See Figure 1). When the victim arrived at work at 9:45 p.m., she talked with the DJ who was setting up in the adjacent room, then walked about 25 feet to an open section of the bar. The bar owner stated she was not experiencing any difficulty breathing at this time. There were approximately 30 people in the bar area. No individuals were in the room with the DJ. According to the owner, the bar was not “overly smoky”. Shortly after the victim went behind the bar, she grabbed the bar manager, saying she needed to get to the hospital and that she needed fresh air. The victim said she wished she had her inhaler with her. As the two walked out from behind the bar and toward the back door, the victim collapsed onto the dance floor. The bar patrons were asked if anyone had an inhaler. Someone did, and the victim attempted to use the inhaler, but was unable to do so. According to the bar manager, the inhaler mist came back into her face. Emergency Medical Service (EMS) was called and she was transported to a local hospital where she was declared dead 30 minutes from the time of the call to EMS.
|
|
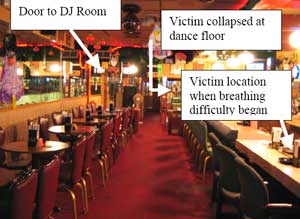
Figure 1. Bar where incident occurred.
|
Recommendations:
- To protect the health of employees, private business owners, including bar and restaurant owners, should consider prohibiting smoking within their establishments.
- Business owners should develop, implement and train employees in the business’ emergency response plan.
Introduction
On May 1, 2004, a 19-year-old African-American female waitress working at a bar died from an asthma attack. MIFACE investigators were informed of this incident by a referral from an asthma study. On September 27, 2005, the MIFACE researcher talked with the owner of the bar where the victim worked and visited the incident scene. The bar owner permitted the MIFACE researcher to take pictures of the establishment. During the writing of this report, the death certificate and medical examiner death scene investigation report were obtained.
The bar has been in business for approximately three years and employs approximately 11 people. There were five employees on site at the time of the incident. The victim worked as a waitress and as a door monitor. She checked for age identification and took cover charges to enter the establishment. The bar served primarily alcohol and food snacks. The victim worked part-time, on an on-call basis to staff the 10:00 p.m. – 2:00 a.m. shift. The victim had been employed at this establishment for approximately three months. She also worked another part-time job at a fast food establishment. The employer did not have an emergency action plan.
Back to Top
Investigation
The bar had two separate areas, the bar area with limited seating and another room with a DJ booth that also sat patrons. The bar area was approximately 18 feet wide and 80 feet long. The front door was very near the area where the victim first began to have breathing problems. (See Figure 1). Walking toward the back door, there was a pool table adjacent to the bar, then a small dance floor. The bar seating accommodated 11 patrons, and had seven tables near the wall, each with four chairs. The room with the DJ booth had a small dance floor, and could be accessed by a standard size door from the bar area. The access door was across from the pool table.
The owner described the ventilation in the bar area as having a “smoke eater”, which drew air from the patron seating area into a 2- to 3-foot high plenum above the drop ceiling (See Figure 2). This drawn air was then discharged above the back door to the outside of the building. There were six rectangular exhaust fans laid on top of the vent panels, presumably to assist in the air discharge to the ceiling plenum (See Figure 3). The “smoke eater” ventilation was working, but the exhaust fans were not turned on at the time of the incident.

|

|
|
Figure 2. Ceiling panels in bar area.
|
Figure 3. Fan laying on ceiling panel in bar area.
|
According to the medical examiner’s report, the victim’s father had seen her at 9:30 p.m. and stated she was having breathing problems at that time.
The victim arrived at work at approximately 9:45 p.m. and greeted her coworkers. She walked into the room with the DJ booth and talked with the DJ for approximately 15 minutes while he was setting up for the evening. After talking with the DJ, she walked through the door to the bar area, walked along the bar to the open area of the bar (See Figure 1). The owner stated that the DJ and the bar manager indicated that she was not experiencing difficulty breathing at this time. There were approximately 30 people in the bar area, and there were no individuals in the room with the DJ. According to the owner, the bar was not “overly smoky”. Shortly after the victim went behind the bar, she grabbed the bar manager, saying she needed to get to the hospital and that she needed fresh air. The victim said she wished she had her inhaler with her. The manager and the victim walked out from behind the bar and toward the back door. The victim collapsed onto the dance floor. The bar patrons were asked if anyone had an inhaler. Someone did, and the victim attempted to use the inhaler, but was unable to do so. According to the owner, the inhaler mist came back into her face.
After her collapse, the bar manager called the owner, who told the bar manager to call for an ambulance. The call was recorded by 911 at 10:06 p.m. The ambulance arrived in five minutes. EMS found her unresponsive, without a pulse and having agonal respirations. Approximately five minutes after EMS arrival, the victim stopped breathing, and EMS started CPR. EMS tried to assist breathing with a mask and bag, but according to the medical examiner report, the EMS personnel could not get air into her lungs. She was transported via ambulance to a local hospital. When she arrived at the hospital, she was unresponsive and the heart monitor showed no heartbeat. She was declared dead at the hospital at 10:36 p.m.
According to the owner, she had not previously had an asthma attack at work. She did not carry her inhaler to work on the day of the incident.
Back to Top
Cause of Death
The cause of death as stated on the death certificate was status asthmaticus. A medical examiner report and toxicology results were not obtained.
Recommendations/Discussion
To protect the health of employees, private business owners, including bar and restaurant owners should consider prohibiting smoking within their establishments.
Ventilation systems, including the most commonly utilized ventilation system – general dilution ventilation – can reduce odor, but fail to guard against environmental tobacco smoke (ETS or secondhand smoke) health dangers. Secondhand smoke is a known asthma trigger. The American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE)1, in their position document on Environmental Tobacco Smoke (June 30, 2005) conclude that:
- “It is the consensus of the medical community and its cognizant authorities that ETS is a health risk, causing lung cancer and heart disease in adults, and exacerbation of asthma, lower respiratory illnesses and other adverse effects on the respiratory health of children.
- At present, the only means of effectively eliminating health risk associated with indoor exposure is to ban smoking activity.
- Although complete separation and isolation of smoking rooms can control ETS exposure in non-smoking spaces in the same building, adverse health effects for the occupants of the smoking room cannot be controlled by ventilation.
- No other engineering approaches, including current and advanced dilution ventilation or air cleaning technologies, have been demonstrated or should be relied upon to control health risks from ETS exposure in spaces where smoking occurs. Some engineering measures may reduce that exposure and the corresponding risk to some degree while also addressing to some extent the comfort issues of odor and some forms of irritation.
- An increasing number of local and national governments, as well as many private building owners, are adopting and implementing bans on indoor smoking.
- At a minimum, ASHRAE members must abide by local regulations and building codes and stay aware of changes in areas where they practice, and should educate and inform their clients of the substantial limitations and the available benefits of engineering controls.
- Because of ASHRAE’s mission to act for the benefit of the public, it encourages elimination of smoking in the indoor environment as the optimal way to minimize ETS exposure.”
The full text of the ASHRAE position document on Environmental Tobacco Smoke may be found at: http://www.ashrae.org/content/ASHRAE/ASHRAE/ArticleAltFormat/20058211239_347.pdf (Link no longer available 11/17/2011)
There is no safe level of exposure to secondhand smoke. Occupational, environmental and public health agencies have recognized that substantial subpopulations with disease states such as asthma or heart disease have their conditions exacerbated by ETS exposure. Air monitoring studies in bars, restaurants and other venues that permit smoking in Massachusetts, Virginia, Minnesota, Delaware and other international locales have shown that the levels of respirable particulate air pollution concentrations inside of these establishments are magnitudes above the respirable particulate air pollution levels found in the outdoor environment; these pollutants are regulated by the Environmental Protection Agency under the National Ambient Air Quality Standard (NAAQS).
According to the American Lung Association State of Tobacco Control: 2005 report:2 “For adult nonsmokers, the workplace is the primary source of secondhand smoke exposure. Levels of secondhand smoke in restaurants and bars are approximately 1.6 times greater and 7.6 times greater, respectively, than in office workplaces. Food service workers have a 50 percent greater risk of dying from lung cancer than the general population”. The American Lung Association Report may be found on the Internet at: http://lungaction.org/reports/tobacco-control05.html (Link no longer available 1/12/2010)
The State of Michigan does not at the time of this report, have a state smoke-free workplace law in place. Private businesses and bars do not have any smoking restrictions; restaurants do have smoking restrictions (i.e. allow smoking in restricted areas). Working in an establishment that permits smoking provides an unhealthy work environment for employees. MIFACE recommends that all private business owners, including owners of bars and restaurants, provide a smoke-free work environment to reduce the risk of their workers developing secondhand smoke-related disease and the exacerbation of existing health conditions.
Business owners should develop, implement and train employees in the business’ emergency response plan.
An emergency situation occurred on the evening of the victim’s death – she had an acute asthma attack. The bar manager did not immediately call 911. Instead she phoned the owner of the bar to let him know what was going on. Only after the owner was contacted was emergency response called. The owner had not developed an emergency response plan. Consequently, valuable time was lost in providing emergency treatment for the victim.
Emergencies can and do happen, including personal injuries, fires, natural disasters such as tornadoes and floods, and violent acts. An emergency action plan describes the actions employees should take to ensure their safety if a fire or other emergency situation occurs.
MIOSHA General Industry Safety Standard Part 6, Fire Exits, Rule 6083 requires that a business with over 10 employees have a written emergency plan. In businesses with fewer than 10 employees, the plan can be communicated orally and need not be in writing. Rule 608 requires that employers inform employees of emergency escape procedures and emergency routes to approved means of egress. In addition, employers must ensure that a sufficient number of persons are designated to assist in a safe and orderly evacuation. MIOSHA General Industry Safety Standard Part 6 may be found and downloaded at: http://www.michigan.gov/documents/CIS_WSH_part6_38111_7.pdfpdf iconexternal icon.
To develop the emergency action plan, identify the potential hazards the business may face. While conducting the hazard assessment, consider hazards to both employees and customers. Potential threats for bars, restaurants, and lounges include but are not limited to: fire, violent acts, tornados, acute illness (e.g., asthma attack, heart attack), the computer “goes down”, water main break, power outage, etc.
After what could go wrong, develop the emergency action plan to address the threats identified. Good business practice, state and local laws and regulations should be considered in the plan development process. The best emergency action plans include the employees in the process and specify what employees should do during an emergency. When employees are included in the planning, it encourages them to offer suggestions about potential hazards, worst-case scenarios, and proper emergency responses.
Designate a person to be in charge of managing the emergency. In this incident, emergency response was unable to provide medical assistance to the victim while inside of the bar due to the intrusion of well-meaning staff and bar patrons. The emergency response personnel needed to take the victim outside to provide medical care. If an individual was designated to be the person “in charge”, and the staff was trained to keep not only themselves away from the scene, but also the bar patrons, EMS would have been able to work and again, time would not have been lost in the medical treatment for the victim.
After the plan is developed, review it with employees to make sure everyone knows what to do before, during, and after an emergency. The emergency plan should be reviewed with all employees not only when it is initially developed, but also when employees’ responsibilities outlined in the plan change, and when the plan itself changes.
To help make sure employees know what’s expected of them in an emergency, consider conducting a “tabletop” exercise. The “tabletop” exercise provides an opportunity to “dry run” the plan and talk over how things might go in an emergency scenario. The “dry run” can provide insight about what might have been missed in your original plan and what might need to be changed in the plan.
Keep a copy of the emergency plan in an easily accessible location that’s convenient to all employees. And, as a best practice, employers should give each employee a copy of the ERP during training and new-employee orientations.
Federal OSHA has an e-tool to assist employers in developing an emergency action plan. The e-tool can be found at: https://www.osha.gov/SLTC/etools/evacuation/index.htmlexternal icon.
Resources
MIOSHA standards cited in this report may be found at and downloaded from the MIOSHA, Michigan Department of Labor and Economic Growth (DLEG) web site at: http://www.michigan.gov/lara/0,4601,7-154-61256_11407_15368—,00.htmlexternal icon (Link updated 4/1/2013). MIOSHA standards are available for a fee by writing to: Michigan Department of Labor and Economic Growth, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan 48909-8143 or calling (517) 322-1845.
- ANSI/ASHRAE Standard 62.1-2004, Ventilation for Acceptable Indoor Air Quality. http://www.ashrae.org/content/ASHRAE/ASHRAE/ArticleAltFormat/20058211239_347.pdf (Link no longer available 11/17/2011)
- American Lung Association. State of Tobacco Control: 2005. Internet Address: http://lungaction.org/reports/tobacco-control05.html (Link no longer available 1/12/2010)
- Department of Labor and Economic Growth, MIOSHA. General Industry Standard Part 6, Fire Exits. http://www.michigan.gov/documents/CIS_WSH_part6_38111_7.pdfpdf iconexternal icon
- US Department of Labor, OSHA. Evacuation Plans and Procedures. Internet Address: https://www.osha.gov/SLTC/etools/evacuation/index.htmlexternal icon
- Effective Emergency Response Plans – anticipate the worst, prepare for the best results. Carl Griffith, Rick Vulpitta. National Safety Council. http://www.nsc.org/issues/emerg/99esc.htm (Link no longer valid 4/16/2007)
Michigan FACE Program
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicine, 117 West Fee Hall, East Lansing, Michigan 48824-1315. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 3/3/06
MIFACE Investigation Report # 04MI223 Evaluation (see page 8 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached. Michigan Case Reports