
Electrician Dies From Being Pinned Between Iron Pipe and Articulated Boom-Supported Aerial Work Platform Control Panel
Michigan Case Report: 03MI146
Summary
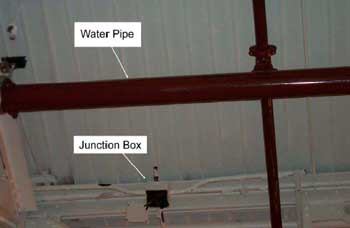
On Monday, November 3, 2003, a 55-year-old electrician had been given an assignment to strip out a section of wiring and conduit from an overhead electrical service. He was operating an articulated boom-supported elevated work platform, JLG Model 660SF, (Figure 1) to access an overhead junction box. Another worker had been assigned as a ground person during this construction activity. The ground person indicated he had walked to the front of the unit when he heard a scraping sound. He called out but received no response. As he called out, he and two other employees looked up saw the decedent pinned with his back against a 6-inch diameter iron fire protection water pipe and his chest against the control panel at the front of the work platform basket. The relationship of junction box and water pipe is shown in Figure 2. They tried to override the basket panel controls (Figure 3) the decedent had been using to operate the work platform, but could not do so, because the key that would allow them to access the controls from the ground was missing from the ground control panel switch (Figure 4). They estimated that three to four minutes passed until they could find a key that allowed them to lower the basket. Another employee used a non-JLG key to gain control of the work platform and lower it to the ground. When they did gain control, the basket and the boom fell abruptly to the dirt floor of the plant. The local fire department and its EMS squad responded to the incident. They found the decedent in the basket on the floor of the plant. Emergency treatment was administered at the plant. He was transported to a local hospital where he was pronounced dead approximately one hour after the incident occurred.
Recommendations:
- The American National Standards Institute (ANSI) should evaluate and consider modifying ANSI A92.S standard titled “The American National Standard for Self Propelled Elevating Work Platforms” and encourage manufacturers and distributors to follow the International Organization for Standardization (ISO) Standard for articulated boom-supported aerial work platforms regarding providing pressure sensor/relief valves on their equipment.
- Limit the number of brands of aerial lifts purchased or leased by a facility.
- Tether the key that operates the equipment from the ground controls to the ground control panel.
- Conduct a written pre-work inspection on equipment and ensure workers do not operate equipment until it is repaired when the pre-work inspection reveals faults such as defeated or missing safety devices.
- Ensure that employee training is appropriate and specific for each type of equipment workers will be using.
Introduction
On Monday, November 3, 2003, a 55-year-old male electrician died when he was crushed between an iron pipe and the control panel of the articulated boom-supported aerial work platform he was operating. On November 4, 2003, MIFACE investigators were informed by the Michigan Occupational Safety and Health Act (MIOSHA) personnel who had received a report on their 24 hour-a-day hotline that a work-related fatal injury had occurred. On November 10, 2004, the MIFACE researcher interviewed a person in corporate safety at the company’s corporate headquarters who had knowledge of the incident. He described the events on the day of the fatality as they had been told to him. The investigator was shown pictures of the site taken after the incident occurred and obtained several for use in this report. During the writing of the report, the medical examiner’s report, the local police department’s incident report, a draft of the company’s internal plant employee fatality report, photographs supplied by the company, and the MIOSHA file and citations were reviewed.
The plant in which the decedent worked builds transmissions for automobiles and trucks. It is one plant in a company that employed approximately 75,000 workers. Approximately 2000 employees worked in this plant. The company was 100 years old; the plant was 75 years old.
The company had a joint labor/management health and safety committee that met at least monthly. The company had joint labor/management health and safety training programs and specific training in how to operate articulated boom-supported aerial work platforms.
The decedent was an electrician. He had been employed by the company and worked in this plant for 32 years. His assignment was to strip out a section of wiring and conduit from an overhead electrical service. He was operating an articulated boom-supported aerial work platform to access an overhead junction box. He was working 8 a.m. to 4 p.m., plus 4 hours overtime. The incident occurred at approximately 4:00 p.m. In accordance with company and plant policy, a ground person was assigned to the area during this construction activity. The ground person had received oral training regarding his duties. The ground person’s duties were to be available on the ground in case the operator encountered an emergency situation, watch from the ground to alert the operator if he was approaching a troublesome situation, and keep the ground area clear of traffic and anything that would obstruct the movement of the aerial lift. Both the ground person and the decedent had received training and were licensed to operate articulated boom-supported aerial work platforms. The training had been given by the plant and by the equipment vendor. The decedent frequently worked with this type of equipment.
The MIOSHA investigation resulted in three Serious violations being issued to the company:
Aerial Work Platforms, Part 32, Rule R408.43207(8) addressed the inadequacy of the instruction and training that had been provided to the employees.
Aerial Work Platforms, Part 32, Rule R408.43208(1) addressed the lack of a visual inspection of the equipment to ensure the ground controls were operational before operation.
Aerial Work Platforms, Part 32, Rule R408.43209(24) addressed the fact that the key necessary for the ground control panel’s emergency control operations was not in the ignition while the employee was operating the equipment.
Back to Top
Investigation
On Monday, November 3, 2003, construction activity was being conducted at a transmission manufacturing plant. An area of the plant had been cleared and the floor torn out such that the working surface was dirt. The decedent had been given an assignment to strip out a section of wiring and conduit from an overhead electrical service. He was operating an articulated boom-supported elevated work platform, JLG Model 660SF, (Figure 1) to access an overhead junction box. He was using this equipment instead of a scissors-lift because the floor was dirt. Another worker had been assigned as a ground person during this construction activity. The ground person indicated he had walked to the front of the unit when he heard a scraping sound. He called out but received no response. As he called out, he and two other employees looked up and observed the decedent pinned with his back against a 6-inch diameter iron fire protection water pipe and his chest against the control panel at the front of the work platform basket. The relationship of the junction box and the pipe is shown in Figure 2. They tried to override the basket panel controls (Figure 3) the decedent had been using to operate the work platform, but could not do so, because the key that would allow them to access the controls from the ground was missing from the ground control ignition switch (Figure 4). They estimated that three to four minutes passed before they could find a key that allowed them to lower the basket. Another employee used a non-JLG key to gain control of the work platform and lower it to the ground. When they did gain control, the basket fell abruptly to the dirt floor of the plant.
The local fire department and its EMS squad responded to the incident. They found the decedent in the basket on the floor of the plant. Emergency treatment was administered at the plant. He was then transported to a local hospital where he was pronounced dead approximately one hour after the incident occurred.
The unit had been rented from an equipment rental company. The decedent’s company required a pre-use inspection be conducted and documented on a written form for this type of equipment, but no written inspection form was found for it on this day. Examination of the unit after the incident revealed that the hydraulic basket tilt cylinder located on the boom had failed catastrophically. The hydraulic tilt cylinder was bent into a “C” shape indicating a large amount of pressure had been exerted on the cylinder. The basket controls were found to be in good working order.
Although no one observed the events immediately preceding the incident, it appears that the decedent was close to the junction box he was trying to access near the plant ceiling but could not quite reach it. As he attempted to reach it, either the controls momentarily malfunctioned driving the articulated arm against a roof truss, or he inadvertently continued to operate the tilt controls after the arm had become wedged against the lower side of a roof truss. The hydraulic lift cylinder failed presumably because of excess pressure exerted on it. When the hydraulic lift cylinder failed, the basket snapped backwards toward an iron water pipe causing the decedent to be crushed. Paint from the roof truss and a scrape were found on the articulated arm near the basket. Paint from the articulated arm was found on the truss. A simulation of where the articulated arm contacted the truss is shown in Figure 5.
According to the manufacturer, the unit was designed such that the key in the ignition switch at the ground controls is held captive when the equipment is engaged in either the platform or ground control mode. No key was found in the switch when the workers tried to operate it from the ground. When the unit involved in the incident was tested with a manufacturer’s key, it was discovered that the key could be removed in either the platform or ground control mode. Control of the unit had been accomplished with a non-manufacturer key at the time of the incident. Interviews with workers familiar with the operation of the articulated boom-supported aerial work platforms indicated that the ground control captive key feature of the equipment could be easily defeated. Also, they indicated that over time the keys became loose, vibrated out of the ignition switch, and were misplaced or lost.
The following actions were taken by the company after the incident occurred.
- The company’s aerial lift standard was reviewed and revised to include:
- Mandatory documentation of all pre-use inspections.
- Conducting a risk assessment before starting a job involving an aerial lift.
- Appointing designated coordinators for aerial lift equipment at each facility.
- Conducting pre-use inspections of purchased, rented or leased aerial lifts prior to commissioning for use in a facility.
- Specifying minimum standards for preventive maintenance tasks.
- Requiring the presence of a ground person for potentially hazardous conditions when an aerial lift is to be operated.
- Documenting written rules for ground persons and requiring successful completion of a written test on the rules.
- Tethering aerial lift keys to the operator’s ground control station.
- Limiting the purchase and leasing of aerial lifts to two brands at a facility in order to standardize the equipment used by aerial lift operators and ensure compliance with regulations that require operator training be designed specifically for the type, make and model of the lift being used.
- Providing lessons on aerial lift safety emphasizing overhead obstructions that could be encountered while in a lift and steps to take if the work platform were to become entangled in the obstructions, because current designs lack the ability to sense and relieve excessive pressure in any of the cylinders.
- Continuing the investigation of the hydraulic system design of boom-supported aerial lifts, because current design systems suggest a lack of a hydraulic relief system in the event of an excessive pressure build-up in any of the cylinders. Current equipment does not contain any type of sensing or warning system for excessive hydraulic pressure. The ISO standard for aerial lifts requires pressure sensing and warning devices be present.
- Establishing communication with the American National Standards Institute (ANSI) committee on aerial lifts (ANSI Standard 92.5). The communication identifies current deficiencies in the standard and requests consideration to adopt the use of load sensing/warning systems similar those used in European aerial lifts.
- Training for aerial lift operators to include provisions added to the company standard such as written tests on the material and refresher training to be required upon expiration of an operator’s license.
Back to Top
Cause of Death
The cause of death as stated on the medical examiner’s report was chest and abdominal injuries. The results of the toxicology tests were negative.
Recommendations/Discussion
The American National Standards Institute (ANSI) should evaluate and consider modifying ANSI A92.S standard titled “The American National Standard for Self Propelled Elevating Work Platforms” and encourage manufacturers and distributors to follow the International Organization for Standardization (ISO) Standard for articulated boom-supported aerial work platforms regarding providing pressure sensor/relief valves on their equipment.
It is not possible to purchase or lease an articulated boom-supported aerial work platform in the United States with pressure sensor/relief valves. This safety equipment is required on all such lifts to be sold and used in Europe in accordance with the ISO standard. Efforts are underway to modify A92.5 of the ANSI standard which emphasizes the location, function, and interlocking of the platform controls for all machine functions to incorporate a requirement that pressure sensor/pressure relief valves be required safety equipment on all boom-supported aerial work platforms. This section also addresses the responsibilities of all involved parties including defining rental inspection and operator education and training.
Limit the number of brands of aerial lifts purchased or leased by a facility.
Operating procedures often are not consistent and cannot be assumed to be consistent between differing types of equipment. Switching between several types of related equipment can be confusing. Limiting the types of equipment workers will be required to operate will help them by reducing and simplifying the amount of information that they need to master to safely operate the equipment.
Tether the key that operates the equipment from the ground controls to the ground control panel.
Because having the key in the ground control ignition in order to operate the work platform apparently is easily defeated and the keys are often missing or lost, tethering the key to the panel would help ensure it was present in case a ground person would have to gain control of the equipment.
Conduct a written pre-work inspection on equipment and ensure workers do not operate equipment until it is repaired when the pre-work inspection reveals faults such as defeated or missing safety devices.
Workers must never become complacent regarding safe practices. The decedent and his partner had received union/company training regarding operating aerial lifts from the plant and from the equipment vendor. A pre-work inspection would have identified the fact that the key was missing. Apparently workers knew that the ground control key was often missing and accepted the fact without having it fixed. Accepting the missing key as a normal situation indicates the safety culture of the plant may need reinforcement. Familiarity with a task often leads to a lax attitude regarding the steps to be followed to perform a job safely. It is not known whether or not gaining control of the overhead basket would have prevented this fatality, but it provides a tragic example of why the key in the ground control is required.
Ensure that employee training is appropriate and specific for each type of equipment workers will be using.
The decedent and his partner had both received training regarding operating aerial lifts, but the incident still occurred. Training that is inappropriate or non-specific with respect to the type of equipment being used is inadequate. It must be expected that equipment pushed beyond its mechanical limits will fail. Knowing the limits of each piece of equipment one is expected to use for work is as important as knowing how to operate it. Workers, particularly those in the skilled trades, are expected to be familiar with many pieces of equipment in order to complete their assignments. Their training must provide them with all the information they need to complete their jobs in a safe manner. Periodic retraining should be conducted when necessary.
References
- MIOSHA standards cited in this report may be found at and downloaded from the MIOSHA, Michigan Department of Labor and Economic Growth (DLEG) web site at: http://www.michigan.gov/lara/0,4601,7-154-61256_11407_15368—,00.htmlexternal icon (Link updated 4/1/2013). MIOSHA standards are available for a fee by writing to: Michigan Department of Labor and Economic Growth, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan 48909-8143 or calling (517) 322-1845.
- DLEG MIOSHA Standard Part 32. Aerial Work Platforms
Figures

|
|

|

|

|
|
Figure 5. Simulation of Arm at Truss
|
Michigan FACE Program
MIFACE (Michigan Fatality Assessment Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicineexternal icon, 117 West Fee Hall, East Lansing, Michigan 48824-1315; http://www.oem.msu.edu/MiFACE_Program.aspx. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. The author of this report is affiliated with Wayne State University. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 6/1/05 (Link updated 8/5/2009)
MIFACE Investigation Report # 03MI146 Evaluation (see page 10 of report)
To contact Michigan State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached. Michigan Case Reports