
A Machine Operator Dies after Becoming Caught in a Computer Numerical Controlled Vertical Milling Machine - Massachusetts
Massachusetts Case Report: 05-MA-035
Release Date: May 26, 2008
Summary
On June 1, 2005, a 37-year-old male machinist was fatally injured when he became caught in the vertical milling machine he was operating at an aerospace parts manufacturer. The victim had reached into the cabinet of the milling machine when the machine cycled, crushing him. A co-worker (co-worker #1) had walked by the machine to let the victim know that it was break time when he noticed that the victim was caught inside the machine. Co-worker #1 had another co-worker (co-worker #2) place a call for emergency medical services (EMS). Multiple co-workers worked to free the victim prior to EMS arriving. EMS transported the victim from the incident location to a local hospital where he was pronounced dead. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers should:
- Ensure that existing and newly purchased machining centers with cabinet doors are equipped with interlocks;
- Develop, implement, and enforce a comprehensive hazardous energy control program including a lockout/tagout procedure and training;
- Provide employees training, in the employees’ primary language(s) and at appropriate literacy levels, on machines they will use, worksite hazards and controls for these hazards;
- Provide frequent supervision of newly-hired and inexperienced employees;
- Periodically perform equipment hazard analyses to ensure equipment is safe to operate;
- Develop, implement, and enforce a comprehensive written health and safety program.
In addition, machining center manufacturers should:
- Ensure that all moveable guards of new numerically controlled and automatic milling machines are safeguarded with interlocks.
Introduction
On June 1, 2005, the Massachusetts FACE Program was notified by a local police department through the 24-hour Occupational Fatality Hotline that on the same day a 37-year-old male machine operator was fatally injured when he was crushed inside the machine he was operating. An investigation was immediately initiated. On June 10, 2005, the Massachusetts FACE Program Director traveled to the incident location and met with several company representatives to discuss the incident. The death certificate, company information, police incident report, and the OSHA fatality and catastrophe report were reviewed during the investigation. In addition, photographs were taken of the machine involved and the incident location.
The employer is a parts manufacturer for the aircraft and aerospace industries. At the time of the incident, the company had been in business approximately 49 years and had 154 employees. Of these employees, 121 worked days and 33 worked nights. The victim was assigned to work the first shift, which started at 6:00 a.m. Employees worked a six day work week of 55 hours. The victim was hired by the company four months prior to the incident. The employer reported that the victim had previous experience as a machinist in this same industry. The victim was born in Vietnam and English was his second language. There was conflicting information about the victim’s level of fluency in English.
The company did not have a written comprehensive health and safety program and did not provide health and safety training to employees. The company did have an employee manual that had some limited information regarding health and safety, such as lockout/tagout. It was company practice to hire only people with three to five years experience in the aircraft/aerospace industry. Newly hired employees were paired with mentors for up to three months. The length of time a new employee was paired with the mentor depended on the mentor’s judgment that the new employee was ready to be on their own. Machine specific training occurred when new equipment was introduced. Typically, the manufacturer of the new piece of equipment would provide training at the company’s location. There is no union representation at this company.
Investigation
The company manufactures aluminum aircraft and aerospace engine components and control system components. The vertical milling machine involved in the incident was manufactured in 1999 and purchased by the company the same year (Figure 1). The company reported that they had not altered the machine since the date it was purchased. Multiple caution signs were affixed to the machine by the manufacturer. One lengthy warning sign includes the statement “Do not clean the machine during automatic operation”.
The basic function of a milling machine is to cut a piece of metal, the work piece, into a product, using a rapidly rotating cutting tool or bit. The milling machine involved in the incident is equipped with a computer numerical control (CNC) system. The CNC system enables a computer program to be written for each specific product. The computer program is then entered into the CNC system, and the CNC system controls the machine to make all of the appropriate cuts to complete the product. The milling machine’s manual controls and an emergency stop button are located immediately to the right of the operator’s area (Figure 1).
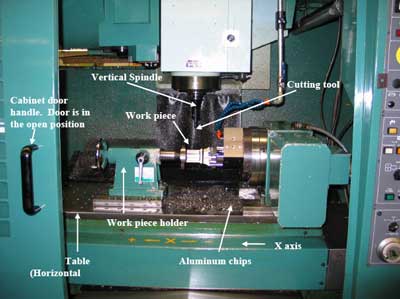
The milling machine is equipped with a cabinet that encloses the entire machine. The cabinet has a sliding door at the operator’s area. When the cabinet’s sliding door is in the open position, the machine’s point of operation (the location where the rotating cutting tool comes in contact with the work piece) is accessible to employees. The cabinet’s sliding door was not equipped with an interlock – a safety device that will override all other machine functions to shut down the machine when the door is opened. Inside the cabinet, at the point of operation, the machine has a table or horizontal platform (approximately three feet high) and a vertical spindle. The table, which has a work piece holder attached to it, moves horizontally side to side (X axis) and back and forth (Y axis). The milling machine’s table does not move vertically (Figure 2).
The bottom section of the vertical spindle is where the cutting tool attaches to the spindle. When the milling machine is operating, the cutting tool rotates rapidly and the entire spindle can move vertically up and down (Z axis). The actual milling process takes place when the rotating cutting tool comes in contact with the work piece and removes material from the work piece.
When the machine operator is attaching a work piece to the work piece holder, the milling machine table is in the start position. In this start position, the table is located directly in front of the operator’s area and the sliding door. At the beginning of a milling cycle, the table moves from the start position along the Y axis towards the cutting tool. This motion along the Y axis toward the back of the cabinet and away from the operator’s sliding door creates a space inside the cabinet between the sliding door and the table.
The type of product being manufactured at the time of the incident had been running for the past 40 days and each piece was estimated to take approximately 1.7 hours to be milled. At the time of the incident, the machine had been set and running in the automatic mode. According to the employer, the victim could have been changing a work piece or using a squeegee to clean up some of the aluminum chip generated during the milling process at the time of the incident. In order to change a work piece or clean up aluminum chips from inside the cabinet, the milling machine’s sliding door would have to be open.
The victim was reaching down inside the machine into the space between the cabinet’s door and the table inside the cabinet when the milling machine cycled. The machine’s cycle moved the table in the forward direction (Y axis) to the start position against the cabinet’s sliding door. The victim’s head was crushed between the table and the front edge of the machine’s cabinet.
At the 8:30 a.m. break time, a co-worker walking to the break room passed the victim’s milling machine and thought that the victim was leaning into the machine, but as co-worker #1 got closer, he realized that the victim was caught in the machine. The co-worker yelled to another co-worker who placed a call for emergency medical services (EMS). Multiple co-workers worked to free the victim. One of the co-workers was then able to use the CNC system to get the milling machine’s table to move away from the victim’s head. The co-workers then removed the victim from the machine and laid him down on the floor. EMS arrived to the incident location within minutes and the victim was transported to a local hospital where he was pronounced dead.
Cause of Death
The medical examiner listed the cause of death as blunt head trauma.
Recommendations/Discussion
Recommendation #1: Employers should ensure that existing and newly purchased machining centers with cabinet doors are equipped with interlocks.
Discussion: An interlock is a safety device that when engaged will override all other machine functions and shut down the machine or prevent the machine from starting. The cabinet’s sliding door on the milling machine involved in the incident was not equipped with an interlock when purchased from the manufacturer. Because the cabinet door did not have an interlock, the door could be opened while the machine was operating allowing employees to come in contact with the machine’s point of operation. In this case, it appears that an interlock on the sliding door would not have interfered with the process of the piece being milled and would have resulted in the machine shutting down when the cabinet door was opened.
When purchasing machining centers with cabinet doors, the employer should ensure that the cabinet doors are equipped with interlocks. If a previously owned machining center is purchased without interlocks on the cabinet doors, then the employer should ensure that the machine is retrofitted with an interlock system prior to the machine being placed in service. When considering altering machines and equipment, including adding interlock systems, the equipment manufacturer and/or mechanical engineers should be consulted.
Recommendation #2: Employers should develop, implement, and enforce a comprehensive hazardous energy control program including a lockout/tagout procedure and training.
Discussion: In this case, the employer had an employee manual that had some limited information on lockout/tagout. OSHA regulation 29 CFR 1910.147, The control of hazardous energy (lockout/tagout) requires that employers establish procedures for isolating machines or equipment from the input of energy by affixing appropriate locks or tags to energy isolating devices. This is done to prevent any unexpected energization, start-up or release of stored energy that would injure workers during service and/or maintenance activities, when employees are required to remove or bypass guarding or safety devices or when employees are required to place any parts of their bodies within the machine’s point of operation. Lockout/tagout procedures should be developed for each machine and address all forms of energy including electrical, hydraulic, pneumatic, and mechanical. A machine’s lockout/tagout procedure should outline the specific requirements and steps to properly perform lockout/tagout on that machine, as well as address when lockout/tagout must be implemented, such as while changing a work piece or cleaning debris from inside a milling machine’s cabinet. For a hazardous energy control program to be effective, the company must provide training to its employees and strictly enforce lockout/tagout procedures.
The review of comprehensive hazardous energy control programs, including the lockout/tagout procedures and associated training, should be performed at least once a year or when safety concerns arise. Involving employees in the process of updating the hazardous energy control program and training is important. The employer should seek input from employees about the effectiveness and limitations of the hazardous energy control program. Employers should ask employees about techniques involved in completing tasks that require employees to expose any part of their bodies to machine hazards, especially maintenance activities and common procedures that are not typically thought of as part of the everyday operation. Employees who spend the majority of their time operating and performing maintenance tasks on equipment will be able to contribute valuable information about the hazards of operating the machine and the effectiveness and limitations of the hazardous energy control program that otherwise might be overlooked.
In this case, the lockout/tagout procedures should include task-specific instructions for when employees will have to expose any part of their bodies to machine hazards to complete these tasks. These instructions should specify that employees entering the milling machine’s cabinet should first lock out the milling machine by de-energizing, isolating, blocking and/or dissipating all forms of the machine’s energy and then affix a lock to secure the energy isolating device. In addition, the employee entering the cabinet must be the only employee with the key to remove the lock in order for the machine to be restarted.
Recommendation #3: Employers should provide employees training, in the employees’ primary language(s) and at appropriate literacy levels, on machines they will use, worksite hazards and controls for these hazards.
Discussion: When employees are hired, employers should provide training that, at a minimum, include both hands on and classroom style training. The training should address how to operate machines and complete tasks safely and should provide information on all known hazards, hazard recognition, the avoidance of unsafe conditions, how to abate identified hazards and which company representatives to contact when safety and health issues arise. Employers should also specify during training that employees should never risk physical harm to accomplish tasks.
Overcoming language and literacy barriers is crucial to providing a safe work environment and effective training for a multilingual workforce. Companies that employ workers whose first languages are not English or do not speak English should identify the languages spoken by their employees and provide and implement multilingual training. If trainings are not conducted in the languages of all employees, a competent interpreter should be present at the trainings. To the extent feasible, the training should be at a literacy level that corresponds with the literacy level of the company’s workforce. This also applies to any training documents that require a worker’s signature. Companies may need to consider providing special safety training for workers with low literacy levels to meet their safety responsibilities.
An assessment of the employees’ knowledge of the material in the training must be performed. Trainings must be documented and the documentation should include who provided the training and their qualifications, the content of the training, workers who were trained, and the assessments of workers’ comprehension of the training.
Recommendation #4: Employers should provide frequent supervision of newly-hired and inexperienced employees.
Discussion: In this case, the employer reported that all new hires are initially paired with mentors, for about three months. The employer also reported that the victim had previous experience in this industry as a machinist. At the time of the incident, the victim had worked for the company for four months and was no longer paired with his mentor.
This incident underscores the need for frequent supervision in the workplace. Frequent supervision should be provided for all employees especially newly-hired and inexperienced employees. Supervisors should be people with the knowledge, training, and experience to routinely evaluate the worker’s performance and competency and with the authority to enforce workplace policies and procedures.
Recommendation #5: Employers should periodically perform equipment hazard analyses to ensure equipment is safe to operate.
Discussion: The milling machine involved in the incident was manufactured in 1999 and purchased by the company involved in the incident that same year. The milling machine was operated for many years without incident. Employers might assume equipment that has been functioning without incident for a number of years is “safe” as designed by the manufacturer. Performing a machine specific hazard analysis might reveal potential hazards that have been previously unnoticed.
It is the employer’s responsibility to ensure a safe workplace for their employees. A hazard analysis is a way of focusing on job tasks to identify hazards to which employees might be exposed. Machine-specific hazard analyses should be performed on all equipment, both new and older equipment, to identify potential and known hazards. Once uncontrolled hazards are identified, the employer should take steps to eliminate or control these hazards. In this case, a hazard analysis of the company’s milling machines might have identified the fact that some of the milling machines were not equipped with interlocks on the cabinet’s sliding door, including the milling machine involved in the incident, and prompted the employer to take steps to control the hazard.
Recommendation #6: Employers should develop, implement, and enforce a comprehensive written health and safety program.
Discussion: The comprehensive health and safety program, developed by employers, should include, but not be limited to, a hazardous energy control program (Recommendation #2), training (Recommendation #3), and all identified and potential hazards and their controls (Recommendation #4). Employers should utilize their employees’ expertise throughout the development process of the comprehensive health and safety program and seek employee input. Once the comprehensive health and safety program is written, employees’ input should continue to be utilized when the program is routinely updated. In addition, the program should be updated when safety concerns arise and when new equipment and new tasks are introduced into the workplace. As a reference, a summary of the Occupational Safety and Health Administration’s (OSHA) draft proposed safety and health program rule, which discusses employee training, has been included at the end of this report.
Recommendation #7: Machining center manufacturers should ensure that all moveable guards of new numerically controlled and automatic milling machines are safeguarded with interlocks.
Discussion: The American National Standard Institute (ANSI) standard B11.23-2002, Safety Requirements for Machining Centers and Automatic, Numerically Controlled Milling, Drilling and Boring Machines states that:
- the machine’s point of operation should be guarded using either fixed guards if access to the location is infrequent, or interlocked moveable guards if routine access to the point of operation is needed for task completion, such as chip removal;
- the machine operation shall only be possible when interlocked moveable guards are closed and the interlocked safeguarding devices are active; and
- if it is possible to open an interlocked moveable guard that the hazardous movement of the machine stops.
References
- Code of Federal Regulations. 29 CFR 1910.212. General requirements for all machines. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- Code of Federal Regulations. 29 CFR 1910.147. The control of hazardous energy (lockout/tagout). Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- NIOSH [1999]. NIOSH Alert: Preventing worker deaths from uncontrolled release of electrical, mechanical, and other types of hazardous energy. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 99-110.
- ANSI B11.23-2002, American National Standard Institute – Safety Requirements for Machining Centers and Automatic, Numerically Controlled Milling, Drilling and Boring Machines.
Illustrations

|
|
| Figure 1. Milling machine involved in the incident with the machine’s cabinet door open. The machine’s manual controls are located to the right of the cabinet door. | |
 |
|
| Figure 2. The milling machine’s point of operation. The cabinet door is open and the table, vertical spindle, cutting tool, work piece, and work piece holder are all visible. | |
|
SUMMARY OF OSHA’S DRAFT PROPOSED |
|
Core elements
Basic obligations
Employee participation
Identify and assess hazards to which employees are exposed
Investigate safety and health events in the workplace
|
Safety and health program record keeping
Hazard prevention and control
Information and training
Program evaluation and maintenance
Multi-employer workplaces
|
Date issued November 23, 1998.
Full text available on https://www.osha.gov/dsg/topics/safetyhealth/nshp.htmlexternal icon. (Link updated 3/21/2013)
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.