
Temporary Laborer was Fatally Injured when Caught between an Idler Pulley and Conveyor Belt at a Recycling Facility - Massachusetts
Massachusetts Case Report: 05-MA-018
Release Date: September 10, 2007
Summary
On March 18, 2005, a 32-year-old Hispanic male temporary laborer (the victim) was fatally injured when he became caught between a screening/recycling system’s idler pulley and a conveyor belt at a recycling company. The victim was helping his brother, who was a full-time employee of the company, realign the conveyor belt when he became caught between the conveyor belt and the idler pulley. Coworkers attempted to free the victim and notified Emergency Medical Services (EMS). EMS responded to the incident site within minutes and pronounced the victim dead at the incident site. The Medical Examiners Office was notified and arrived to remove the victim’s body. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers should:
- Ensure that all exposed and accessible sections of conveyors are guarded
- Routinely conduct a job safety analysis (JSA) to ensure equipment and current practices are safe
- Designate only workers who have been trained to perform or assist in required machine maintenance tasks
- Ensure that all workers have knowledge of worksite hazards by providing safety training in the workers’ primary language(s) and at appropriate literacy levels
- Ensure that workers employed through temporary agencies are provided site and task specific safety and health training
- Develop, implement, and enforce a comprehensive hazardous energy control program including lockout/tagout procedures and routinely review and update the program and training.
In addition, manufacturers of equipment with conveyors should::
- Ensure that all moving sections of conveyors are guarded
- Consider installing pull cable emergency stops that surround the accessible sections of conveyors.
Introduction
On March 25, 2005, the Massachusetts FACE Program was notified by a town clerk through the 24-hour Occupational Fatality Hotline that, on March 18, 2005, a Hispanic male temporary laborer was fatally injured when he became trapped in a conveyor belt. An investigation was initiated. On April 15, 2005, the Massachusetts FACE Program Director traveled to the incident location where representatives of the company, including the environmental manager and the safety manager, were interviewed. The death certificate, police report, corporate information, and the OSHA fatality and catastrophe report were reviewed. Photographs were taken of the incident location.
The employer is a solid waste disposal and recycling company that had been in business for approximately 30 years at the time of the incident. The company provides services to residential, commercial, and municipal clients. The company has 60 locations in 16 states; 12 of their locations are in Massachusetts. The company purchased the facility, where the incident occurred, 1½ years before the incident. At the incident location, the company employed approximately 34 workers. Fifteen of these workers were full-time employees, which included the victim’s brother. The remaining 19 workers, including the victim, were temporary workers. The company reported that temporary workers held job titles such as debris sorters and general laborers. All of the temporary workers were hired through one temporary agency. The victim had been working at the company through the temporary agency for approximately three weeks at the time of the incident. It was reported by company representatives that the victim had worked in the recycling industry while living in Guatemala, prior to coming to the United States. The company’s typical workday was a ten hour shift. The typical work week was Monday through Saturday. Not every employee worked Saturdays and the employees that did work Saturdays typically did not work a full ten hour shift. At the time of the incident, at least two supervisors on-site were bilingual and spoke English and Spanish. The victim spoke only Spanish.
The company had a designated person in charge of employee safety and health, and a safety and health program, which addressed lockout/tagout, hearing protection and blood borne pathogens. The company provided full-time employees classroom and on-the-job training. An interpreter was available for the Spanish speaking employees at the trainings. Employees’ comprehension of the training was performed by testing the employees’ knowledge as a group. There was no documentation of the trainings. Prior to this incident, training was not made available to temporary workers. The employer also held weekly tool box talks and biweekly safety committee meetings, although there was no documentation of these tool box talks, safety committee meetings and trainings. Employees were not part of a union collective bargaining unit.
Investigation
The incident site is a construction debris processing and recycling facility (Figure 1). The main function of the site is as a transfer station. Debris from demolition work on construction sites is brought to the facility where it is sorted, screened, and recycled. The company had two similar systems at the incident location side by side that recycled debris. The screening/recycling system involved in the incident was manufactured in 1998. The company purchased the system from a company in the Netherlands in 2004, one year prior to the incident. The system was equipped with an emergency stop and emergency cable at each manual sorting station.
The process of sorting, screening, and recycling the debris begins once the debris arrives at the facility. The debris is transported to the facility by trucks and is offloaded into piles. Excavators with grapple attachments are used to place the debris piles into the screening/recycling system’s hoppers (Figures 2 and 3). The bottom section of the hoppers is the start point of the two feed conveyor belts. The feed conveyor belts for this system are 52 inches wide and 12 feet long. During normal use, the belts move approximately 20 feet per minute. The feed conveyor belts transport the debris past two employees (sorters) who manually pick out of the debris large objects, such as wood, metal, and concrete pieces, as the debris passes by them.
After the debris passes the sorters, it enters a size selective screening section of the system. Debris that is smaller than two inches passes through the screens and lands on a second conveyor. The debris on this second conveyor is then loaded into a dump truck (Figure 4). The debris that does not pass through the screen is transported to the larger sorting area via the feed conveyor. At this sorting area, there are typically 15 laborers, all temporary workers, who manually pick pieces of metal, wood, and concrete out of the debris. The debris remaining on the conveyor then passes under a magnet that collects smaller sized metal pieces. The conveyor then continues to a grinder and the remaining debris is ground down to pieces with a maximum size of six inches. This debris is then stockpiled at the facility.
Routine maintenance for the screening/recycling systems typically occurs on Saturdays, at which time approximately six to eight full-time employees work a four hour shift. During this maintenance time the plant is shut down. The routine maintenance performed consists of greasing and oiling the equipment, and changing filters. The company reported that only full-time employees, not temporary workers, perform the maintenance of the equipment.
On the day of the incident, a Friday morning, employees arrived at the facility at approximately 6:30 a.m. The temporary agency provided a van to pick up the temporary workers and transport them to the work site. Some of the temporary workers did not utilize the van service and provided their own transportation to the worksite. When the workers arrived, the plant was not operating because no construction debris had been delivered that morning. Because no debris material was delivered, the temporary workers could not perform all of their normal tasks and were assigned other tasks that included general cleanup, and picking up litter at the fence surrounding the property.
To take advantage of the facility’s downtime due to the absence of debris being delivered, the company decided to perform the typical Saturday maintenance tasks. Since the routine maintenance work was going to be completed that day, Friday, the facility then planned to be closed the next day, Saturday. In addition to the routine maintenance tasks, there was one other maintenance task planned this day – to repair/adjust one of the feed conveyor belts. The conveyor belt was partially off of a pulley and needed to be adjusted.
The victim and his brother were assigned to the maintenance task of realigning the conveyor belt (Figure 5). At the time of the incident, approximately 8:00 a.m., the victim and his brother had already made one adjustment to the conveyor belt with the conveyor turned off. The victim’s brother then went to the screening/recycling system’s control area to turn on the conveyor so they could observe the belt’s motion. After this first adjustment the belt was still not perfectly aligned, and the victim’s brother went back to the screening/recycling system’s control area to turn the machine back off while the victim stayed by the conveyor belt (Figures 2 and 5). After turning off the machine, the brother returned to the conveyor belt and found the victim caught in the in-running nip point between the conveyor belt and an idler pulley. Nearby coworkers attempted to free the victim by cutting the conveyor belt, but they were unsuccessful.
Coworkers called 911 and the local police department who arrived at the incident location within minutes. The victim was pronounced dead at the incident site and the Medical Examiners Office was notified to remove the victim’s body. Since the incident, the company has enhanced their lockout/tagout program, started providing training to all workers, including temporary workers, and has upgraded machine guarding.
Months prior to the incident, this same feed conveyor had been in repeated need of adjustment. The company replaced the belt with a new belt approximately five weeks prior to the incident. At the time of the site visit, the employer suggested that the new conveyor belt could have stretched between the date it was installed and the date of the incident causing the belt to shift off the pulleys. It was also suggested by the employer that the victim may have been retrieving a fallen tool when he became caught.
Cause of Death
The medical examiner listed the cause of death as multiple traumatic injuries.
Recommendations/Discussion
Recommendation #1: Employers should ensure that all exposed and accessible sections of conveyors are guarded.
Discussion: Rotating parts on machines can be dangerous if not properly guarded. Even machine parts that are moving slowly and smoothly, such as some conveyors, can grip clothing and skin and cause an employee to become caught. There are federal regulations (29 CFR 1910.212)1 that specifically require machine guarding. The OSHA regulation states “One or more methods of machine guarding shall be provided to protect the operator and other employees in the machine area from hazards such as those created by point of operation, ingoing nip points, rotating parts, flying chips and sparks.”
In this case, the hazard that existed on the screening/recycling system was an unguarded in-running nip point created as the moving conveyor belt passed over the idler pulley. Although this unguarded section of the screening/recycling system’s conveyor was located partially underneath the machine, it was still an accessible and exposed moving machine part and should have been guarded either with a point of operation guard or a barrier guard. When considering altering a piece of equipment, including adding a guard, employers should consult the manufacturer of the equipment and an engineer prior to the alteration.
Recommendation #2: Employers should routinely conduct a job safety analysis (JSA) to ensure equipment and current practices are safe.
Discussion: A job safety analysis (JSA) is a way to evaluate how to perform tasks safely and to identify all potential hazards and hazardous situations that could occur when performing tasks, such as aligning a conveyor belt. A JSA should be routinely performed on all equipment, both new and existing, to identify uncontrolled hazards. Once hazards are identified, the employer should take steps to eliminate or control these hazards.
Employers should not assume that new equipment is “safe” as designed by the manufacturer. Although the screening/recycling system involved in the incident was six years old at the time of the incident, a section of the conveyor was unguarded. A hazard analysis of the system by the employer might have revealed this hazard leading the employer to take steps to eliminate this hazard.
Recommendation #3: Employers should designate only workers who have been trained to perform or assist in required machine maintenance task.
Discussion: The victim was not specifically trained in how to properly adjust the screening/recycling system’s conveyor belts and in the safety hazards associated with this task. The employer reported that after the first conveyor belt adjustment, the victim stayed by the conveyor belt while the victim’s brother went to turn off the machine. If the victim had been trained and fully understood hazards associated with moving conveyors, such as in-running nip points, he may have positioned himself away from the moving conveyor, minimizing the danger of becoming caught between the conveyor and an idler pulley.
This incident underscores the importance of ensuring that all employees assigned to perform or assist in maintenance tasks are trained in the proper procedures involved in completing these tasks safely. Also this incident underscores the importance of ensuring that all employees have a basic understanding of the hazards that exist in their workplace even if their assigned tasks do not directly place them near the hazard.
Recommendation #4: Employers should ensure that all workers have knowledge of worksite hazards by providing safety training in the workers’ primary language(s) and at appropriate literacy levels.
Discussion: Overcoming language and literacy barriers is crucial to providing a safe work environment for a multilingual workforce. Companies that employ workers who do not understand English should identify the languages spoken by their employees and design and implement multilingual training. To the extent feasible, the training should be developed at a literacy level that corresponds with the literacy level of the company’s workforce. This also applies to any training documents that require a worker’s signature. Companies may need to consider providing special safety training for workers with low literacy levels to meet their safety responsibilities.
The training should address all known hazards, required safe work practices, specific safety protection for all tasks performed, methods to identify and avoid hazards, and company representatives to contact when safety and health issues arise. A competent interpreter should be present at all trainings, or trainings should be conducted in the languages of all employees. An assessment of the employees’ knowledge of the material in the training must be performed. Trainings must be documented and the documentation should include who provided the training and their qualifications, the content of the training, workers who were trained, and the assessments of workers’ comprehension of the training.
Recently, OSHA has developed a Web page designed to assist employers in providing health and safety information to Spanish speaking employees. The Compliance Assistance: Hispanic Employers and Workersexternal icon Web page covers topics such as workplace rights and responsibilities, Spanish-language outreach/training resources, and OSHA cooperative programs. The Web page is available at www.osha.gov/dcsp/compliance_assistance/index_hispanic.html or can be obtained by contacting an area OSHA office.
Recommendation #5: Employers should ensure that workers employed through temporary agencies are provided with site and task specific safety and health training.
Discussion: Employees of temporary agencies should be provided general safety and health training by the temporary agency. Companies that contract with temporary agencies are responsible for providing site and task specific safety and health training to the temporary employees. In addition, if temporary employees are hired out to one company for a long time period, then the temporary employees should be provided with annual refresher training that should include any new hazards at the workplace.
Recommendation #6: Employers should develop, implement, and enforce a comprehensive hazardous energy control program including lockout/tagout procedures and routinely review and update the program and training.
Discussion: In this case, the employer had a hazardous energy control program that included lockout/tagout procedures, but these procedures were not comprehensive. OSHA regulation 1910.147 requires that employers establish procedures for isolating machines or equipment from the input of energy by affixing appropriate locks or tags to energy isolating devices2. This is done to prevent any unexpected energization, start-up or release of stored energy that would injure workers during servicing and maintenance of machines and equipment. All forms of energy must be considered, including electrical, hydraulic, pneumatic, and mechanical. Therefore, for each machine an individual lockout/tagout procedure is needed that specifies the requirements to properly perform lockout/tagout on that machine, as well as when the lockout/tagout should be implemented, such as while realigning a feed conveyor belt that is part of a screening/recycling system.
A machine specific lockout/tagout program should be documented in writing and include, but not be limited to:
- Identification and labeling of all hazardous energy sources
- Procedures to de-energize, isolate, block, and/or dissipate all forms of hazardous energy, and verify by tests and/or observations that all energy sources are de-energized before work begins
- Requirements that workers secure the machines’ energy control devices with their own individually assigned locks and keys, and that:
- Each lock assigned to a worker only has one key for regular use, which is held by that worker
- Locks are clearly labeled with durable tags to identify the worker associated with the lock
- Workers who install locks are the only ones who remove the locks
- Requirements that if work is not completed when the shift changes, workers arriving on shift apply their locks before departing workers remove their locks
- Inspecting repair work before reactivating the equipment
- Ensuring that all workers are clear of danger points before re-energizing the system
- Inspecting each energy control procedure at least annually, to ensure that the procedures and the requirements of the OSHA standard are being followed
Involving employees in the process of inspecting and updating the hazardous energy control program and training is important. The employer should seek input from employees by having employees evaluate the effectiveness and limitations of the hazardous energy control program. Employers should ask employees about techniques involved in completing tasks that require them to expose any part of their bodies to machine hazards, especially maintenance activities and common procedures that are not typically thought of as part of the everyday operation, such as realigning conveyor belts. Employees who spend the majority of their time operating and performing maintenance tasks on equipment will be able to contribute valuable information that might have been overlooked, and these employees will likely be able to contribute the most information about the effectiveness and limitations of the hazardous energy control program.
A comprehensive hazardous energy control program is not going to be effective if the employer does not strictly enforce the procedures outlined in the program. Enforcing a hazardous energy control program should include random inspections of employee work habits related to procedures outlined in the hazardous energy control program.
Recommendation #7: Manufacturers of equipment that have conveyors should ensure that all moving sections of conveyors are guarded.
Discussion: At the time of this incident, a section of a feed conveyor that was located partially underneath the machine was not guarded. Manufacturers should design point of operation guards for all sections of conveyors where in-running nip point hazards exist. In addition, if manufacturers have unguarded sections of conveyors on older models, they should consider designing retrofit guards for these models and contact purchasers of the equipment to inform them that an additional safety feature is available.
Recommendation #8: Manufacturers of equipment with conveyors should consider installing pull cable emergency stops that surrounds accessible sections of the conveyors.
Discussion: Emergency stops are a safety feature that overrides all other controls located on the machine. When an emergency stop is activated, the machine is immediately shut down. In this case, a pull cable emergency stop3 could have surrounded the accessible sections of the machine’s conveyor in addition to the pull cable that was located at the manual sorting areas.
References
- Code of Federal Regulations, 29 CFR 1910.212 Machinery and Machine Guarding, General requirements for all machines, Government Printing Office.
- Code of Federal Regulations, 29 CFR 1910.147 General Environmental Controls, The control of hazardous energy (lockout/tagout), Government Printing Office.
- Honeywellexternal icon, Sensing and Control, Safety Cable Pull Switch for Emergency Stop, http://honeywell.com/Pages/Home.aspx (Link updated 3/27/2013)
Illustrations
 |
 |
|
Figure 2 – Debris pile, system’s conveyor belt and hopper, and incident location |
 |
|
Figure 3 – Excavator with grapple loading debris into the system’s hopper |
 |
|
Figure 4 – First manual sorting location and dump truck being loaded |
 |
|
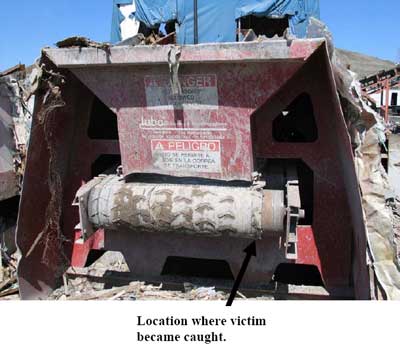
Figure 5 – Location of incident and conveyor belt |
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.