
Vessel Mechanic Drowns after Falling from a Ladder Between a Tugboat and the Dock - Massachusetts
Case: 02-MA-010-01
Release Date: May 26, 2004
SUMMARY
On May 9, 2002, a 38-year-old male vessel mechanic (the victim) drowned when he fell approximately 13 feet from an aluminum ladder that was being used as to access a tugboat from a pier. The victim was on site to assist in repairing the vessel when a coworker found him in the water between the tugboat, a wooden bumper and the pier. The victim was transported to an ambulance by the United States Coast Guard and brought to a hospital where he was pronounced dead. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers should:
- ensure that all articulated tug barge (ATB) unit’s tugs are outfitted with gangways
- ensure that vessels are only docked at designated docking locations
- provide and require the use of U.S. Coast Guard personal flotation devices
- train employees in procedures to safely board and disembark a docked tugboat
INTRODUCTION
On May 10, 2002, the Massachusetts FACE Program was alerted, by the local media, that on May 9, 2002, a worker drowned after falling from a boat. An investigation was initiated. On June 5, 2002, the Massachusetts FACE Program Director and an investigator traveled to the incident location where a company representative was interviewed. The police report, death certificate, corporate information and the Occupational Safety and Health Administration (OSHA) fatality/catastrophe report were reviewed during the course of the investigation.
The employer, a marine-based petroleum transportation company with headquarters in both New York and Massachusetts, had been in business approximately 79 years at the time of the incident. At the time of the incident, the company employed approximately 450 individuals. Of these employees approximately 30 held the same job title as the victim, shore based mechanic. The majority of the shore based mechanics, including the victim, worked out of the New York office. The company had specific representatives responsible for safety and health in both the New York and Massachusetts locations, and had written safety and health procedures specific to each location. Neither set of safety and health procedures included a section related to tugboat access. However, sections on other topics such as lockout/tagout and confined space entry were included.
The victim had been employed with the company at the New York location as a shore based mechanic for approximately 8 months at the time of his death. There was union representation for employees at both the New York and Massachusetts locations. The victim’s training was primarily on the job.
INVESTIGATION
The style of the vessel involved in the incident was a new style tug and barge combination called an articulated tug barge unit (ATB). Unlike the older integrated tug/barge style, the ATB has a hinged connection system between the tug and barge. The ATB system “couples” the tug and barge together. The ATB unit’s barge has a notch in the stern where its tug bow fits. Pins are located on both sides of the tug’s bow that extend out and into the barge locking the vessels together. An ATB tug can be separated from the barge and used alone. At the time of the incident, the ATB technology was approximately six years old and five ATBs were in use on the East Coast.
The tug involved in the incident, manufactured in 1999, was a 7,200 horsepower twin-screw tug that was 124-feet long and 40-feet wide. At the time of the incident, the tug was unattached from its barge. The double-hulled barge was 460 feet long and designed to hold 135,000 barrels of fuel. An ATB crew usually consists of nine members, which is smaller than the typical crew size of an older style tug.
The day of the incident, the tug and barge were in the Massachusetts area delivering fuel. The tug needed repairs to the engine and one of the coupling system gearboxes located inside the engine room several decks below. The tug, which is not a functional part of the offloading process, was disconnected from the barge and brought to the Massachusetts dock location for the repairs. The labor-intensive repair process, which was estimated to take one day to complete, was going to be performed during the several hours of downtime while the product was being offloaded from the barge.
The victim, a shore based mechanic out of the New York office, drove from the New York office to the Massachusetts office to assist with the repairs. In addition, a representative from the ATB manufacturer was also on site supplying technical support during the repairs, for warranty purposes. The tug arrived at the Massachusetts office location at approximately 11:00 a.m. and the victim arrived at the Massachusetts office an hour prior to the tug. The weather on the day of the incident consisted of light winds, calm seas, and a temperature of about 60 degrees Fahrenheit. Around the time of the incident, the tide at the Massachusetts office location was approximately two hours before low tide and low tide was estimated to be 1.2 feet above sea level.
It was estimated that the Massachusetts location had approximately three hours notice that the tug was going to arrive for repairs. Because the Massachusetts location had not been notified about the repair, the docking slips at the Massachusetts pier were occupied with Massachusetts based tugs. It was reported by the company representative that they were unable to free up a docking slip for the arriving tug because few Massachusetts tug operators were onsite at that time. The majority of the tug operators (at the Massachusetts location) were on call as fulltime employees.
When the tug arrived at the Massachusetts location, it was docked across the end of one pier with the tug’s front starboard side (right side) against the dock. Boarding and disembarking the vessel was performed using an aluminum extension ladder that was kept with the vessel. The ladder was 12 feet long and both the top and bottom rungs were damaged. The sides of an ATB are higher than a conventional tugboat; therefore, a ladder placed against the side of an ATB is typically pitched on an incline from the dock up to the boat’s side creating an awkward walking/climbing surface. It was reported that one end of the ladder was lashed down, but it was unknown if it was the end on the dock or the tug.
Approximately three hours into the repair, a truck located on land had to be moved. The victim volunteered to move the truck and disembarked the tug alone. While re-boarding the tug one end of the ladder slipped off of either the dock or the tug causing the victim to fall approximately 13 feet from the aluminum extension ladder into the water. A co-worker found the victim head down in the water between the tug and a large wooden bumper that was against the dock. A call for emergency assistance was placed and personnel from fire and police departments responded within minutes. Emergency Medical Service (EMS) personnel arrived at the incident site and the victim was transported by a fireboat with EMS personnel to a local Coast Guard base where an ambulance was waiting to take the victim to a hospital. The victim was pronounced dead at the hospital.
CAUSE OF DEATH
The medical examiner listed the primary cause of death as drowning and blunt head trauma as an underlying contributing cause but not resulting cause in the death.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that all articulated tug barge (ATB) unit’s tugs are outfitted with gangways.
Discussion: At the time of the incident, ATB technology was new. The sides of ATB tugs are higher compared to conventional tugs. With sides higher than conventional tugboats, when a ladder is placed against the side of an ATB it’s typically pitched on an incline from the dock up to the boat’s side creating an awkward walking/climbing surface.
All ATB style tugs should be outfitted with gangways and the gangways should be used whenever boarding and disembarking ATB tugs. If the ATB involved in the incident had been outfitted with a gangway the victim would have had a solid no slip walking surface with guardrails, reducing the possibility of the victim falling in between the vessel and the dock.
Recommendation #2: Employers should ensure that vessels are only docked at designated docking locations.
Discussion: The day of the incident, no docking slips were available at the Massachusetts pier. It was reported that this location had approximately three hours notice that the tug was arriving for repairs. Arrangements should have been made by the employer to have a docking location available by the time the vessel arrived. If the employer was unable to free up a docking location then the repair should have been postponed until the tug was back at its home port, approximately one week later. If the tug’s repairs were urgent then the tug should have been pulled out of service for the repairs.
Recommendation #3: Employers should provide and require the use of U.S. Coast Guard personal flotation devices.
Discussion: Employers should provide and require the wearing of U.S. Coast Guard approved personal flotation devices (PFDs), such as life vests, for each employee engaged in work in which the employee might fall into the water. These tasks might include but are not limited to, working within a few feet from the edge of a vessel or dock/pier and when boarding and disembarking vessels.
Recommendation #4: Employers should train employees in procedures to safely board and disembark a docked tugboat.
Discussion: Gangways that have a solid no-slip walking surface with guardrails are safer to board or disembark an ATB tug than using a ladder. Employers should provide training to employees about how to safely board and disembark an ATB tug using a gangway and the proper procedures of setting up a gangway. In addition, the training should include recognition and avoidance of hazards, such as falling between the tug and dock and when to use a gangway.
REFERENCES
- U.S. Army Corps Safety and Health Requirements Manual – Section 19, Floating Plant and Marine Activities, September 1996, Publication Number 385-1-1
- American National Standards Institute Safety (ANSI), Code for Portable Metal Ladders, A14.2-1990.
- Code of Federal Regulations, Labor 29 Parts 1915.72 Scaffolds, Ladders and Other Working Surfaces, Ladders.
- Code of Federal Regulations, Labor 29 Parts 1915.74 Scaffolds, Ladders and Other Working Surfaces, Access to vessels.
ILLUSTRATIONS
|
|
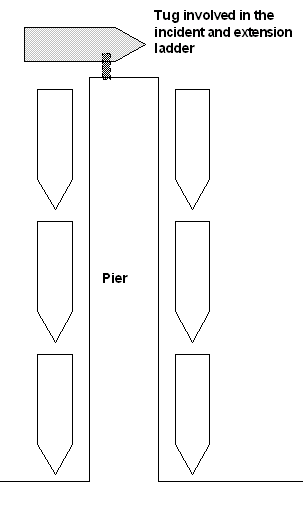
Figure 1 – Diagram of the incident site.
* Not drawn to scale |

|
|
Figure 2 – Massachusetts location
|
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.