
State Worker Fatally Injured While Operating a Bulldozer at a State Mental Health Facility – Massachusetts
Investigation: # 00-MA-069-01
Release Date: September 19, 2002
SUMMARY
On December 29, 2000, a 37-year-old male equipment operator was fatally injured when he was run over by the bulldozer he was operating at a state mental health facility. While moving the bulldozer into the blacksmith shop, the victim slowed or stopped the bulldozer and climbed out of the bulldozer’s operator area. Once standing on the ground, the victim tried to climb back into the operator’s seat when he became caught on the bulldozer track and was run over. Two co-workers in the immediate area placed a call for emergency assistance and then went to assist the victim. The campus police were on the scene within minutes along with an ambulance, which transported the victim to a local hospital where he was pronounced dead approximately six hours later. The Massachusetts FACE Program concluded that to prevent similar occurrences in the future, employers, including state facilities, that utilize bulldozers should:
- train all bulldozer operators on health and safety aspects of the equipment including proper steps to follow when stopping and exiting the bulldozer
- develop, implement and enforce a comprehensive health and safety program that includes but is not limited to procedures for entering, exiting and stopping bulldozers
In addition, all states without state OSHA plans should:
- explore options to ensure that state and municipal workers are provided with the same health and safety protection as their private sector counterparts
Also, crawler bulldozer manufacturers should:
- consider equipment engineering design changes, such as developing a step to prevent the operator from stepping on the track while entering or exiting the bulldozer cab
INTRODUCTION
On January 3, 2001, a local city health department notified the Massachusetts FACE Program through the 24-hour Occupational Fatality Hotline, that on December 29, 2000, a 37-year-old male equipment operator was fatally injured when he was run over by a bulldozer. An investigation was immediately initiated. On January 23, 2001, the Massachusetts FACE Program Director traveled to the campus of the state facility where the manager and one coworker were interviewed. The campus police report, death certificate, and the bulldozer operator/maintenance manual were obtained during the course of the investigation.
The incident site, a state owned residential facility for the mentally retarded, had been in operation approximately 100 years at the time of the incident. The facility employed approximately 400 individuals, 16 of them, including the victim, were part of the farm crew. The facility did not have a designated individual in charge of safety nor a comprehensive health and safety program.
The victim, a union member, was employed at the facility for approximately 17 years at the time of his death. During the first eight years of his employment at the facility, he worked as a vocational instructor, and during the nine years prior to the incident, he worked as an equipment operator. His training at the facility was primarily on-the-job, including demonstrations by senior personnel. There were five bulldozer operators at the facility, including the victim, and all of them were licensed through the Massachusetts Department of Public Safety as 2A hoisting machinery operators.
INVESTIGATION
The facility was a self-sufficient residential community for mentally retarded adults. Home to approximately 160 residents, the facility consisted of 2,600 acres of which 350 acres were maintained as a functioning farm.
Employees of the facility held a wide range of jobs including but not limited to clinical (e.g. registered nurses), farming, maintenance, food services, and clerical positions. All maintenance and repairs to various, equipment including farm equipment, construction equipment, and different workshop machines, were performed on site by the employees. In addition, some residents held part-time jobs at the facility producing and selling wood products, operating a farm stand, and maintaining small assembly lines for local businesses to help with the facility’s funds.
The facility owned three crawler bulldozers. The bulldozer involved in the fatality was used most often, approximately 10 times a year. This bulldozer was a nine-ton machine with a four-cylinder diesel engine. It had a dozer blade attachment in the front (Figure 1) and was equipped for a backhoe attachment in the rear. The bulldozer was purchased new approximately 13 years ago. The dealer had provided instructions on how to operate the bulldozer upon delivery. The victim was not an equipment operator at the time of purchase and was subsequently trained by senior employees. The bulldozer was not equipped with an auxiliary (“pony”) engine.
At the time of the incident, all five of the bulldozer operators had current state operator’s license through the Massachusetts Department of Public Safety for crawler dozer style equipment. Typical tasks the bulldozer had been used for included road grading, trench style silo packing, and snow removal with the dozer blade. In addition, ditch digging and stump pulling were performed with the backhoe attachment.
The bulldozer had not been used and was stored outdoors for five weeks prior to the incident. On the day of the incident, due to a forecasted snowstorm for that night, the bulldozer was being moved inside the blacksmith shop so it could be used for snow plowing and snow clearing the following day. The victim, who was going to move the bulldozer, climbed inside the cab of the bulldozer, which had been warming up for approximately one hour, and started moving it in the forward direction towards the blacksmith shop. At the same time a co-worker (A), was moving a front-end loader out of the blacksmith shop, and another co-worker (B) was located inside the blacksmith shop. Both co-workers witnessed the incident, although their views were partially obstructed.
Just prior to the incident, the victim exited the bulldozer cab. The co-workers did not know why nor did they know if he had stopped or slowed the bulldozer before climbing out. Once the victim was out of the cab and standing on the ground, it appeared that the bulldozer started to increase in speed. The victim attempted to reenter the cab but became caught on the bulldozer track, which appears that he tried to used as a “second” step to climb into the cab (Figure 2). The “first” step, which was provided by the bulldozer manufacture, was located under the top section of the bulldozer track (Figure 2). The victim was crushed when the bulldozer track rolled over him. The bulldozer then continued in the forward direction and struck the side of the blacksmith shop causing extensive damage to the building.
Co-worker A, who was moving the front-end loader, went to assist the victim while co-worker B, who was inside the blacksmith shop, placed a call for emergency assistance. According to the police report, co-worker B then exited the building, went over to the bulldozer and shifted it out of gear. Campus police and an ambulance arrived quickly and the victim was rushed to a local hospital where he was pronounced dead approximately six hours later.
One possible scenario is that the victim, while exiting the cab with the machine still in gear and the throttle lever in the idle position, unintentionally bumped the throttle lever (Figure 3) resulting in an increase in engine speed and subsequently motion of the bulldozer. Apparently, the victim attempted to regain control of the bulldozer by stepping on to the track, on which he became caught, to reenter the cab.
CAUSE OF DEATH
The medical examiner listed the cause of death as multiple traumatic injuries.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: State facilities should train all bulldozer operators on health and safety aspects of the equipment including proper steps to follow when stopping and exiting the bulldozer.
Discussion: This small, self sufficient facility had three bulldozers that were each used infrequently, less than ten times per year. The bulldozer involved in this incident had not been moved in the previous five weeks. Each bulldozer operator had a current operator’s license issued by the Massachusetts Department of Public Safety. To obtain this license an initial examination was required and the license was then automatically renewed every two years without any further requirements.
Equipment training should be provided for all heavy equipment operators, including on equipment that is used infrequently, in this case bulldozers. Annual heavy equipment training for bulldozer operators should include but not limited to the proper steps to follow when stopping and exiting the machine:
- Stop on level ground and reduce engine speed.
- Set the gearshift lever into neutral.
- Set the neutral lock lever, which will lock the transmission in neutral.
- Engage the brake pedals locking lever, which would lock the brakes on both tracks immobilizing the machine.
- Position the bulldozer blade and any other attachments in the full down position, which would also prohibit the bulldozer from moving.
In addition, the employer should always use the equipment operation manual when developing training for the operators. The operation manual will provide the manufacture’s operating procedures, which will include starting, stopping and using the equipment.
Recommendation #2: State facilities utilizing bulldozers should develop, implement and enforce a comprehensive health and safety program that includes but is not limited to procedures for entering, exiting and stopping bulldozers.
Discussion: This facility did not have a comprehensive health and safety program nor any single individual designated as responsible for health and safety. A comprehensive health and safety program should be developed with employee input. This should include but not be limited to a designated hierarchy of responsibility for the health and safety program, procedures for identifying and controlling hazards and training requirements. In addition, the health and safety program should include the development of a health and safety committee. The committee should include both management and workers and act as an avenue to bring these two groups together and discuss health and safety issues and concerns. A summary of OSHA’s draft proposed safety and health program rule has been included at the end of this report.
Given the wide array of tasks performed at this facility, development of a comprehensive health and safety program will be challenging. Development of the program should begin with employee input whereby employees provide lists of the tasks they perform, and identify the potential hazards associated with these tasks. Written procedures for tasks should be established as a combined effort of both management and the workers. All identified hazards should be ranked by severity and those identified as most dangerous to employee’s health and safety should be controlled first. A hazard control completion schedule should be developed for the remaining hazards.
Recommendation #3: States without state OSHA plans should explore options to ensure that state and municipal workers are provided with the same health and safety protection as their private sector counterparts.
Discussion: In Massachusetts, federal OSHA is responsible for enforcing health and safety standards in the private sector. The public sector is not subject to OSHA enforcement, thus state and municipal employers are not legally required to comply with OSHA standards in Massachusetts. OSHA regulation however, set important standards of practice for all employers, public as well as private.
Currently there are 23 states and jurisdictions operating complete state OSHA plans (covering both private sector and state and local government employees) and three that cover public employees only. Massachusetts has neither a state OSHA plan nor a state based occupational health and safety enforcement system for public sector workers. State, municipal, and county employees face similar hazards as their private sector counterparts and should be afforded the same protection.
Recommendation #4: Bulldozer manufacturers should consider equipment engineering design changes, such as developing a step to prevent the operator from stepping on the track while entering or exiting the bulldozer cab.
Discussion: In this case, the victim was trying to reenter the bulldozer operator’s area while the bulldozer was moving and the victim became caught on the rotating track. Bulldozer manufacturers should consider manufacturing all bulldozers, and retrofitting older models with two additional steps, one for each side of the bulldozer, that would cover a section of the track and flip up and out of the way when the bulldozer was in use. The step could be designed to cover a section of the track to prevent the operator from stepping directly on the track.
The step in the upright position could also act as a half-door and guard, providing the operator with increased protection while operating the bulldozer. In the event that the machine unexpectedly moves while the operator is entering or exiting the operator’s area, the possibility of the operator being exposed to and becoming caught on the moving track would be minimized. In addition, the flip step could have an interlock built into it so when the step is in the down position the interlock would disengage the bulldozer tracks.
REFERENCES
- Code of Federal Regulations, 29 CFR 1926.601 (b)(4) Motor vehicles, Government Printing Office
- ILO, Safety and Health in Construction: An ILO code of practice, Geneva, International Labor Office, 1992
- Code of Federal Regulations, 29 CFR 1926.602 (a)(1) and (d) Material handling equipment, Government Printing Office
- Fiatallis, Operation and Maintenance Instructions, FD7, Print No. 604.00.202 – English

Figure 1 – Bulldozer involved in the incident, inside the blacksmith shop
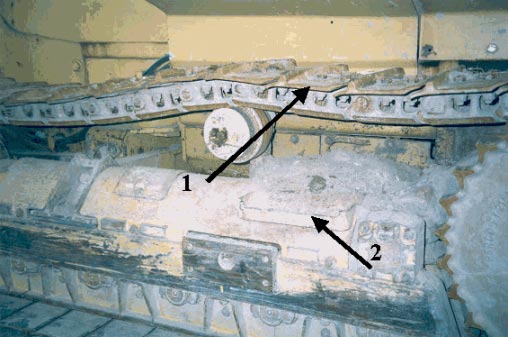
Figure 2 – Section of the bulldozer track
Arrow 1 – indicates bulldozer track section used as a step
Arrow 2 – indicates a step currently provided by the manufacture
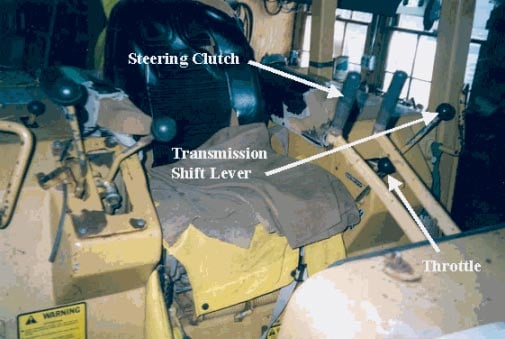
Figure 3 – Bulldozer operator’s seat and controls
|
SUMMARY OF OSHA’S DRAFT PROPOSED |
|
Core elements
Basic obligations
Employee participation
Identify and assess hazards to which employees are exposed
Investigate safety and health events in the workplace
|
Safety and health program record keeping
Hazard prevention and control
Information and training
Program evaluation and maintenance
Multi-employer workplaces
|
Date issued November 23, 1998. Full text available on https://www.osha.gov/dsg/topics/safetyhealth/nshp.htmlexternal icon. (Link updated 3/20/2013)
To contact Massachusetts State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.