
A Hispanic Ironworker Dies When He Falls 50 Feet Through a Floor Opening.
California Case Report: 07CA009
Summary
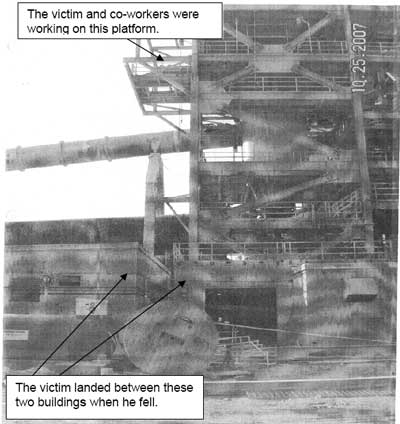
A 24 year-old Hispanic ironworker died after falling through a floor opening on a building platform. The victim and two co-workers were evaluating a job they were to undertake at a later date when the incident occurred. The platform on which they were standing was approximately 50 feet above the ground. The hole through which the victim fell had a cover, but it was not secured in place. The cover did not have any marking on it to indicate what it was being used for. The victim was wearing fall protective equipment but was not tied off. The CA/FACE investigator determined that, in order to prevent future occurrences, employers, as part of their Injury and Illness Prevention Program (IIPP) should:
- Ensure that proper procedures are followed when employees are working around elevated floor openings.
Introduction
On October 25, 2007, at approximately 1:45 p.m., a 24-year-old Hispanic ironworker died when he fell approximately 50 feet through a floor opening on a building platform. The CA/FACE investigator learned of this incident on November 5, 2007, from the Cal/OSHA Bureau of Investigation. The CA/FACE investigator made contact with the company for whom the victim worked on November 12, 2007. On February 5, 2008, the CA/FACE investigator visited the incident site and interviewed company management representatives. However, the victim’s co-workers could not be interviewed as they were no longer employed by the company and no contact number was available.
The employer of the victim was a construction company that had been in business for 84 years and employed over 14,000 employees. Approximately 700 employees were at the site where the incident occurred. The victim had worked at this location for five months. He was born in Mexico and had been in the United States for less than one year. He had an eighth grade education and spoke only Spanish. It is not known how long the victim had worked as an ironworker.
The employer had a safety program which included an IIPP that met Cal/OSHA and the Mine Safety and Health Administration (MSHA) requirements. The safety supervisors were bilingual and conducted the safety meetings in Spanish, which were held weekly and documented. The employer also had a documented bilingual training program that instructed their employees in all the safety requirements needed for their jobs. There were bilingual written task specific safe work procedures for the tasks performed at the construction site. The victim had received specific training in fall protection.
Investigation
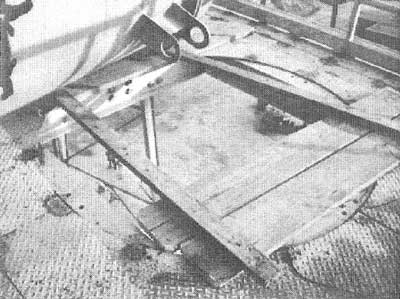
The site of the incident was a cement plant under construction. On the day of the incident, the victim, along with two other workers, climbed stairs to a balcony that was an extension of one of the cement plant floors. The balcony was approximately 50 feet above the ground. The employees were to determine what tools and equipment would be needed to assist in the installation of a tank that had been temporarily placed on the balcony. In the center of the balcony was a 48-inch diameter opening that was to accommodate an air duct to be installed at a later date. The opening had a cover consisting of six scaffold planks held together with 2 x 4’s nailed at each end. It is not known if the cover was in place over the hole at the time of the workers’ arrival. There were no signs or placards to alert workers about the hazard of removing the hole cover. A photograph obtained during the MSHA investigation showed that the cover had been partially disassembled and removed. The supervisor stated the co-workers told him that the cover had been removed prior to beginning their work, while a written safety checklist completed earlier that morning indicated that the cover was in place. At some point in the evaluation process, the victim, who was wearing fall protection equipment but was not tied off, fell through the floor opening approximately 50 feet to the ground below. The paramedics were called and arrived to find the victim lying on the ground. They performed emergency procedures on the victim and transported him to a local hospital where he was pronounced dead.
Cause of Death
The cause of death, according to the death certificate, was multiple blunt force trauma.
Recommendations/Discussion
Recommendation #1: Ensure that proper procedures are followed when employees are working around elevated floor openings.
Discussion: When employees work around an elevated floor opening, proper procedures must be followed in order to provide a safe and healthy work environment. The floor opening must be covered to prevent workers from falling through it. The covers should be capable of safely supporting whichever is greatest: 400 pounds, or twice the weight of the employees, equipment, and materials that may be imposed on any one square foot area. The cover must be secured in place to prevent accidental removal or displacement. Additionally, it should be clearly marked with letters not less than one inch high and in a language the workers can understand, stating: “Opening–Do Not Remove.” In this case, the hole was covered but not marked, and the evidence suggests that the victim and co-workers either removed the cover of the opening in order to accomplish their task, or the cover had already been removed prior to their entering the balcony. In either case, personal fall protection equipment should be used properly to prevent falls through unguarded floor openings. The victim and co-workers had safety harnesses on with lanyards but they did not tie off when they were working around the floor opening. Employers can enhance worker compliance with safe work practices through programs of task specific training, supervision, recognition, and progressive disciplinary measures.
Reference
- California Code of Regulations, Subchapter 7. General Industry Safety Orders, Group 1. General Physical Conditions and Structures Article 2. Standard Specifications. §3212. Floor Openings, Floor Holes and Roofs.
Exhibits
|
|
Exhibit 1. The structure involved in the incident. |
 |
|
Exhibit 2. View looking up at the floor opening on the |
 |
|
Exhibit 3. View looking down through the opening in the platform.
|
California Fatality Assessment and Control Evaluation (FACE) Project
The California Department of Public Health, in cooperation with the Public Health Institute and the National Institute for Occupational Safety and Health (NIOSH), conducts investigations of work-related fatalities. The goal of the CA/FACE program is to prevent fatal work injuries. CA/FACE aims to achieve this goal by studying the work environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact. NIOSH-funded, State-based FACE programs include: California, Iowa, Kentucky, Massachusetts, Michigan, New Jersey, New York, Oregon, and Washington.
To contact California State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site. Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.