
Pipefitter dies from 40-foot fall
Alaska FACE Investigation 98AK027
SUMMARY
A 32-year-old journeyman pipefitter was killed when he fell 40 feet from a metal roof. The pipefitter (the victim) had climbed onto the roof to direct the placement of a tool case on top of a scaffold platform. The victim was wearing a body harness with an attached lanyard but was not secured to a lifeline or the scaffold. The lift operation required a mobile crane to lift the case from one side of the building, over the roof, to the opposite side. The victim was using a two-way radio to communicate instructions to the crane operator. While the case was being lowered to the crew on the scaffold, the victim lost radio contact with the crane operator. He walked to the peak of the roof to see if he could give visual signals to the operator. As he neared the peak, the victim slipped or tripped, fell over the peak, and slid down the opposite side. The victim fell 40 feet to the ground. Co-workers immediately called for emergency assistance. The victim was transported to the site’s medical facility where he died a short time later.
Based on the findings of the investigation, to prevent similar occurrences, employers should:
- Ensure that workers adhere to existing standards and procedures for the use of personal fall restraint equipment and ensure that equipment meets all safety standards before it is placed in use.
- Ensure that workers are able to recognize and avoid hazardous situations and be able to effectively warn others of potential hazards.
- Routinely conduct scheduled and unscheduled worksite safety inspections.
INTRODUCTION
At 11:05 AM on September 22, 1998, a 32-year-old male journeyman pipefitter (the victim) fell 40 feet from a roof and later died from his injuries. On the same day, the owner/operator of the worksite and the Alaska Department of Labor (AK-DOL) notified the Alaska Division of Public Health, Section of Epidemiology. An investigation involving an Injury Prevention Specialist for the Alaska Department of Health and Social Services, Section of Epidemiology ensued on September 23, 1998. The incident was reviewed with AK-DOL officials. Alaska State Troopers, Medical Examiner, and AK-DOL reports were requested.
The company involved in the incident was privately owned and had been in business since 1968. The company provided construction, fabrication, and installation services and employed about 250 workers in Alaska; 30 were assigned to the incident location. At the time of the incident, the victim and two co-workers (a journeyman pipefitter and a welder) were working on a scaffold to repair a gas recycle line. The victim was the lead man for the three-man repair crew. The company involved was working under contract to the worksite owner (the client company).
The company had a written safety program that detailed specific work practices and employee conduct at the worksite. A job safety analysis (JSA) was also completed for each task. All employees attended an orientation to the company’s safety program upon initial hire. On-the-job safety training usually addressed personal protective equipment, hazard identification, work practices, machinery and equipment use, and hazard communication. Since the company normally contracted their services to a general contractor or client company, employees were also required to attend all safety training classes conducted by or on behalf of a general contractor or client company. The individual crews also conducted daily toolbox safety meetings and daily and weekly walk-thru site inspections. This was the first fatality experienced by the company.
Many projects at the incident location required the use of specialty tradespersons supplied by various contractors. As required by the client company, the individual contractors had comprehensive safety plans and designated personnel to implement and supervise their respective safety and health programs. When projects required multiple contractors to work concurrently, the safety management teams would sometimes agree to work cooperatively to minimize duplication of tasks.
INVESTIGATION
The company had been contracted to repair a section of pipe used as a gas recycle line. The task was initially assigned to another contractor. However, due to the workload and the limited amount of time left for completion of the project, a second contractor (the company) was also hired, working concurrently with the first contractor. The pipe repair crew involved in the incident consisted of a crane operator, a welder, and two journeyman pipefitters; all had extensive experience at the worksite. The pipe to be repaired was located in a pipe saddle approximately 40 feet above ground behind a building. A scaffold was erected under the section of pipe to be repaired.
Weather on the day of the incident was overcast. Temperatures varied from 30° F at 8:00 AM to 34° F at 12:00 PM. Winds were 4 to 12 MPH, producing potential wind chill temperatures of 13 to 18° F. During the morning tool box safety meeting, workers were cautioned to be observant of slick and ice-covered work surfaces and to follow all safety guidelines when climbing to, working on, and descending from elevated work stations. Client company guidelines mandated the use of personal fall arrest system when working on unguarded surfaces that were 6 feet or more above the next lower level.
Following the morning toolbox meeting, the individual crews went to their assigned work areas. A crew working on the roof of another building encountered icy conditions. As the crew walked across the roof surface, one worker slipped, slid a short distance down the roof surface, but was restrained from sliding off the roof by his personal fall arrest system. The incident was immediately reported to the foreman who cancelled their assignment until conditions improved. This information was not conveyed to the other crews since all were cautioned about icy working surfaces during the toolbox meeting. The roof was checked later that morning and found to be dry.
The building involved in the incident was 42 feet wide, 24 feet long, and 32 feet tall. The building was set on top of 8-foot pilings. The roof had a 4½ x 12 pitch. Total height from the roof to the ground was 40 feet at the edge and nearly 45 feet at the peak. Exterior surfaces including the roof were covered with overlapping metal sheets that were bolted in place. The 5/8 inch bolt heads were not flush with the metal surface and extended approximately ¼ to 3/8 inch above the surface (Figures 1 and 2).
Two of the three scaffolds used by the repair crew were erected near the edge of the building’s metal roof and under the sections of pipe (Figure 3). The scaffold platforms were 38 feet above ground. Landing platforms were not installed on the scaffold ladder. Workers wore body harnesses with attached lanyards but did not use any other ladder safety devices that incorporated a friction brake and sliding attachment (ascenders) for climbing to and descending from the scaffold platform. In order to accommodate the pipe, several handrails and mid-rails were not in place. Both scaffolds were tagged “incomplete” and required all workers to use personal fall protection equipment (100% tie-off) whenever on the scaffolds. The scaffolds were inspected and signed-off daily by the erector; site surveys were also completed by the foreman.

Figure 1. View of building and surrounding structures.
Caption: The scaffold was located on the opposite side of the building.
The lower section of the building that includes the 8-foot pilings is not in view.
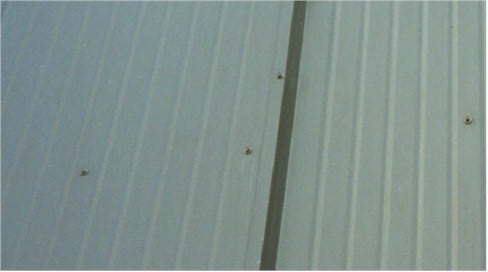
Figure 2. Close-up view of metal sheets covering the building exterior.
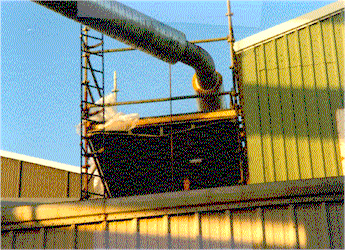
Figure 3. Scaffold under section of pipe to be repaired.
Caption: This is not the scaffold involved in the incident, however it is similar in construction and location.
The view of the scaffold is partially blocked (foreground) by another building.
The difference in height between the scaffold platform and the roof edge is approximately 2 feet.
On the morning of the incident, the repair crew climbed onto one of the scaffold platforms and completed the initial cut for the pipe weld repair. The next phase of the repair required the use of a tri-tool to bevel the pipe edge for the weld. The tri-tool, which weighed approximately 100 pounds, was stored in a hard plastic case. Due to the configuration of pipes and structures around the building, a mobile crane was positioned in front of the building (opposite the pipe repair) to lift the case to the repair crew. Prior to lifting the tri-tool, the crew descended the scaffold for their morning break. During this time, the crane operator and the foreman checked the crane’s boom extension and angle to make sure it could reach the scaffold and remain clear of the roof peak.
After the morning break, the repair crew again climbed to the scaffold platform to await the tri-tool. “Blind” lifts were not uncommon, and since the crane operator would not be able to see the scaffold, the victim and the crane operator used hand-held two-way radios to communicate. The radios were checked by the foreman and the victim and then again by the victim and the crane operator. Radios were functioning properly during both communication checks. Each member of the repair crew was wearing a body harness and lanyard. Except for the victim, the repair crew removed their harnesses after climbing onto the platform. The crewmembers stated that the harnesses were too restrictive especially during welding procedures.
The victim left the scaffold and climbed onto the roof to direct the lift. The surface conditions of the roof were not known, however witnesses reported relatively dry conditions on the lower section of the roof and scaffold. Since the crew was assigned to work on the scaffold, a lifeline was not secured to the roof. Although the victim was still wearing his harness and lanyard, he was not tied-off to the scaffold. The crewmembers later said the victim stated he wanted a better view of the boom to assure it did not contact the roof. They assumed that if the victim were to fall, he would slide back onto the scaffold platform: the metal roof panels would keep him aligned with the scaffold. They therefore did not question the victim’s actions.
The lift began without complication. As the tri-tool case neared the scaffold, the victim instructed the crane operator to stop. The case was suspended approximately 10 feet in the air above the scaffold. The victim instructed the crane operator to move left. When the operator did not respond, the victim repeated his instruction and then attempted to check the radio function by adjusting the controls. At 11:05 AM, the crewmembers observed the victim climbing the roof. They assumed that the victim was going to attempt to visually signal the crane operator from the peak. As the victim neared the peak, one crewmember (the witness) saw him pitch forward and fall over the peak. The witness could not tell if the victim lost his footing due to a slip or if the victim tripped, possibly on a bolt head. The victim appeared to try to twist around to grab the roof cap and then slid down the opposite side of the roof, falling 40 feet from the roof edge to the ground (Figure 4).
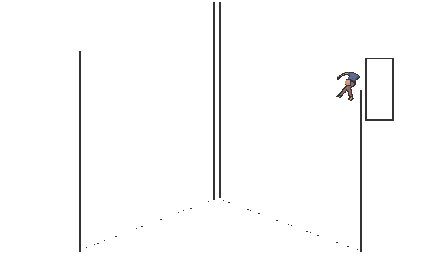
Figure 4. Diagram of roof and scaffold (not to scale)
The victim was found on the ground by co-workers immediately following the incident. One co-worker ran to a nearby office to call for emergency assistance while others assisted the victim. Emergency medical staff arrived at the site minutes later at 11:12 AM. Examination of the victim indicated extensive fall injuries. The victim was transported to a nearby medical facility at 11:42. Upon arrival to the facility, the victim exhibited no respiration or pulse; CPR was initiated. The medical staff consulted with an Anchorage-based emergency room physician; the victim was pronounced dead at 12:25 PM.
CAUSE OF DEATH
The medical examiner’s report listed the cause of death as impact injuries to the chest from a 40-foot fall.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that workers comply with existing standards and procedures for the use of personal fall restraint equipment and ensure that equipment meets all safety standards before it is placed in use.
Discussion: In this incident, complacency severely diminished worksite safety. The scaffold was incomplete and tagged to alert workers that personal fall arrest equipment must be used at all times. Although the repair crew wore personal fall arrest equipment, two of them removed their harnesses to work more easily around the pipe. In addition, since an appropriate safety system was not in place, no one was authorized to leave the scaffold. Crewmembers were either not aware of, not observant of, or did not thoroughly comprehend the standards and procedures that affected their use of scaffolds. While workers may become accustomed to working on elevated surfaces or platforms, they must still remain aware of the dangers in their immediate surroundings and comply with existing safety guidelines. Whenever workers are not capable of complying with existing safety standards and procedures or if personal protective equipment is too restrictive or cumbersome to proceed safely with the task—1) the job should be immediately stopped and 2) alternative methods should be discussed and requested.
Employers should ensure that scaffolds meet all safety standards prior to their use. The scaffold in this incident was compromised. Ascenders and landing platforms on the fixed ladder should have been in place to reduce the risk to workers climbing to and descending from the work platform (29 CFR 1910.27(d)).
Recommendation #2: Employers should ensure that workers are able to recognize and avoid hazardous situations and be able to effectively warn others of potential hazards.
Discussion: In this incident, the victim left the scaffold and climbed onto the metal roof. Due to the close proximity of the scaffold platform to the roof edge, the victim and his co-workers did not recognize the hazards associated with his actions. Employees should be aware of their work environments. Where there is a potential for a fall, they should receive specific and adequate training to recognize potential fall hazards. This training should always include:
- Information on hazard communications, how it is documented, and where to look for it before initiating a task.
- Instruction on the appropriate use of equipment to control or abate a fall hazard.
Recommendation #3: Employers should routinely conduct scheduled and unscheduled worksite safety inspections.
Discussion: Employers should emphasize safety to their employees by enforcing a comprehensive safety program. The safety program should include unscheduled worksite safety inspections to evaluate compliance with and understanding of established safety standards. While employees have the right to question the safety of any task, they are responsible for following the practices outlined in their employer’s safety program. The primary responsibility for an individual’s safety is always their own.
References
National Safety Council. Accident Prevention Manual for Business & Industry: Administration & Programs. 10th Ed. Chicago, IL; 1992.
Office of the Federal Register: Code of Federal Regulations, Labor 29 Part 1910. Washington, DC: U.S. Government Printing Office, 1996.
Fatality Assessment and Control Evaluation (FACE) Project
The Alaska Division of Public Health, Section of Epidemiology performs Fatality Assessment and Control Evaluation (FACE) investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR). The goal of these evaluations is to prevent fatal work injuries in the future by studying the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact.
To contact Alaska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.