
Laborer Dies from Crush Injuries When He was Struck-by a Suspended Overhaul Ball
FACE 97-AK-033
SUMMARY
A 29-year-old male laborer was killed when a suspended 350-pound overhaul ball was severed from a cable on a mobile crane and struck his head. The victim was a sheet metal worker/welder at a remote construction site. During off-duty hours, he had acquired additional employment with a second construction company as a temporary laborer to assist in the relocation of several trailers. The mobile crane in the incident was equipped with two hoists. Each hoist was attached to a lift assembly, either a hook block (on the main hoist assemblage) or an overhaul ball (on the auxiliary hoist assemblage). After repositioning the crane to lift the next trailer, the crane operator rotated the boom and lowered the hook block so the victim could attach the rigging. Seeing the block was approximately a half-foot short of position, the operator (the witness) extended the boom to adjust the block position. During this procedure, the overhaul ball came into contact with the boom nose and the cable severed. The victim was struck on the head by the ball. After checking the victim, the operator immediately drove to the main road for help. Emergency service units were summoned to the site. The victim was transported to the medical clinic where he was pronounced dead by the attending nurse practitioner.
Based on the findings of the investigation, to prevent similar occurrences, employers should:
- ensure all employees are capable of recognizing worksite hazards and their avoidance;
- ensure the use of written, pre-start inspection checklists and incorporate all retrofit safety devices and aids into the checklist;
- ensure equipment operators follow manufacturer guidelines for the safe operation of equipment;
- ensure the completion of all periodic equipment inspections by a qualified person and communicate recommendations and findings to the equipment operators.
INTRODUCTION
At approximately 9:45AM on September 20, 1997, a 29 year-old-male laborer (the victim) was killed after being struck by the overhaul ball of a mobile crane. The overhaul ball is commonly referred to in the industry as a “headache ball.” Upon reporting of the incident in the media, the Alaska Division of Public Health, Section of Epidemiology contacted the Alaska Department of Labor (AKDOL) on September 24, 1997. An investigation involving an injury prevention specialist for the Alaska Department of Health and Social Services, Section of Epidemiology ensued on September 30, 1997. The injury prevention specialist traveled to the incident site and reviewed the incident with company representatives and the AKDOL investigator. Photographs of the incident site were obtained during the investigation. Alaska State Troopers and Medical Examiner reports, as well as AKDOL reports, were requested.
The construction company in this incident was composed of two privately owned companies which conducted joint ventures in Alaska since 1972. At the time of the incident, the operation was in the process of demobilizing (removing from service) its camp from a construction site. The operation employed a five-man crew to complete the demobilization — the victim was a crew member as a temporary laborer. He had worked for approximately 3 hours prior to the incident. The victim was also employed full-time as a sheet metal worker/welder for another company at the same location.
The joint venture had a written safety program/manual. Prior to beginning assigned duties, employees attended a worksite meeting. This was conducted by the site supervisor and included discussion of safety issues pertaining to the pre-lift, lift, and relocation process. This was the first fatality experienced by the joint venture of the two companies.
INVESTIGATION
The incident occurred at a construction/renovation project site located in a remote Alaska community. The project site included several large lots used for storage, primarily heavy equipment, supplies, and various types of portable units including trailers and liquid storage tanks. These lots were in a flat, open area, approximately 0.2 mile from a main transportation road traversing the project site. The joint venture camp was located in one of these lots. The lot surface was level and consisted of compacted soil and crushed rock. At the time of the incident, weather was not considered a contributing factor.
Demobilization involved relocating several large portable housing/office units, tractor-trailers, and other heavy equipment to a dock for loading and shipment. The process of relocating the portable units entailed the use of a crane to lift each unit onto a low bed trailer. The units were then transported to the dock for placement on a barge. The crane used at the incident site was a 1973 mobile hydraulic crane with a telescoping boom (Figure 1) the boom mounted to the right of the operator’s compartment. The crane was equipped with two hoist assemblages: a main and an auxiliary (whipline). Both hoist assemblages consisted of a hoist (a hydraulic operating drum), a cable, and hook block (a block with an attached hook for lifting loads with the main hoist) or overhaul ball (a heavy ball required to unwind cable from the hoist drum) with an attached hook. Sheaves (wheels or disks with a grooved rim) guided cables over the boom nose. In this incident, the main hoist assemblage was being used to lift the trailers, however the whipline was in place and functional. The crane’s certificate of inspection for lifting equipment was posted inside the cab and had expired in 1994. The crane had not been used in the 3-year interim.
On the day of the incident, the crew arrived at the lot to discuss the procedure of lifting, loading, and transport of the trailers. The victim and the crane operator (the witness) remained at the lot to coordinate pre-lift, lift, and loading activities, while the other three crew members transported the trailers to or worked at the dock. The crane operator had 20 years experience in crane operation including approximately 6 months with mobile hydraulic cranes. Prior to beginning lifting, the operator had completed a “walkaround” visual inspection of the crane. A written inspection worksheet was not used at that time. Anti-two-blocking devices were installed on the crane, however they were not required for operation of this particular unit and had not been inspected during the walkaround. During inspection after the incident, the devices were found to be missing parts and not capable of functioning as designed.
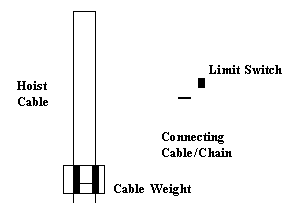
“Two-blocking” is a term used to describe contact between the hook block (or overhaul ball) and the boom nose. Two-blocking will occur if the hook block or overhaul ball is pulled into the boom nose by the operating hoist. Alternatively, two-blocking can be caused by either extending the boom or lowering the boom if the hook block or overhaul ball is already close to the boom nose and cable is not simultaneously let out. An anti-two-blocking device is an “operational aid” to help prevent contact between these components. The devices on this unit were closed circuit sensors consisting of weights and limit switches. Typically, the devices consist of weights fastened around each cable below the boom nose and suspended from the limit switch by a cable or chain. While the weight remained suspended, allowing the cable to pass freely through the weight, it maintained a closed circuit (Figure 2). The circuit opened when the block or ball rose to a position to support the weight, activating an audible alarm and warning light. Crane actions of hoist up, boom extension, and boom lowering are also halted. A bypass switch enabled the operator to override the automatic shutoff.
Prior to the incident the victim and the crane operator had completed lifting and loading one trailer and had disconnected the rigging from the hook block. The crane was repositioned for lifting the next trailer. Outriggers were extended and the crane was checked to be level. The rigging, a four-point cable assembly attached to a spreader bar, remained on the ground and would later be attached to the hook block in order to lift and suspend the unit properly. The boom was raised to an approximate 40 degree angle. The boom nose was approximately 30 feet from the ground (Figure 3). The hook block was positioned several inches from the ground and approximately 6 inches short of the “O” ring connecting the four-point cable assembly of the spreader bar. It was surmised the overhaul ball was near or in contact with the boom nose at this time. The operator extended the boom to correct the hook block position. As the hook block position was adjusted, the boom simultaneously extended under the stationary auxiliary hoist cable. The overhaul ball and cable were pulled towards the boom nose, contacting the whipline sheave (Figure 4). The cable was severed just above the cable connector for the overhaul ball.
As the operator was making the final boom adjustment as described, the victim walked toward the rigging inside the spreader bar to grasp the “O” ring of the cable assembly. The victim was returning to an upright position when the cable severed. The ball struck the top left-side of the victim’s hard hat. The operator witnessed the victim’s immediate collapse and ran over to check for a pulse. Finding no pulse, he drove to the main road to flag a vehicle with a two-way radio. Time needed for this action was unclear, but it was estimated to be minutes. The emergency medical service team was notified at 9:46 AM. At 9:50 AM, emergency medical technicians arrived at the incident location and started CPR. The victim was transported by ambulance to the facility health clinic at 9:56 AM where he was pronounced dead.
CAUSE OF DEATH
The certifier’s form from the Office of the State Medical Examiner listed the cause of death as massive craniocerebral disruption.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure all employees are capable of recognizing worksite hazards and their avoidance.
Discussion: 29 CFR 1926.550(a)(19) states “All employees shall be kept clear of loads about to be lifted and of suspended loads.” In this incident, the victim approached the crane and lift assembly prior to the completion of the boom adjustment by the crane operator. While the victim may have been aware of the dangers associated with suspended loads, he apparently did not recognize the potential hazard of the lift assemblies. Employers should ensure workers are capable of recognizing the potential hazard of all suspended materials, including any rigging such as spreader bars, overhaul (headache) balls, and hook blocks, and maintain a safe distance and orientation to avoid their hazard.
Recommendation #2: Employers should ensure the use of written, pre-start inspection checklist and incorporate all retrofit safety devices and aids into the checklist.
Discussion: In this incident, an inspection worksheet was not used during the pre-start inspection of the crane. The checklist provides an effective means to ensure all manufacturer’s suggested items have been inspected to identify deficiencies for the safe operation of the equipment. While the crane was not required to have anti-two-blocking devices, it had been retrofitted with these devices as a safety aid for the operator. Physical inspection and function checks of these safety aids and all other retrofit devices should be included as additional checklist items. Any defects should be noted in the equipment maintenance log and be repaired or replaced, if necessary, prior to initial start-up and use of the equipment.
Recommendation #3: Employers should ensure equipment operators follow industry guidelines for the safe operation of equipment.
Discussion: In this incident, the overhaul ball was close to the boom nose prior to the extension of the boom. As the boom is either lowered or extended, the boom nose will move closer to the hook block and overhaul ball. In the absence of functional anti-two-blocking devices, the proximity of the block or ball to the boom nose becomes critical. In accordance with accepted industry practices for safe operation of cranes, both the main and auxiliary cables should be simultaneously let out when extending (or lowering) the boom to prevent two-blocking the boom nose with the hook block or overhaul ball. Employers should ensure equipment operators follow all manufacturer guidelines for the safe operation of equipment.
Recommendation #4: Employers should ensure the completion of all periodic equipment inspections by a qualified person and communicate recommendations and findings to the equipment operators.
Discussion: In this incident, the mobile crane had previously been certified in 1993. However, it had remained inactive without periodic inspection for the 3 years following the (1994) expiration of the certificate. 29 CFR 1926.550(a)(6) states AA thorough, annual inspection of the hoist machinery shall be made by a competent person, or by a government or private agency recognized by the U.S. Department of Labor.@ Employers should ensure lifting equipment is inspected by a competent person or agency and all defects are recorded, evaluated for safety hazard, and communicated to the equipment operator prior to placing the equipment in service.
REFERENCES
American National Standard, Safety Standard for Mobile and Locomotive Cranes, ANSI/ASME B30.5. New York, New York: American Society of Mechanical Engineers, 1982.
Office of the Federal Register: Code of Federal Regulations, Labor 29 Part 1926. Washington, DC: U.S. Government Printing Office, 1996.
Fatality Assessment and Control Evaluation (FACE) Project The Alaska Division of Public Health, Section of Epidemiology performs Fatality Assessment and Control Evaluation (FACE) investigations through a cooperative agreement with the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR). The goal of these evaluations is to prevent fatal work injuries in the future by studying the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact.
To contact Alaska State FACE program personnel regarding State-based FACE reports, please use information listed on the Contact Sheet on the NIOSH FACE web site Please contact In-house FACE program personnel regarding In-house FACE reports and to gain assistance when State-FACE program personnel cannot be reached.
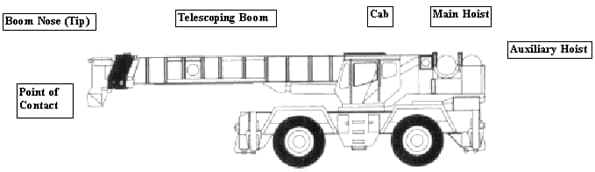
Figure 1. Mobile Hydraulic Crane – Side View
|

|
|
Figure 2. Anti-Two-Blocking Device |
Figure 3. Height and Angle of Boom |

Figure 4. Whipline Sheave and Anti-Two-Blocking Device