
Manufacturing Traffic Supervisor Dies When Struck By Forklift
Michigan Case Report: 08MI010
Summary
|
|
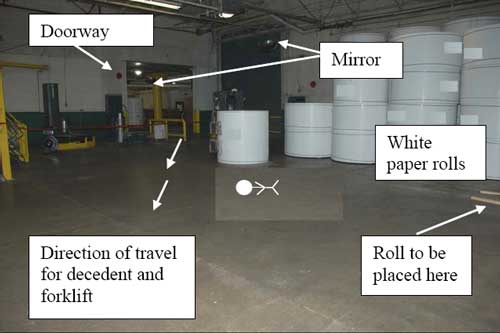
Figure 1. Incident scene showing entrance to storage area, path of forklift travel, final position of decedent, overhead mirrors |
On March 3, 2008, a 59-year-old male traffic supervisor, who was wearing a white hard hat, died when he was struck by a Yale clamp truck that was transporting a paper roll that was approximately 59 inches tall and 50 inches wide. The decedent, who was not using the designated pedestrian aisleway, was walking through the forklift travel area of the paper roll storage warehouse on his way to the shipping and receiving offices. The driver, who had entered the roll storage area through the doorway, was traveling in a forward direction (not trailing the load). He intended to place the roll in its appropriate place on 2- by 4-inch pieces of wood. The clamp truck/paper roll struck the decedent. The driver looked to his right on the ground and could see the decedent’s body to the right of the truck’s right tire. He immediately backed up and called for emergency assistance. Emergency response arrived. The decedent was declared dead at the scene.
Recommendations:
- The employer should revise its forklift safety rule regarding driving the forklift in the direction that affords the “best visibility” to clarify and require the operator to trail a load when a driver’s forward vision is obscured.
- Employers should continually stress the importance of adherence to established safe work procedures.
- The company should review the locations of the designated pedestrian aisleways to determine if they are appropriately located for pedestrian travel.
- The company should consider using a highly visible hard hat color (such as yellow or orange) and when job appropriate, the use of reflective vests for pedestrians.
Introduction
On March 3, 2008, a 59-year-old male traffic supervisor died when he was struck by a Yale clamp truck transporting a paper roll. On the same day, MIOSHA General Industry Safety and Health division personnel notified MIFACE that the above incident had occurred. On April 30, 2008, the MIFACE researcher interviewed the firm’s safety director. After the interview, the safety director escorted the MIFACE researcher to the location of the incident and noted the building modifications that had been installed after the incident. MIFACE reviewed the autopsy results, death certificate, police report and pictures, MIOSHA file and citations, and the firm’s written safety program provided by the firm’s safety director. The pictures used in Figures 1 and 4 are courtesy of the responding police department. Pictures used in Figures 2 and 3 were taken at the time of the MIFACE site visit. Figure 5 is courtesy of the MIOSHA compliance officer.
The employer for whom the decedent worked was a paperboard manufacturer, supplying food product manufacturers. Approximately 200 people who worked for the company at the time of the incident. The decedent had worked at the company for 38 years, 20 of which were in his current position, traffic manager. He was a full-time employee. His work shift was 4:00 a.m. to 12:00 p.m. He arrived at work on the day of the incident at approximately 3:30 a.m.
The firm employed a full time safety director who had nine years of safety management experience. The safety director had worked six months as an hourly employee at this facility as well as both an hourly employee and supervisor at an automotive plant. The safety director, who was responsible for administering the company’s safety program, reported directly to the company’s general manager. The safety person was not present onsite at the time of the incident.
The MIOSHA compliance officer determined that the firm’s written safety program had been partially implemented at the time of the incident. The safety program had specific safety rules for pedestrian safety and lift truck operation. The Lift Truck Safety section in the safety program stated that the forklift driver should “always drive in the direction that affords the best visibility.” The Pedestrian Safety section stated, “The use of pedestrian aisles is mandatory where provided and must be explained and reviewed with all employees, contractors, and visitors as part of our mill orientation before they are permitted in the mill.” Additionally, the Pedestrian Safety section included, “Employees must not, as a matter of convenience, take shortcuts between stacked materials, equipment, or through a warehouse area outside of designated aisles.” Both of these sections noted that the pedestrian and lift truck driver shall make eye contact with each other to ensure safe travel. Safety responsibilities were delegated to supervisors, who had received appropriate training.
The firm had a joint management/labor health and safety committee, which met on a monthly basis. A written disciplinary procedure was in place. The safety committee was comprised teams that addressed specific problems and issues. For example, there was a lockout team that assessed equipment and procedures, a team that addressed building issues, and a safety work order team.
Supervisors held 5-minute safety talks with employees on a weekly basis. On a quarterly basis, the safety director held safety meetings with all employees. The firm had a safety training program that included classroom and on-the-job training. New employees had a 3-day safety orientation. Employee training was documented. At the time of the incident, the decedent was wearing the company mandated hearing protection, eye protection, steel-toed boots, and a hard hat. The firm’s hard hats were white.
The forklift driver had a previous forklift crash; he had been driving too fast and had struck a pole. He sustained head injuries in that incident. He told police who had interviewed him at the time of this incident that he had been more careful.
Company Remediation
After the incident, the company rigorously enforced its disciplinary policy when a driver was observed driving with the load in front when the load obstructed the driver’s vision.
Figures 2 and 3 show the structural modifications made to the incident scene area after the incident. The company installed an overhead hanging STOP sign at the entrance to the roll storage room, and added pedestrian protections, including marked a pedestrian aisle way in the main corridor, gates with posted STOP signs at the entrance to forklift travel areas, and a chain that must be removed by the forklift operator before entering the roll storage area.
 |
|
Figure 2. Building modifications made after incident, looking from supervisor’s office toward roll storage warehouse |

|
|
Figure 3. Building modifications looking from roll storage warehouse towards supervisor’s office |
MIOSHA General Industry Safety and Health Division issued the following Serious citations at the conclusion of its investigation:
SERIOUS:
POWERED INDUSTRIAL TRUCKS, PART 21, RULE 2185.
A powered industrial truck was driven when the operator could not look in the direction of and/or keep a clear view of the direction of travel.
Firm not enforcing that operators trail loads when view is obstructed, Yale Clamp Truck.
SERIOUS:
POWERED INDUSTRIAL TRUCKS, PART 21, RULE 2152(1)(e). An employer shall provide training to the employee before the employee’s assignment as an operator of a powered industrial truck. Instruction shall include state safety standard rules 2171 to 2193 of Part 21 “Powered Industrial Trucks,” being R 408.12171 to R 408.12193 of the Michigan Administrative Code.
Inadequate training, not adequately trained on which loads being moved need to be trailed, Yale Clamp Truck.
Investigation
A 7,700 pound capacity Yale clamp truck with a 7,500 pound capacity clamp attachment was involved in the incident. The truck had a functioning horn and head-lights mounted just under the overhead guard. The headlights turned on when the truck was started. After the incident, no mechanical issue was found concerning the truck. The truck with clamp attachment was transporting a 59 1/2 inch tall by approximately 50-inch wide paper roll weighing 4,847 pounds from one area of the plant to a roll storage area. Forklifts were required to be checked each day. If all control and operational checks were satisfactory, the driver did not need to check anything on the forklift checklist form. The checklist was marked only if the forklift needed maintenance.

|
|
Figure 4. Yale clamp truck with paper roll involved in incident |
The decedent, who was the traffic supervisor, was in charge of shipping and receiving, scheduling trucks and the truck loading/unloading in the dock area. The decedent was also responsible for training employees on forklift operation and conducting forklift testing. The decedent had come to work early the day of the incident so he could meet with the third shift supervisors to determine staffing needs for the first shift. After the staffing discussion that was held in the supervisor’s office, the decedent walked from the supervisor’s office through the roll storage warehouse area to the shipping and receiving office.
In the Roll Storage Warehouse, there was a non-operational machine located to the wall side of the entrance, an open area about 25 feet wide, and paper roll storage on the far side of the entrance. Pedestrian walkways were designated around the perimeter of the roll storage area. The doorway to the roll storage warehouse was approximately 12 feet wide and was approximately 40 to 50 feet from the roll storage. The floor from the doorway into the warehouse had approximately a 4-degree slope towards the roll storage for about 10-15 feet. An overhead mirror was present at the doorway. Also present was an additional overhead mirror hanging from the ceiling in the roll storage area.
 |
|
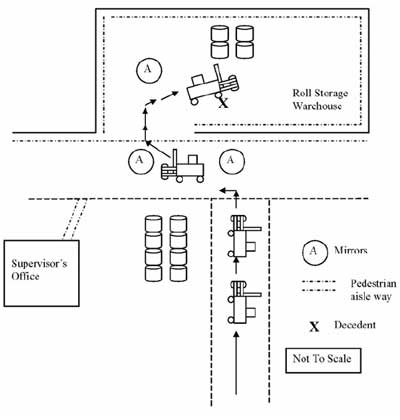
Drawing 1. Overview of incident scene showing
Yale clamp truck travel path |
The third shift forklift drivers had not kept pace with machine operations and were behind in transporting the rolls to the roll storage warehouse. The forklift operator, who was 6 feet 6 inches tall, had been driving clamp trucks for 10 years. He began his work shift at 11:00 p.m. He picked up a roll of paper in the roll staging area, backed up and rotated the roll so that roll was vertical, (i.e., the ends of the roll were facing up and down). The driver then drove forward down an aisle, turned left at the main aisle, and then turned right through the doorway into the roll storage warehouse. Continuing to drive forward with the roll in front of him, he drove toward the designated storage location, indicated by 2- by 4-inch wood planks in one of the paper storage rows (See Figure 1 and Drawing 1). The police report stated that the forklift driver indicated it was the company’s policy to honk the horn on the forklift every time the forklift came to a mirror. The driver indicated he had complied with this policy and honked his horn at all of the aisle intersections and at the entrance to the roll storage area. The driver had been carrying the paper roll between 6 inches and 12 inches from the floor. The top of the paper roll was estimated to have been 66 to 72 inches above the floor.
The incident was not witnessed. The forklift driver stated to the police that he did not see the decedent as he entered the warehouse area. He indicated he was driving approximately twice walking speed. It appeared that the decedent was walking on an angle from the supervisor’s office to the shipping and receiving office. The forklift was approximately 10 feet from its destination when the forklift was stopped. The driver looked to his right. On the ground, he could see the decedent’s head, just to the right of his right rubber tire and the decedent’s shoulder pressed up against this tire. The driver backed off the decedent.
The forklift driver immediately called for assistance on his company-issued radio. He ran to the supervisor’s office, banged on the window to attract the supervisor’s attention, and screamed to have someone call 911. He ran back to the decedent and saw that he was having trouble breathing. The driver detected a heartbeat and administered two to three breaths of air before other workers took over. Emergency response arrived and the decedent was declared dead at the scene.
The forklift driver stated to the MIOSHA compliance officer that he was instructed by the decedent to drive in reverse if his vision was obstructed but if he could see over the load, he did not have to drive in reverse. The MIOSHA compliance officer also indicated in the MIOSHA file that additional forklift operators had been interviewed. These operators also told the MIOSHA compliance officer that the decedent had instructed them that they could drive forward if they could see over the paper roll.
To simulate the forklift operator’s line of vision, the firm representative raised the paper roll to six inches above the floor. Figure 5 was taken by the MIOSHA compliance officer as he positioned himself in the forklift to the approximate line of vision of the forklift driver. The officer observed that the roll obstructed forward vision – as the officer looked over the roll, the officer could not see the floor for the first 20 to 30 feet.
 |
|
Figure 5. Simulated forklift driver forward view when seated in seat.
|
The decedent was 5 feet 6 inches tall, which placed the top of his head at the same height as the top of the roll if the roll was carried 6 inches above the floor. If the roll had been carried at 12 inches above the floor, it would have been 6 inches above the decedent’s head.
Back to Top
Cause of Death
The cause of death as stated on the death certificate was multiple blunt force injuries. Toxicological analysis showed no alcohol or prescription or illegal drugs present in his system.
Back to Top
Recommendations/Discussion
The employer should revise its forklift safety rule regarding driving the forklift in the direction that affords the “best visibility” to clarify and require the operator to trail a load when a driver’s forward vision is obscured.
The safety policy indicated that the forklift driver must “always drive in the direction that affords the best visibility.” At the time of the incident, there appeared to be a departure from the employer’s policy of “best visibility” and the training the employees received. The decedent, who trained the forklift drivers, appeared to have indicated during his training that if the driver could see over the load, then the driver could drive in a forward direction. It appears that the decedent may have interpreted the policy statement that an ability to see over the load could be acceptable for meeting the requirement of “best visibility.” Another possibility was that he may not have fully understood the requirement, as it did not provide a more direct instruction that complied with the requirements of MIOSHA General Industry Safety and Health Powered Industrial Truck Standard, Part 21, Rule 2185. The driver involved in the incident, although he may have been able to see over the load, had an obstructed forward view and did not have the best visibility as described in the safety program. The Powered Industrial Truck Standard, Part 21, Rule 2185 addresses the requirement for a clear view during operation. Rule 2185 states: “An operator shall look in the direction of and keep a clear view of the direction of travel. When moving loads blocking the forward visibility, for safe handling, an operator shall drive the truck with the load trailing.” To avoid any confusion in the future, the employer should revise the language from “best visibility” in the safety program to address obstructed vision and the requirement to operate the load in reverse if forward vision is obstructed.
Employers should continually stress the importance of adherence to established safe work procedures.
Prior to the incident, the company did not routinely enforce its written safety policies concerning forklift operation and pedestrian safety. The safety director indicated to the MIFACE researcher that greater attention is now being paid to enforcement of forklift operators trailing their load when vision is obstructed. The director did not discuss, and the MIFACE researcher did not ask, whether the attention is also being paid to ensuring pedestrians walk only in the designated aisles instead of taking short-cuts through plant areas. The company pedestrian safety section had clearly stated policies concerning the requirement for pedestrians to use pedestrian aisles. The decedent was not in a designated walkway, and if he had been, the incident would have been avoided because he would not have been in the travel path of the forklift.
The company should review the locations of the designated pedestrian aisleways to determine if they are appropriately located for pedestrian travel.
The aisleways in the warehouse area were at the perimeter of the room. This made it inconvenient for employees to travel from one area to another and therefore indirectly encouraged employees to take short-cuts. The company should review existing pedestrian traffic areas to determine if aisleway locations discourage their use and where appropriate, designate other walk way locations. Material handling and placement should also be included in this study.
The company should consider using a highly visible hard hat color (such as yellow or orange) and when job appropriate, the use of reflective vests for pedestrians.
The paper rolls MIFACE observed at the time of the site visit were white. A white hard hat blended in with the surroundings and could make it more difficult for a forklift operator to see a pedestrian who was not in an aisleway. To enhance pedestrian visibility, non-white hard hats should be considered, as well as the use of reflective vests. The MIFACE researcher has conducted several fatality investigations where pedestrians were required to wear a reflective vest when walking through the manufacturing facility.
References
MIOSHA standardsexternal icon cited in this report may be found at and downloaded from the MIOSHA, Michigan Department of Labor and Economic Growth (DLEG) website at: www.michigan.gov/mioshastandards. MIOSHA standards are available for a fee by writing to: Michigan Department of Labor and Economic Growth, MIOSHA Standards Section, P.O. Box 30643, Lansing, Michigan 48909-8143 or calling (517) 322-1845.
- MIOSHA General Industry Safety and Health Standard, Powered Industrial Trucks, Part 21.
Michigan FACE Program
MIFACE (Michigan Fatality Assessment and Control Evaluation), Michigan State University (MSU) Occupational & Environmental Medicineexternal icon, 117 West Fee Hall, East Lansing, Michigan 48824-1315; http://www.oem.msu.edu/MiFACE_Program.aspx. This information is for educational purposes only. This MIFACE report becomes public property upon publication and may be printed verbatim with credit to MSU. Reprinting cannot be used to endorse or advertise a commercial product or company. All rights reserved. MSU is an affirmative-action, equal opportunity employer. 6/3/09
MIFACE Investigation Report # 08MI010 Evaluationpdf iconexternal icon (see page 9 of report)