
Company President Killed When Forklift Overturns-- North Carolina
FACE 9701
SUMMARY
A 43-year-old male company president/co-owner (the victim) died as a result of injuries he sustained after a forklift he was operating overturned. The victim and the director of field operations (the witness) were in the process of unloading materials from a tractor trailer when the incident occurred. The victim had completed unloading material from one side of the trailer and drove to the back of the trailer for another load. He drove the forklift down and alongside the trailer and then steered the forklift left around the corner to go behind the trailer. In making the turn, the forklift began to tip over and the victim tried to jump clear. The forklift overturned on its right side and the victim was pinned to the concrete driveway by the roll-over/falling object protection structure (ROPS/FOPS) (Figure 1). The witness ran to the area and turned off the forklift, then summoned the emergency medical service (EMS). The EMS arrived about 10 minutes later, removed the forklift from the victim, and determined the victim was dead. The coroner arrived about 25 minutes after the incident occurred and officially pronounced the victim dead at the scene. NIOSH investigators concluded that, to prevent similar occurrences, employers should:
- ensure that only trained and authorized personnel be permitted to maintain, repair, adjust, and inspect industrial trucks (e.g., forklifts) in accordance with manufacturer’s specifications
- retrofit forklifts with seat belts
- inspect roll-over/falling object protection structures for damage and repair where applicable.
INTRODUCTION
On September 18, 1996, a 43-year-old male company president/co-owner (the victim) died after being pinned to a concrete driveway by the ROPS/FOPS on a forklift after it overturned. On September 30, 1996, officials of the North Carolina Occupational Safety and Health Administration (NCOSHA) notified the Division of Safety Research (DSR) of the occurrence, and requested technical assistance. On October 9, 1996, a DSR safety specialist reviewed the case file and photographs taken at the incident site with the compliance officer assigned to the case. On October 10, 1996, the safety specialist visited the incident site and met with the director of field operations, the victim’s widow, and the county coroner to further discuss the case and examine the forklift.
The employer in this incident was an advertising-sign design, fabrication, and installation company, which had been in business for 22 years. The company employed 30 workers and had been partially owned by the victim, who was also the company’s president. The victim was responsible for management of the plant’s safety program and maintenance of the forklift. The company had a written safety program, and training was performed on the job. The victim had been president/co-owner of the company for 22 years. He had also operated the forklift involved in the incident on a routine basis for 22 years. This was the first fatality experienced by the company.
INVESTIGATION
The company had received a shipment of steel tubing via flatbed tractor trailer, which had to be unloaded. The victim and the director of field operations (the witness) arrived at the plant about 6:40 a.m. on the day of the incident to unload the tubing. As the witness began other chores, the victim began unloading the flatbed trailer using a 1961-62 Clark, model FL1002, forklift. The forklift had a 2,000-lb. capacity and had been retrofitted with a steel roll-over/falling object protection structure (ROPS/FOPS), but had not been retrofitted with a seat belt. The propane-powered forklift was approximately 9-feet 8-inches long, 3-feet wide, with a wheel base 45-inches long by 28-inches wide. The solid-rubber tires were extremely worn. The front tires measured 192-inches in diameter by 6-inches wide, while the rear tires were 142-inches in diameter and 4-inches wide. The forklift had front-wheel drive and rear-wheel steering. Also, axle-stop steel bars, about 9-inches long and 1-inch wide, by 3/8-inch thick, were positioned above each rear-wheel axle. The bars were welded to the frame of the forklift and extended downward to within 3/4-inch of the top of the axle, next to the tire rim (Figure 2).
The axle-stops prevented the body of the forklift from contacting the tires, and limited the amount of vehicle lean due to shifting loads or excessive speeds in turns.
By 8 a.m. the victim had unloaded two-thirds of the steel tubing from the flatbed trailer. He then drove the forklift, with the forks about 6 inches above the concrete driveway, down the left side of the trailer. As he approached the rear of the trailer, traveling about 5-miles per hour down a 3-percent grade, he turned left to go behind the trailer. At that time, the forklift began to tip over and the victim tried to jump from the operator’s seat to the concrete driveway. As the forklift over-turned on its right side, the victim became pinned between the top of the ROPS/FOPS and the concrete drive. The witness looked in the direction of the victim at the time the forklift tipped over and saw the victim get pinned. He ran to the scene, turned off the forklift, and summoned the EMS. EMS arrived in about 10 minutes and with the aid of an air bag and compressor, lifted the forklift off the victim. The victim was checked immediately for vital signs, but none were found. The coroner arrived 25 minutes later and pronounced the victim dead at the scene.
CAUSE OF DEATH
The coroner’s report listed the cause of death as head and neck trauma.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should ensure that only trained and authorized personnel be permitted to maintain, repair, adjust, and inspect industrial trucks (e.g., forklifts), and only in accordance with manufacturer’s specifications.
Discussion: The victim, in addition to being the company president, provided maintenance to the forklift. Although he had general mechanical training he was not trained and authorized to maintain, repair, adjust and inspect forklifts. The American Society of Mechanical Engineers ASME/ANSI B56.1-1993, 6.2.7 Safety Standard for Low Lift and High Lift Trucks states “Brakes, steering mechanisms, control mechanisms, warning devices, lights, governors, lift overload devices, guards and safety devices, lift and tilt mechanisms, articulating axle stops, and frame members shall be carefully and regularly inspected and maintained in a safe operating condition.” The axle stop located over the right-side-rear articulating axle had been damaged sometime prior to the incident. The axle stops are critical in the operation of the forklifts because they limit the amount of lean of the forklift in turns, and in instances of shifting loads which might cause an overturn. The axle stop, according to manufacturer’s specifications, should have been positioned directly above and within 3/4 of an inch of the axle. The stop was off-center by 2 inches to the side and 2 inches above the axle. Forklifts, like other industrial and agricultural equipment, have articulating steering axles to allow them to go over uneven terrain. Movement of the articulating axle is limited by axle stops which are normally welded directly into the frame of forklifts. Additionally, if the axle stop is not aligned properly with the axle or is damaged or even missing, the forklift tires may contact the frame, causing the machine to stop suddenly and contribute to the potential for an overturn. Also, slack in the steering mechanism required the operator to turn the steering wheel slightly more than half a revolution before the tires/wheels would start to turn. These factors of the articulating-axle stop being damaged/distorted and out of position, the slack in the steering mechanism, and the forklift being operated around a corner down a 3-percent grade, all contributed to the overturn of the forklift and the eventual death of the victim.
Recommendation #2: Employers should retrofit forklifts with seat belts.
Discussion: The forklift, which was manufactured in 1961/62, was not originally equipped with ROPS/FOPS but had been retrofitted with a steel ROPS/FOPS system sometime prior to the incident. However, seat belts had not been installed. Owners of machinery (e.g., forklifts) equipped with ROPS/FOPS should contact forklift manufactures to determine how seat belts could be installed, have the seat belts installed, and require the operators of such machinery to always wear the seat belts while operating machinery. Wearing a seat belt while operating machinery will keep the operator from being thrown off the vehicle while driving over rough terrain, making sharp turns, or in the event of machine overturn. Wearing seat belts will assure that the driver remains in the ROPS/FOPS-protected zone. In this case, remaining on the forklift may have been a safer choice than attempting to jump from it.
Recommendation #3: Employers should inspect roll-over/falling object protection structures for damage and repair where applicable.
Discussion: After an incident of this nature, the ROPS/FOPS on any machinery involved in an overturn should be inspected by a qualified mechanic, to determine the extent of damage to the ROPS/FOPS system and have the system repaired to its original standards. If the ROPS/FOPS systems is not repaired to its original standards, the system may not protect the operator as originally designed in any future incidents.
REFERENCES
The American Society of Mechanical Engineers, ASME B56.1-1993, Safety Standards for Low Lift and High Lift Trucks, 1993.
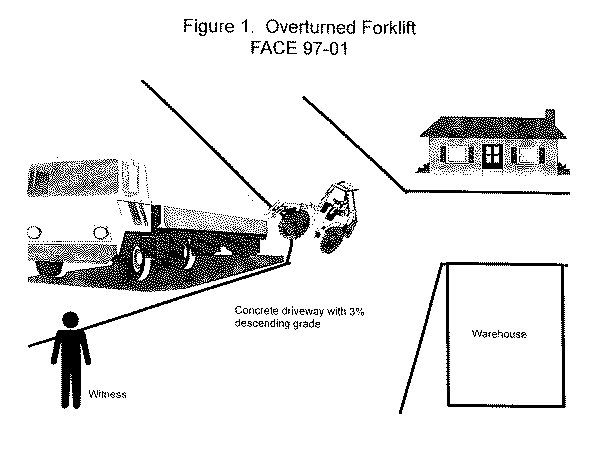
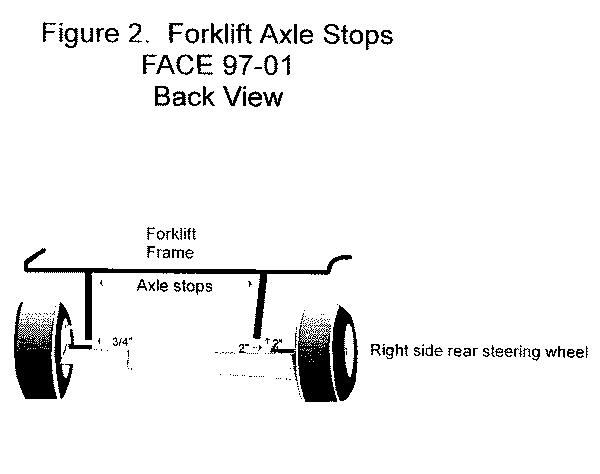
Figure 1.
Figure 2.
Return to In-house FACE reports