
Assistant Grain Elevator Supervisor Dies After Being Engulfed in Shelled Corn--North Carolina
FACE 9416
SUMMARY
A 61-year-old assistant grain elevator supervisor (the victim) died after being engulfed in shelled corn inside a grain elevator. The victim and a co-worker entered the elevator to shovel corn toward a rotating auger at the base of the sloped floor. Holding onto a rope mounted on the inside of the elevator, the victim walked on the corn, around the inside of the elevator and down the floor toward the auger. As he did so, the remaining corn on the floor (approximately 800 bushels) slid down on the victim, knocking him off his feet. The co-worker tried to pull the victim from the corn, but was unsuccessful. The co-worker exited the elevator to get additional help. When he returned with a second co-worker the victim was engulfed in the corn, with only one hand protruding above the surface. The second co-worker exited the elevator to turn off the auger while the co-worker ran to the company office to summon the fire department and the emergency medical service by phone. A door at the bottom of the elevator was opened in an attempt to drain the corn off the victim and a vacuum was used to remove the corn from on top of the victim. When the corn was removed, the victim was removed from the elevator (45 minutes after the incident occurred) and transported to the local hospital where he was pronounced dead on arrival. NIOSH investigators concluded that, to prevent similar occurrences, employers should:
- develop and implement a comprehensive safety program that clearly documents procedures for safe entry into confined spaces such as those contained in the NIOSH criteria document “Working in Confined Spaces” (NIOSH Publication 80-106) and “A Guide to Safety in Confined Spaces” (NIOSH Publication 87-13)
- equip confined spaces containing unstable material with life lines and harnesses at their entrance point(s), and train workers in their usage
- ensure that when work is being performed in a confined space containing unstable material, a standby person be utilized in a manner such that constant communication with the worker(s) inside the confined space can be maintained.
- instruct workers to enter confined spaces only when absolutely necessary and to strictly adhere to established confined space entry procedures
- prohibit workers from standing on or working from loose, granular materials, even when the surface appears to be stable.
INTRODUCTION
On September 11, 1994, a 61-year-old male assistant grain elevator supervisor died after being engulfed in shelled corn inside a grain elevator. On September 15, 1994, officials of the North Carolina Occupational Safety and Health Administration (NCOSHA) notified the Division of Safety Research (DSR) of this fatality, and requested technical assistance. On September 21, 1994, a DSR safety specialist investigated and reviewed the incident with an employer representative, the NCOSHA compliance officer assigned to the case, and the medical examiner.
The employer was a grain handling facility that had been in operation for 40 years and employed eight full-time workers. During the harvesting season, three additional employees were hired and the facility operated 24 hours a day (two 12-hour shifts). The company had no written safety program or procedures. Training was provided on the job, and safe job procedures were conveyed verbally. Company policy prohibited entrance into an elevator while the auger was running, or without safety belts and lanyards. This was the first traumatic fatality experienced by the employer. Previously, a worker suffered a fatal heart attack at the facility. The victim had worked at the facility for 16 years.
INVESTIGATION
The victim was employed at a grain handling facility that had 17 grain elevators of various sizes. Shelled corn was purchased, stored and dried in the elevators, then shipped as orders were received. Early in the harvest season, most of the corn was shipped by truck to poultry and livestock feed manufacturers. When the harvesting season was at its peak, shipments were made by rail.
Because the corn could be picked with a moisture content as high as 30%, it had to be passed through a drier several times to prevent it from molding or souring. The corn was dried as it was passed between elevators. The corn was transferred between elevators by means of an auger located at the bottom of the elevators.
The elevator involved in the incident was 60 feet high, 18 feet in diameter, and had a capacity of 10,000 bushels. The floor of the elevator was sloped at a 60E angle to allow the corn to be fed by gravity toward the auger at the base of the elevator. The sloped floor was 14-feet-high, 12 feet being above ground level (Figure). The top of the floor was accessed by a 18-inch by 24-inch steel-door opening located on the side of the elevator, 12 feet above ground.
On the day of the incident, the corn in the elevator was being transferred to a tank that fed the grain drier. When the elevator was almost empty (an estimated 800 bushels remained on the floor and sides), the victim (supervisor) and a co-worker entered the elevator to knock any corn from the sides of the elevator and to shovel any corn remaining on the floor toward the auger. Against company policy, the men entered the elevator with the auger running, and without the required safety belts and lanyards that were available in the control room located adjacent to the elevator.
The co-worker stood in the vicinity of the door and pushed the corn toward the bottom of the sloped floor while holding onto the rope around the interior of the tank to which the lanyards could be attached. The victim walked around the inner wall toward the auger while holding onto the rope. As the victim approached the auger, the corn slid down the floor, knocking the victim off his feet. The gravity flow from the turning auger pulled the victim into the corn.
The co-worker walked around the floor and tried unsuccessfully to pull the victim from the corn. The co-worker exited the elevator and ran to another elevator to get a second co-worker to help. The two men returned to the elevator to find the victim engulfed in the corn with only his right hand above the surface of the corn. The two men tried to pull the victim from the corn, but were unsuccessful. The second co-worker went to the control room to turn off the auger, while the other co-worker ran to the office to have office personnel call the fire department and the emergency medical service (EMS).
A door at the bottom of the elevator was opened in an attempt to remove the corn, while workers inside the elevator used a pneumatic vacuum to remove the corn from above. The victim was removed from the elevator through the steel-door opening approximately 40 minutes after the incident occurred, and transported by the EMS to the local hospital, where he was pronounced dead by the attending physician.
CAUSE OF DEATH
The medical examiner lists asphyxiation due to being trapped in a grain elevator as the cause of death.
RECOMMENDATIONS/DISCUSSION
Recommendation #1: Employers should develop and implement a comprehensive safety program that clearly outlines procedures for safe entry into confined spaces such as those contained in the NIOSH criteria document “Working in Confined Spaces” (NIOSH Publication 80-106) and “A Guide to Safety in Confined Spaces” (NIOSH Publication 87-13).
Discussion: All employees who work in or around confined spaces should be aware of potential hazards, possible emergencies, and specific procedures to be followed prior to working in a confined space. These procedures should include, but not be limited to:
- testing air quality to determine adequate oxygen level and the presence of flammable and/or toxic gas/vapors
- ventilating the space to remove air contaminants
- monitoring the space to determine if a safe oxygen level is being maintained
- training employees in confined space entry, testing, and the use of personal protective equipment, safety harnesses, respirators, clothing, etc.
- stationing (a) stand-by person(s) outside the space for communication and visual monitoring
- providing for emergency rescue procedures
- identifying and controlling of the hazards associated with unstable surfaces.
Recommendation #2: Employers should equip confined spaces containing unstable material with life lines and harnesses at their entrance point(s), and workers should be trained in their usage.
Discussion: Life lines and harnesses should be present at the entrance(s) of confined spaces containing unstable materials and should be utilized by all persons entering the confined spaces. If these are not incorporated into the design of the elevator by the manufacturer, they should be installed by the user prior to worker entry into the confined space. Workers should then be trained in the proper use of this equipment. In this incident, life lines and harnesses were available at the control room near the elevator entrance instead of being at the entrance.
Recommendation #3: Employers should ensure that when work is being performed in a confined space containing unstable material, a standby person be utilized in a manner such that constant communication with the worker(s) inside the confined space can be maintained.
Discussion: A standby person, stationed outside of confined spaces containing unstable material (i.e., shelled corn), should maintain constant communication with the worker(s) inside the area. If visual contact cannot be maintained, the standby person should at least maintain constant voice contact. In this incident both workers were inside the space working, and, before additional help was summoned, valuable rescue time was lost.
Recommendation #4: Employers should instruct workers to enter confined spaces only when absolutely necessary and to strictly adhere to established confined space entry procedures.
Discussion: In this incident, it was not absolutely necessary for the workers to enter the grain elevator when the job began. The auger was still running and standard operating procedures prohibited entry until the auger has been turned off. Had the auger been turned off, the action of the shelled corn and its pull on the victim may have been lessened.
Recommendation #5: Employers should not allow workers to stand on, or work from, loose, granular materials, even when the surface appears to be stable.
Discussion: Employers should not only prohibit workers from standing on unstable surfaces while performing their assigned tasks, but should also require employees to wear safety harnesses or safety belts attached to life lines when working in the vicinity of unstable surfaces. Workers should be made aware of the hazards, such as engulfment, bridging, and crusting, associated with unstable surfaces. Workers should be instructed in the identification of these hazards and appropriate methods needed to avoid them.
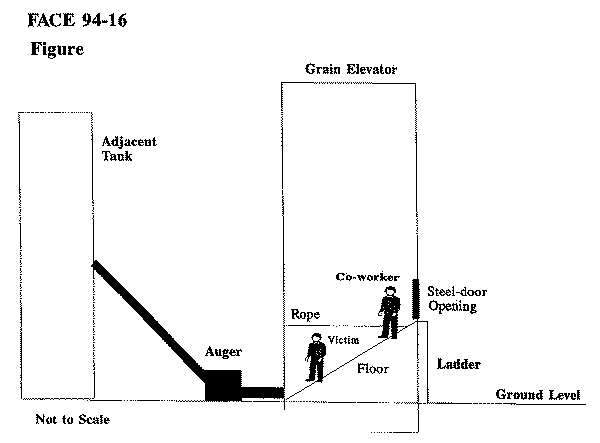
Figure.