Millworker Dies in Feed Storage Bin--Virginia
FACE 9234
SUMMARY
On August 31, 1992, a 56-year-old male millworker (the victim) died of suffocation after becoming engulfed in soybean hulls in a grain mill storage bin. The victim and two co-workers were unloading the soybean hulls from an open-topped indoor storage bin compartment when the material became lodged in the compartment. The victim positioned himself on the upper level of the multilevel feedmill building to attempt to dislodge the material with a flexible sewer tape. After load out operations had been completed, the co-workers could not locate the victim. He was later found dead inside the bin compartment, engulfed in the soybean hulls. The victim either entered or fell into the open-topped storage compartment and was engulfed when the bridged material collapsed during load out operations.
NIOSH investigators concluded that, to prevent future similar incidents, employers should:
- develop, implement, and enforce a written safety program which includes confined space entry and rescue procedures and training to ensure that workers assume that all stored materials are bridged and that the potential for entrapment and suffocation associated with stored grain and other loose materials is constant
- ensure that workers are protected from the engulfment hazards of open-topped bins by installing bin covers to prohibit entry
- consider installation of devices which will prevent stored granular materials from lodging on the inside of bins
- install standard railings with toeboards and intermediate rails around all openings where persons may be exposed to hazards of falls
- ensure that workers entering storage areas wear safety belts or harnesses equipped with properly fastened life lines
- ensure that safety signs are posted to warn workers of the hazards of working with stored grains and other loose materials.
INTRODUCTION
On August 31, 1992, a 56-year-old male millworker (the victim) died of suffocation after becoming engulfed in soybean hulls. On September 14, 1992, the Virginia Occupational Safety and Health Administration (VAOSHA) notified the Division of Safety Research (DSR) of the incident and requested technical assistance. On September 23, 1992, a DSR safety engineer traveled to the site and conducted an investigation of the incident. The investigator interviewed the general manager of the feedmill, a co-worker, and the VAOSHA compliance officer assigned to the case. Measurements and photographs of the site were obtained as well as copies of the death certificate and medical examiner’s report.
The employer was a regional farm bureau established in 1913, employing a total of 40 employees at various locations throughout the region, 5 of whom were millworkers employed at the feedmill where the incident took place. According to the general manager, the facility had been in existence in various capacities for about 80 years. Safety issues were the responsibility of the general manager, who reported to a board of directors. The employer did not have a written safety program; however, safety policies were communicated verbally from the general manager to employees. There was no formal training program and specific job duties were learned on the job. The victim had been employed as a millworker for 10 years, all at the incident site. This was the first fatality experienced by the farm bureau since its inception.
INVESTIGATION
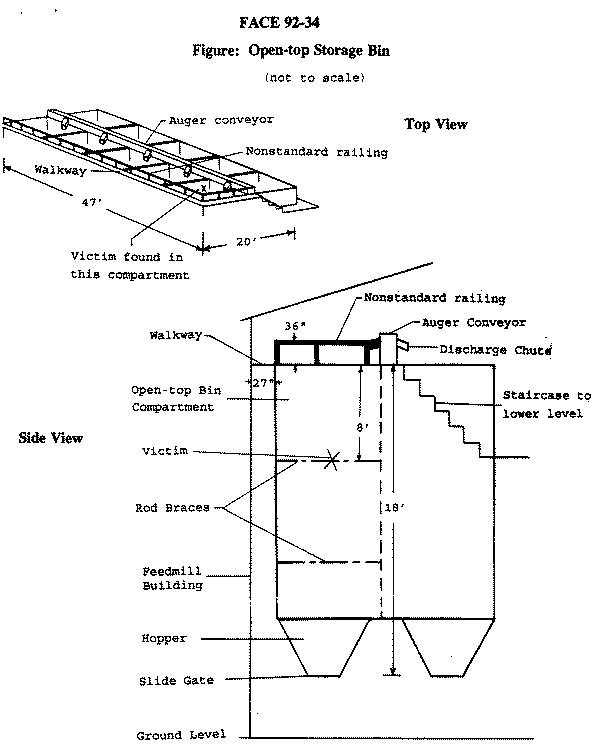
The incident occurred in a 10-compartment open-topped storage bin, which was approximately 47 feet long, 20 feet wide, and 18 feet deep (Figure). The top of the bin was accessed by a 27-inch-wide walkway around two sides and one end. The compartments were arranged in two rows of five, with an auger-type conveyor centrally located along the top of the bin. The conveyor loaded material into each compartment through individual discharge chutes dropping from the side of the conveyor trough. Load out was accomplished by another auger-type conveyor system located under the compartment hoppers. At the time of the incident, a nonstandard railing had been installed around one side of the bin, 36-inches above the walkway.
On the day of the incident, the victim and co-workers started work at the normal 7 a.m. start time. Throughout the morning the victim and his co-workers had been engaged in loading trucks with material from the bin compartments. At about 11 a.m. they began loading a truck with soybean hulls. They had almost completed loading the truck when the compartment was emptied.
They then switched load out to the end compartment, which had been filled 3 weeks earlier with 18.6 tons (37,220 lbs.) of soybean hulls. The victim and his two co-workers attempted to unload the compartment by opening the slide gate under the compartment hopper and pounding on the hopper sides to dislodge the hulls. When this failed, the victim ascended the stairs to the walkway around the top of the bin, and attempted to dislodge the bridged material by dropping the weighted end of a flexible sewer tape into the soybean hulls. Shortly after the victim left, the co-workers observed the hulls begin to flow out of the compartment. They proceeded to load out the material into 300 pound capacity wheeled boxes, to be transferred into the waiting truck. After four boxes had been loaded, the truck was full and the co-workers shut down the conveyor system. Thinking that the victim would know that the truck was loaded when he heard the conveyor machinery shutdown, they proceeded to eat lunch. After a short period, they decided to look for the victim, since he had not joined them for lunch. The area around the bin was searched without success and one of the co-workers expressed concern that the victim may have fallen into the bin. They then decided to load out the contents of the bin compartment to see if the victim was inside. The conveyor machinery was started and the contents were loaded out into boxes, exposing the victim lying on two rod braces approximately 8 feet below the top of the compartment. One of the co-workers notified the local emergency medical service, (EMS) which responded in about 10 minutes. The victim was removed from the compartment by EMS personnel, transported to a local hospital and pronounced dead at 1:15 p.m.
CAUSE OF DEATH
The medical examiner determined the cause of death as suffocation.
RECOMMENDATIONSDISCUSSION
Recommendation #1: Employers should develop, implement, and enforce a written safety program which includes confined space entry and rescue procedures and training to ensure that workers assume that all stored materials are bridged and that the potential for entrapment and suffocation associated with stored grain and other loose materials is constant.
Discussion: The co-worker interviewed during this investigation indicated that, when the compartment had been filled 3 weeks prior to the incident, it was necessary for the millworkers to trim the top of the load to prevent material from spilling over into adjacent compartments. This had been done with shovels while the millworkers were standing on top of the material in the bin compartment. There had been no problems with this procedure at the time of loading. While it is not known whether or not the victim entered the bin compartment of his own volition, past experience of the workers with this particular material, soybean hulls, indicated to them that standing on top of the material in the compartment was an acceptable practice. NIOSH has prepared an Alert detailing the hazards associated with the storage of grain and other loose granular materials (NIOSH Publication No. 88-102). NIOSH has published other materials which can also serve as the basis for developing a comprehensive confined space entry program (NIOSH Publication Nos. 80-106, 86-116, and 87-113.) The physical properties of granular materials in bins are such that workers may easily develop a false sense of security while on top of the material, because the exact set of conditions necessary for bridging and subsequent collapse of the bridged material may only occur infrequently. Bridging occurs in storage bins that contain loose materials such as soybean hulls; it is caused by the material clinging to the sides of the bin. As the bin is emptied from the bottom, the material clinging to the bin sides lodges there, forming a bridge over the void previously occupied by the withdrawn material. The bridge may collapse without warning, entrapping workers who are standing on the bridge and who may be unaware that the surface is unstable. Workers may not be aware that the potential for engulfment is constantly present. Safety programs should prohibit entry into bins unless absolutely necessary; when entry is necessary, workers should be adequately protected from the hazards of confined spaces, such as engulfment. Workers may be protected by using properly secured safety harnesses and lanyards and by stationing standby persons outside of the bin.
Recommendation #2: Employers should ensure that workers are protected from the engulfment hazards of open-topped bins by installing bin covers to prohibit entry.
Discussion: The bin compartment in this incident was open at the top and guarded by a 36-inch-high railing. It is conceivable that the victim fell over the top or slipped under the railing while trying to dislodge material with the sewer tape. After the incident, the tape was found routed under the railing, with the weighted end in the compartment and the other end on the walkway. Bins can be covered with solid sheeting, or if necessary, a grating could be installed, to allow access for tools while prohibiting intentional or inadvertent entry by workers.
Recommendation #3: Employers should consider installation of devices which will prevent stored granular materials from lodging on the inside of bins.
Discussion: Devices are available which, when installed in a bin, can prevent material from bridging or can dislodge bridged material without the need for workers to be exposed to the hazards of confined spaces or unstable materials. These devices range in complexity from a simple chain hung down the center of the bin, to mechanical vibrators. In this incident, one of the compartments of the bin had been equipped with a chain attached to the ceiling of the building and hung down inside the compartment near its center. This compartment normally stored soybean meal, a material which readily bridges. Ambient vibration present when machinery is operated inside the building causes the chain to oscillate, thereby minimizing lodging of the surrounding material. A similar arrangement could be applied to other compartments containing granular materials.
Recommendation #4: Employers should install standard railings with toeboards and intermediate rails around all openings where persons may be exposed to hazards of falls.
Discussion: In this incident, a 36-inch-high railing had been installed around the edge of the bin compartments and the walkway. Standard 42-inch-high railings as specified in 29 CFR, 1910.23(e) should be installed around all floor openings where persons are exposed to fall hazards. Such railings should be equipped with toeboards and intermediate railings, as well as a top rail. Although this incident was unobserved, evidence suggests that the victim may have fallen through or over the railing and into the bin compartment during unloading operations. Additionally, railings could provide an anchor point for safety lines and lanyards worn by workers when working over the bin compartment.
Recommendation #5: Employers should ensure that workers entering storage areas wear safety belts or harnesses equipped with properly fastened life lines.
Discussion: Although it is not known whether the victim intentionally entered the bin compartment during the incident or fell into it, workers at this facility had entered prior to the incident without the protection of properly secured safety belts or harnesses. When entering areas where granular materials are stored, the potential for engulfment is always present. If the storage space absolutely must be entered, safety belts or harnesses secured to life lines can protect the workers by arresting their fall when bridged material collapses, and by providing a means for rescue retrieval.
Recommendation #6: Employers should ensure that safety signs are posted to warn workers of the hazards of working with stored grains and other loose materials.
Discussion: Although a nonstandard railing had been erected around the accessible sides of the open-topped bin compartment, there were no warning signs posted to alert workers to the hazard of potential entrapment and suffocation present if the compartment was entered. Employers should treat all grain bins, silos and other areas where grain is stored as confined spaces. Posting readily observable warning signs where workers may be exposed to the hazards of confined spaces can reinforce worker training and serve as a constant reminder of the hazards associated with the storage of granular materials.
REFERENCES
NIOSH Criteria for a Recommended Standard … Working in Confined Spaces, December 1987, U.S. Department of Health, Education and Welfare, Publication No. 80-106.
NIOSH Alert, Request for Assistance in Preventing Occupational Fatalities in Confined Spaces. January 1986, U.S. Department of Health and Human Services, Publication No. 86-110.
A Guide to Safety in Confined Spaces. July 1987, U.S. Department of Health and Human Services, Publication No. 87-113.
NIOSH Alert, Request for Assistance in Preventing Entrapment and Suffocation Caused by the Unstable Surfaces of Stored Grain and Other Materials. December 1987, U.S. Department of Health and Human Services, Publication No. 88-102.
NIOSH Alert, Request for Assistance in Preventing Entrapment and Suffocation Caused by the Unstable Surfaces of Stored Grain and Other Materials. December 1987, U.S. Department of Health and Human Services, Publication No. 88-102.
29 CFR, 1910.23(e) Code of Federal Regulations, Washington, D.C.: U.S. Government Printing Office, Office of the Federal Register. June 27, 1974.