
Apprentice Electrician Electrocuted
FACE 89-50
Introduction
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), performs Fatal Accident Circumstances and Epidemiology (FACE) investigations when a participating state reports an occupational fatality and requests technical assistance. The goal of these evaluations is to prevent fatal work injuries in the future by studying the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interact.
On August 23, 1989, a 23-year-old male apprentice electrician was electrocuted while making a connection for a light fixture in a junction box.
Contacts/Activities
State officials notified DSR of this fatality and requested technical assistance. On September 14, 1989, a safety engineer from DSR traveled to the site and conducted an investigation, reviewed the case with company officials, photographed the incident site, and met with state compliance officials to obtain information about the events surrounding this incident.
Overview of Employer’s Safety Program
The employer, an electrical contractor with 40 employees, has been in business for 15 years. The company has a designated part-time safety officer, but has no formal safety program. The company does a wide range of electrical work in construction, remodeling, and home repairs. Safety is handled through on-the-job training, observation of work practices by supervisors, and printed handouts of safety topics that management deems appropriate.
The victim had previously worked for the company for 2 years. He left the company for about 2 years and returned to work at the beginning of 1989. While working for another employer the victim received electrical burns on his hands. The victim had recently taken the examination to be classed as a journeyman electrician but had not received the results.
Synopsis of Events
The employer had a contract to install wiring and fixtures in an office complex that was located behind a new shopping mall. The third floor of the office complex was being hurriedly prepared for a tenant. The off-site designer made daily changes (e.g., fixture locations) to electrical system blueprints, and transmitted the revised drawings to the jobsite via a facsimile transmission (fax) machine.
The lighting system is a 3-phase, 4-wire, 277/480-volt system. The wires for two circuits (three hot wires and one neutral wire per circuit) were run in one conduit down a central hall with junction boxes installed for branch circuits to individual lights. The lights are mounted in a metal gridwork, flush with ceiling tiles. System grounding is achieved through the metal conduit. Work had been completed on one side of the hall and the victim was installing conduit and fixtures on the other side.
At the time of the incident, the victim was wiring in a light fixture at a junction box and was in contact with the gridwork. During the work, he received a shock, came down from the fiberglass ladder, said “cut the juice,” and collapsed. Two co-workers immediately started cardiopulmonary resuscitation while another worker called the emergency service number. The phone call was made from an elevator which had the same number as other elevators in the mall-office complex. The person at the emergency service answering location asked if the call was coming from the place where the victim was located. (The number and location were available to the emergency service person.) The caller replied that it was, neither one realizing that the mall was the listed address for the phone number. The emergency rescue team went to the mall searching for the victim, while the co-workers waited with the victim for assistance in the office complex. Approximately 20 minutes elapsed before the rescue team reached the victim. The victim was then transported to a local hospital where he was pronounced dead-on-arrival.
Work was stopped for that day and the area secured until an investigation could be made by the company. The next day no energized lines could be detected in the junction box where the victim was working when he received the fatal shock. The panel box was in a closet, but was not locked. After work in the area was finished, further investigation revealed that the two neutral conductors in the same conduit run had been cross-wired at a junction box. That is, the neutral wire in the de-energized circuit was mistakenly connected to the neutral wire of an energized circuit back at the junction box. Company officials believe that the victim had previously, inadvertently cross-wired the neutral conductors, which subsequently allowed electricity to flow from the live circuit on the completed side of the building through a light fixture, to the circuit on which the victim was working. When he handled the energized neutral conductor to make the connection, his body provided a path to the metal gridwork he was touching, which was connected to the building structural steel.
The Figure on page 5 demonstrates how it could be possible for the victim to be electrocuted due to the crossed neutral wires. The circuit breaker had to be closed and the light switch in the “on” position on the live circuit to allow current to flow through the light fixture to the neutral line wire of the parallel circuit.
Cause of Death
The medical examiner ruled that the cause of death was electrocution.
Recommendations/Discussion
Recommendation #1: Employers should limit panel box access to electricians and lock it (if possible) or tag out circuits being actively worked on.
Discussion: The preferred method to control access would be to lock out the circuits where possible. However, the individual twenty-amp circuit breakers such as those used on this project are not designed to be locked out. The front of the panel box, which can be locked, was not in place because wires were still being installed in the panel. At a minimum, electricians should open the circuit breakers for the circuits they will be working on, and tape across the circuit breakers. Then a tag should be located at the circuit breakers to inform other workers who is working on those circuits. Additionally, secure temporary barriers should be considered that would keep unauthorized people out of the panel box area. This could be a temporary gate or door with a lock that only the electricians have the key to open. This would limit access to the panel box to electricians. The electricians should also be trained in lockout/tagout procedures so that any circuits being worked on are either locked out or tagged. These procedures need to be used and compliance enforced.
Recommendation #2: All conductors in the immediate work area should be tested by the worker to verify that they are de-energized before starting to work.
Discussion: An ohm meter or a voltage indicator meter should be used by the electrician to determine that all lines are de-energized before starting work. This simple test should detect problems such as incorrect wiring or unsuccessful de-energization. The instruments required to do this are inexpensive and easy to carry, and would not impose a significant burden on the worker. In a job such as this, where changes were being made on a regular basis, the extra precaution of testing the circuit might have prevented the incident.
Recommendation #3: Wiring done by apprentice electricians should be checked by a journeyman.
Discussion: The victim was an apprentice electrician with 4 to 5 years of experience. Due to the rush nature of the job (3 weeks after the incident the offices were occupied) and the fact that changes were being made regularly on the electrical blueprints, it would have been good practice to have a journeyman electrician check the apprentices’ work.
Recommendation #4: The company should develop and implement a comprehensive safety training program.
Discussion: The company, at present, has an informal safety training program, which covers areas of concern as management becomes aware of them. There is no plan to cover various safety hazards on a formal basis. The company does have a good inspection program for ladders. A formal safety training program to inform employees of potential hazards needs to be developed and implemented.
Recommendation #5: The jobsite supervisor should evaluate all revisions to the original blueprints to identify potential hazards that these revisions might create.
Discussion: Since the revisions to the blueprints were being sent directly to the jobsite, the contractor did not have a chance to review the modifications. For this reason, the supervisor at the jobsite should review all the revisions to the system to identify potential hazards. The changes were being made on blueprints, with small sections of the marked-up blueprint being sent by FAX machine to the jobsite. Some of these changes involved rewiring connections in various junction boxes. As a result of the rush nature of the job and the many design changes, the potential for error was increased. The evaluation of the changes by the jobsite supervisor might have identified areas where potential electrical hazards could exist, such as areas where connections were to be rewired. Once these areas were identified, they should have been carefully inspected to ensure proper wiring techniques.
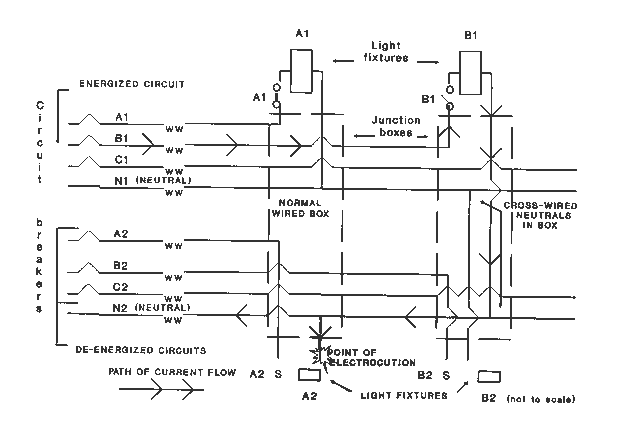
Figure. Cross-wired Neutrals