
Electrical Contractor Crew Leader Electrocuted
FACE 88-45
Introduction
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), performs Fatal Accident Circumstances and Epidemiology (FACE) investigations when a participating state reports an occupational fatality and requests technical assistance. The goal of these evaluations is to prevent fatal work injuries in the future by studying: the working environment, the worker, the task the worker was performing, the tools the worker was using, the energy exchange resulting in fatal injury, and the role of management in controlling how these factors interacts
On September 1, 1988, a 35-year-old male crew leader for an electrical contractor was electrocuted while connecting a newly installed, concrete pad-mounted transformer for a new residence.
Contacts/Activities
State officials notified DSR of this fatality and requested technical assistance. On September 22, 1988, a research safety specialist conducted a site visit, met with an employer representative, and discussed the incident with the county coroner and the Occupational Safety and Health Administration (OSHA) compliance officer.
Overview of Employer’s Safety Program
The victim was employed by an electrical contractor who has been in operation for over 19 years. The contractor employs 300 workers. The contractor has a written safety policy, a comprehensive safety and training program, and a full-time safety officer. The employees receive periodic training and retraining. Daily tailgate safety meetings, including discussions of safe work procedures for hazard control, are conducted at each job site. The safety officer also visits each crew at least once a week to conduct a site evaluation and job crew safety meeting.
The employer has developed a list of “absolute do’s and don’ts” as primary jobsite safety rules. These rules are carefully explained to the workers and laminated copies are posted in all company vehicles and at all jobsites. A violator of these rules is sent home after twice committing an infraction. The third infraction warrants dismissal.
The employer implements an additional safety measure. Multiple grounding of trucks and equipment is required in an effort to prevent electrocutions due to inadvertent energization of this equipment. This procedure is not required by legal or consensus standards, but is felt by the company to be essential in reducing workers, risk of injury during line work.
Three weeks prior to the incident the victim completed a 1-week training course in underground power transmission. The victim, with 10 years of experience working for the contractor, was considered by the employer as “the best and most experienced underground transmission crew leader” in the company.
Synopsis of Events
The employer had been contracted by the local electrical utility company to install encased transformers on concrete pads (i.e., pad-mounted transformers) for a 15,000-volt underground transmission system. The pad-mounted transformers were being installed for new residences under construction.
On the day of the incident the victim (crew leader) and two crew members were given the work order to splice a previously installed, pad-mounted transformer into an existing underground 7,200-volt primary cable. The primary wire was one of three that originated in a main switch cabinet approximately three-quarters of a mile away. The primary continued to a second switch cabinet which contained no fuse holders and was de-energized (see Figure). Therefore, the current could reach the incident site (transformer) only from the direction of the main switch cabinet. The victim went to an adjacent transformer he thought was on the incoming power side of the primary line, de-energized the line (i.e., opened a switch) and grounded it. The victim then returned to the worksite and told the crew members to cut the primary wire and begin the splicing operation. When the primary wire was cut an arc occurred. The victim then realized that the worksite was between the de-energized transformer and the power supplied by the main switch cabinet. He also knew that the arc would cause the fuse on the primary wire in the main switch cabinet to blow.
After instructing the crew members to stop working until his return, the victim drove to the main switch cabinet and removed the blown fuse and its holder. He did not ground the primary wire at this point as required by company procedures. (Before splicing operations had begun, the victim and crew had been visited by the employer’s district supervisor and safety officer. The proper procedures to be followed, including grounding procedures for this task, were reviewed during this visit.)
The victim returned and instructed the crew members to test both ends of the primary wire to ensure that they were de-energized. When both ends of the primary wire were found to be de-energized the victim instructed the crew members to prepare the ends for connection to the transformer.
Although company procedures required that both ends of the primary wire be grounded, no grounds were installed. The victim went to his truck and replaced the blown fuse in the holder he had removed from the main switch cabinet. He left this unit in the truck. He then walked to the adjacent transformer, removed the ground wire he had installed, and returned the transformer to normal service (i.e., closed the switch). The primary wire remained de-energized because the fuse and fuse holder had been removed from the main switch cabinet. The victim returned to the worksite and informed one of the crew members that he would finish work on that end of the primary wire to speed up operations.
It was determined during investigation that the victim was working on the end that returned to the main switch cabinet from which he had removed the fuse and fuse holder. The victim had been working on the wire for 1 1/2 minutes in a squatting position when he groaned and fell backwards onto the crew member who was observing him. The crew member received a shock and jumped away from the victim. The crew members pulled him away from the transformer and began cardiopulmonary resuscitation (CPR). One of the crew members contacted the electrical utility office by truck radio and requested an ambulance. The emergency medical service arrived within 10 minutes and performed advanced cardiac life support (ACLS) procedures on the victim. The victim was transported to the local hospital where he was pronounced dead on arrival.
The incident was immediately investigated by electrical utility engineers, employer engineers, and linemen. The only other electrical attachment to the primary wire between the incident site and the main switch cabinet is a bank of two 25-kilovolt ampere pad-mounted transformers that served an emergency battery powered generator for the water pumps. If the power from the electrical utility’s line to the water pumps is interrupted, a switch automatically transfers the electrical load of the pumps to the battery-operated generator.
Tests on the automatic transfer switch showed it to be in proper working condition. The designer of the transfer system (i.e., the automatic transfer switch and the battery-operated generator) was summoned to the site to explain the mechanics of the system. The designer stated that if the transfer switch was operated manually after the generator was activated (i.e., transferring the load from the generator back to the electrical utility’s primary line) current would feed through the two transformers and automatic transfer switch to the electrical utility’s primary line. By using a voltmeter at the incident site it was determined that 4500 volts appeared on the primary line when the automatic transfer switch was operated in this manner.
Electrical utility engineers, employer engineers, and the system designer agreed that at some point after the battery-powered generator had been activated, the automatic transfer switch had been operated manually, allowing current to appear on the primary wire, causing the electrocution of the victim.
Cause of Death
The medical examiner listed electrocution as the cause of death.
Recommendations/Discussion
Recommendation #1: Employers should stress the importance of established safe work procedures to all workers.
Discussion: The victim, considered by the employer to be the most experienced underground crew leader in the company, had recently received training in the proper techniques and procedures for grounding underground power systems. He had discussed grounding procedures necessary for the task to be performed with the district supervisor and the safety officer on the day of the incident. Still, he did not ground the primary line at the main switch cabinet or the ends of the primary line at the incident site. Employers must ensure that all workers understand the importance of always following established safe work procedures.
Recommendation #2: Prior to any work being performed on an electrical system, all involved workers should be familiar with the operation of all components of that electrical system.
Discussion: In this incident it appears that the victim was not aware of the existence of the back-up generator; therefore, he was not aware that current could feed back through the transformers to the primary line even with the fuse and fuse holder removed from the main switch cabinet. Before beginning work on any electrical system, all persons involved in working on that electrical system should be made aware of the function of all components of the systems. Workers should be made aware of any hazards that might be created by the functions of these components before any work is performed on the electrical system.
This is especially important when working on underground systems because the lines or the direction of current flow cannot be visibly traced. The victim thought he had de-energized the primary line at the beginning of the job. Yet, when the crew members cut the cable an are occurred. This illustrates the fact that the victim was not familiar with all components of the system. If the victim had been aware of the possibility of the feedback of energy, he may have placed the required grounds on the primary line and placed a danger tag on the automatic transfer switch. These measures might have prevented this fatality.
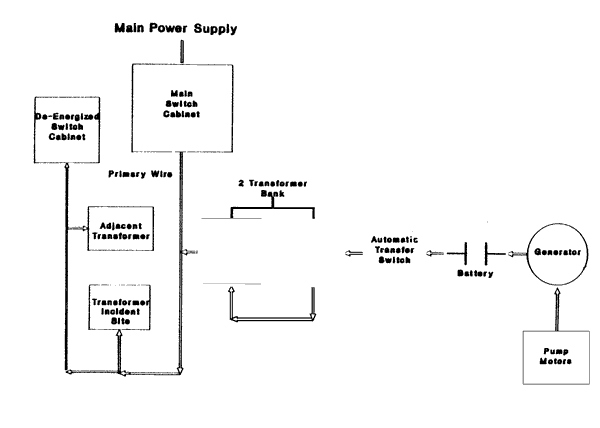
Figure.