
Fatal Accident Summary Report: Die Cast Operator Pinned by Robot
FACE 8420
INTRODUCTION
The National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR), is currently conducting the Fatal Accident Circumstances and Epidemiology (FACE) Study. By scientifically collecting data from a sample of similar fatal accidents, this study will identify and rank factors which increase the risk of fatal injury for selected employees.
On July 21, 1984 a 34 year old die cast operator with 15 years experience went into cardiopulmonary arrest after being pinned between the right rear end of a hydraulic robot and a safety pole. Rescue efforts included unpinning the worker, administering CPR, and transporting him to the emergency room of a nearby hospital. Five days later, he was pronounced dead as a result of cerebral necrosis. The attending medical examiner then notified the U.S. Consumer Product Safety Commission (CPSC) through their Medical Examiner and Coroner Alert Project (MECAP).
CONTACTS/ACTIVITIES
Subsequent to receiving notification from CPSC and cooperation from the employer, DSR sent a research team, consisting of an epidemiologist, safety engineer, and mechanical engineer, to conduct a field evaluation on August 23-24, 1984. An opening conference was held with the company’s Director of Manufacturing who provided background information about the company’s history, production, safety and training programs, injury statistics, and use of robotics. A site survey included visual observation and documentation of both the accident site and another automated die cast system while the robots were operating. Documentation of these work sites included 35mm slides and videotapes. During the site survey, interviews were held with the Director of Manufacturing and several operators in order to better understand the events surrounding the accident and the daily activities performed by operators. Other interviews were held with the worker who first found the victim, the foreman who was on duty the day the accident occurred, the president of the union local, the emergency medical squad, the fire department rescue squad, and the city dispatcher.
SCENARIO OF EVENTS
The employer of the victim is a die cast company with approximately 280 employees (including 66 die cast operators) and 24 die cast machines. Within the last two years, two of these machines had been automated and two more robots have been purchased but not placed into production at the time of the accident. The company works three shifts and operates 24 hours a day. Recently, the employees had been working six days (and occasionally seven days) a week.
On July 21, 1984, the die cast operator was working with an automated die cast system that utilized a Unimate Robot. This robot was programmed to extract the casting from-the die-cast machine, dip it into a quench tank and then insert it into an automatic trim press (see figure 1). The robot is programmed to perform the entire cycle in 27 steps which take approximately one minute. The safeguard present included a safety rail with interlock gate..
At approximately 1:00 PM, the victim entered the working area of the robot by either climbing over/through the safety rail or by walking through one of the unguarded gaps between the safety rail and related die-casting equipment. There was a 32 inch wide opening between the interlocking gate and the die-casting machine. There was also a 19 inch wide gap between the other end of the fence and the automatic trim press. His reason for entering the robot work envelope is uncertain. Several workers believed that since he had an air gun with him, he may have been trying to clean up ‘flash’ and “scrap metal- that had accumulated on the floor. The air hose was attached outside the work envelope but was sufficiently long to allow the operator to clean up the floor anywhere inside the envelope. Fellow workers also stated that they had seen the die-cast operator inside the work envelope on previous occasions with the robot up and running. The die-cast operator had been trained against this prohibited activity at the manufacturer’s training course on the robot. He had recently attended the course from June 25, 1984 to July 1, 1984.
The victim was discovered when a fellow employee, who worked at an adjacent die-cast work station heard an air hose steadily hissing. The accident site could not be seen from the neighboring work station but the fellow employee stated that he heard this continual hissing noise for 10 to 15-minutes. The neighboring employee stopped working and went to the next work station to investigate the hissing noise. He discovered the victim pinned between the right rear of the robot and a safety pole in a slumped but upright position (see Figure 2). The robot stalled when it contacted the man’s body and continued to apply pressure on the chest area. The employee then ran to get help from the foreman.
When the Director of Manufacturing arrived, he stated that fellow workers of the victim were struggling with the robot’s controller, a hand-held teach pendant which is used to program the robot. After giving up on this first robot controller, a second teach pendant was retrieved from another robot.’ The Director of Manufacturing finally unpinned the victim using the second hand-held robot controller and began administering CPR. The Fire Department arrived approximately one minute later. The Emergency Medical Service arrived approximately two minutes after the Fire Department and proceeded to transport the victim to the local hospital. The victim died five days later in the hospital. The next-of-kin refused to permit an autopsy; consequently, the complete pathology of the injuries is unknown. However, physical signs of any crushing injury were absent and x-rays of bones and internal organs were negative.
Subsequent to the accident, the employer installed a cyclone fence which covered the gaps and made unauthorized entry impossible.
CONCLUSIONS/RECOMMENDATIONS
At the time of the accident, the victim was an experienced die cast operator who received both- classroom training and on-the-job instruction on robotic safety. He had been both previously observed inside the envelope while the robot was running and verbally warned against this practice by fellow workers. The major factor contributing to this fatal accident may have been the behavior of the victim.
The evaluation of this fatal incident allows general recommendations to be made which are applicable to all establishments and workers who use or anticipate using robots. These recommendations pertain to three categories: ergonomic design, training, and supervision.
Ergonomic Design: 1. Safety fences with interlocking gates rather than rails should be used to fence off active robots. The purpose of the fence is to prevent unauthorized entry into the range of the robot’s moving parts.
2. Free-standing steel posts,-designed to restrict the movement of the robot’s arm in case a ‘loss of control’ is experienced, may provide man-sized pinch points where an unsuspecting worker could become trapped.
Training: ‘Extensive training should be provided for employees who will be programming,. operating or maintaining robots. This training should be safety-oriented as well at instructing employees in the methods of programming, starting up and stopping the robot. Newly trained employees may require close supervision until they adjust to the robot. Specific aspects of any training program should include/stress the following points:
1. Operators should never be in the work envelope while the robot is operational.
2. Because programming must be done inside the work envelope while the robot is operational, programmers should operate the robot at a slow safe speed be made aware of all the possible pinch points where his body or extremities could be trapped.
3. Training is not only needed for the inexperienced workers but refresher courses should be provided for experienced robot programmers and operators as well. The refresher courses will allow the experienced workers to remain up to date with new technology advancements and to reveal any problems or hazards that they might have experienced.
4. During programming, the robot should be stopped at each intermediate step and all possible pinch points should be identified and eliminated if possible. Possible pinch points should be considered on all sides of the robot.
5. During the safety and training course the following statements should be emphasized. ‘If the robot is stopped, don’t assume that it will remain stopped’, and ‘If a robot is repeating a motion, don’t assume that it will continue to repeat only that motion.’
Supervision: 1. Strict enforcement of a set of clearly written safety rules that reflect the company’s own safety program is essential to ensure the protection of the worker. Disciplinary action should be taken against anyone who enters the work envelope without first putting the robot on hold or in a ‘power down’ .condition.
2. Supervisors should be cognizant of the fact that operators experienced at automated tasks may be become bored, overconfident, or lose concern for safety. These conditions may-increase the worker’s risk of injury.
The assistance of the company employing the victim was exceptional and is greatly appreciated.
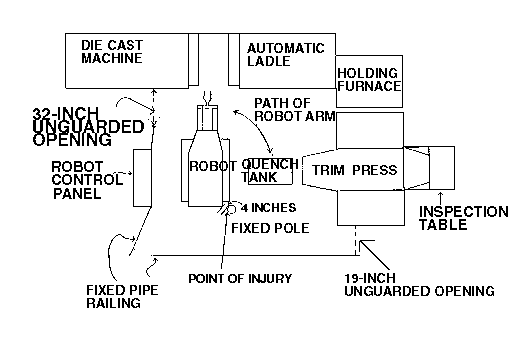
Figure 1. Diagram of Accident Site
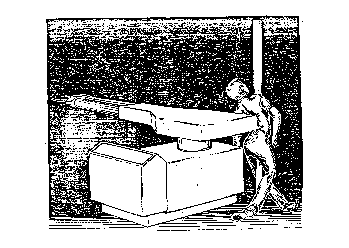
Figure 2. Artist’s Rendition of Body Position While Pinned