
Hispanic Sawmill Worker Dies Inside Storage Silo After Being Engulfed In Sawdust - North Carolina
NIOSH In-house FACE Report 2004-09
May 19, 2005
Summary
On May 17, 2004, a 36-year-old Hispanic laborer (the victim) died after he entered a sawdust storage silo to unclog a sweep auger advance mechanism and became engulfed in sawdust. Several minutes after the victim entered the silo, a Hispanic coworker working nearby heard a noise from the silo which prompted him to call out to the victim. When he heard no response, he and several Hispanic co-workers began looking for the victim. After approximately 20 minutes of digging through the collapsed sawdust, they found him. Coworkers ran to several locations trying to report the incident and get help. They notified a company senior official who then called 911. Emergency Medical Services (EMS) responded within approximately 30-35 minutes of the presumed time of engulfment and attempted resuscitation. They transported the victim by ambulance to a local hospital where he was pronounced dead by the emergency room physician.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
- ensure that equipment is inspected daily and all defective equipment is removed from service until needed repairs have been made
- consider retrofitting silos and similar storage facilities with mechanical leveling/raking devices or other means to minimize the need for workers to enter
- develop, implement, and enforce a comprehensive written safety and training program for all workers, including requirements for work in permit-required confined spaces, such as silos
- train workers in hazard recognition and safe work practices for all tasks to which they are assigned or allowed to perform, including those pertaining to work in permit-required confined spaces. The use of the workers’ primary language(s) and careful consideration of literacy levels will maximize worker comprehension of these subjects.
- post warning signs at entrances to permit-required confined spaces, such as silos, warning of immediate danger and safety requirements for entry in a language(s) that all workers can understand.
Introduction
On May 17, 2004, a 36-year-old Hispanic laborer (the victim) entered a sawdust storage silo through an opening under the silo floor to unclog a sweep auger advance mechanism. As he worked, sawdust, piled as high as 30 feet up the wall of the silo, collapsed and engulfed him. On August 12, 2004, the North Carolina Occupational Safety and Health (NCOSH) office notified the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) of the incident. On August 19, 2004, a DSR safety and occupational health team conducted an investigation of the incident. The incident was reviewed with the NCOSH compliance officers who had conducted an incident investigation on the day of the incident, and a site visit was arranged. One of the company’s senior officials and their environmental health and safety (EHS) manager accompanied DSR investigators to the incident scene where an inspection was conducted and photographs were taken. Investigators reviewed the sheriff’s report and obtained the cause of death from the medical examiner’s office.
The employer purchased the sawmill in 1986 and employed 142 workers. Approximately half of these workers were Hispanic. The victim was Hispanic and had been working at the facility for more than a year. He spoke primarily Spanish, but reportedly was able to understand basic work instructions given in English. Reportedly, supervisors spoke English but were able to give basic work instructions in both Spanish and English. Three weeks prior to the incident, the company had hired an experienced EHS manager, a position that had not been filled for nearly 4 years. According to the NCOSH compliance officer, the company had a general safety program that was deficient in several areas. The confined space and hazardous energy programs in place at the time of the incident were not adequate for this facility. The confined space program consisted of a video in English entitled “7-Minute Safety Trainer Program on Employees’ Roles in Confined Spaces.” The video was sent home with some of the employees to be watched at home. There was no documentation indicating that the victim, or a coworker removing sawdust on the day of the incident, had received training in safe work practices when working in or around confined spaces or around hazardous energy. The newly hired EHS manager was developing more comprehensive confined space and hazardous energy programs, but these had not been completed and implemented. This was the employer’s first workplace fatality.
Back to Top
Investigation
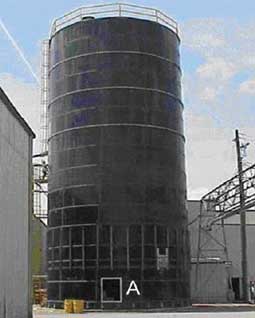
The incident took place at a sawmill that produced over 35 million board-feet of saw lumber per year. On site were three silos that were used to store sawdust, a by-product of lumber processing. Two of these silos, including the one involved in the incident, were flat-bottomed silos (photo 1). They had been purchased used at an auction, and were installed approximately one year prior to the incident. The third silo was an older hopper-bottomed design and had been manufactured by a different manufacturer (photo 2).
The silos received sawdust from the mill through a blower system. The sawdust was stored there until it was needed to fuel boilers. Whenever the local electric utility was unable to meet the mill’s energy needs, sawdust would be moved from the storage silos to the boilers using a system of augers. When sawdust was burned to heat water in boilers, steam heat was generated and converted to electricity on site to run the mill.
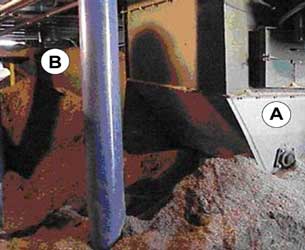
According to the company’s senior official and the company’s EHS manager who accompanied DSR investigators to the incident site, the sweep auger system in the flat-bottomed silos had clogged frequently since the time it was installed, and required unclogging approximately every two weeks during the periods it was activated. The victim was working inside one of these silos, which measure 30 feet in diameter, 60 feet in height and have flat, level floors, when he became engulfed in sawdust. A three-armed rotating sweep-auger installed on the silo floor was used to funnel the stored sawdust through an opening in the middle of the silo floor. The sawdust would then fall down to another auger called a transfer unloader located below the silo floor in the machine room (photos 3 & 4). The transfer unloader auger would then funnel the sawdust through a series of pipes to the boilers (photo 5). The machine room contained the power equipment to operate the augers and serves as a storage site for other pieces of equipment.
The company’s written procedure for manually unclogging the sweep auger advance mechanism (reproduced below verbatim in its entirety) reads as follows:
Clean out Procedures for the Silos
- Remove 3 12 x 24” access doors.
- Chip away card board at the access door.
- Take poles and rakes and chip away at the saw dust. (Photo 6)
- Repeat step #3 until saw dust is below the first ring level before entering into upper level of silo.
- Lockout disconnect and finish cleaning out silo from inside.
- Repair and test.
The written procedure above implies that the workers were to remain positioned inside the auger machinery room, not inside the silo, until sawdust was “raked down” to below the predetermined depth (“below the first ring”). No instructions were available in Spanish.
On the day of the incident, sawdust in the storage silo was to be removed in order to unclog the sweep auger located on the silo floor. One Hispanic laborer entered the silo from the machine room directly below the silo floor through the access opening (photos 7 & 8), but quickly exited after determining that the conditions were unsafe inside the silo due to the tall mounds of sawdust against the silo walls. According to another Hispanic laborer, the victim entered the silo alone a short time later to remove sawdust to clear the sweep auger. A coworker reported that the victim had been warned previously by at least two coworkers in both Spanish and English about the unsafe conditions. As the victim worked, sawdust piled as high as 30 feet up the wall of the silo collapsed and engulfed him not long after he entered the silo. Several minutes passed before his absence was noted by coworkers who then began calling out to the victim. When there was no response, one coworker climbed to the top of the silo in order to take a look from above. He did not see the victim. By this time, other coworkers entered the silo and, manually digging and using poles for probing, searched for the victim in the collapsed sawdust.
Coworkers found the unresponsive victim after approximately twenty minutes and tried to remove the sawdust from his mouth. Coworkers ran to several locations trying to report the incident and get help. A company senior official was notified of the incident and called 911. However, the call for 911 was not placed until the victim was already found. Emergency Medical Services (EMS) responded within 30-35 minutes of the presumed time of engulfment and attempted resuscitation. EMS transported the victim by ambulance to a local hospital where he was pronounced dead by the emergency room physician.
After the incident, the flat-bottomed silos were shut down. The hopper-bottomed silo had no history of jamming and remained in operation.
Back to Top
Cause of Death
The medical examiner’s report indicated the cause of death was asphyxiation.
Recommendations/Discussion
Recommendation #1: Employers should ensure that equipment is inspected daily and all defective equipment is removed from service until needed repairs have been made.
Discussion: Employers should designate a supervisor to be responsible for daily preshift equipment checks and for verifying that any problems identified are corrected. Although equipment may also be inspected by other workers, for example, the workers assigned to begin the sawdust transfer to the boiler, the supervisor must be responsible for ensuring that inspections are performed daily, that necessary repairs are made, that scheduled maintenance is performed, and that records of all inspections are maintained. Equipment not operating properly should be removed from service until repairs are made. All sources of hazardous energy should be locked out before any repairs are begun. Regulations regarding the control of hazardous energy (lockout/tagout) must be followed and are covered under the OSHA standards.1
Recommendation #2: Employers and manufacturers should consider retrofitting silos and other similar storage facilities with mechanical leveling/raking devices or other means to minimize the need for workers to enter.
Discussion: Company owners should consult with silo manufacturers to determine which measures would improve the flow of the materials. Silos, bins, and hoppers where loose materials such as waste sawdust are stored, handled, or transferred could be equipped with mechanical leveling/raking devices or other means for remotely handling materials. These devices, such as mechanical agitators or vibrators, could minimize or eliminate the need for workers to enter such storage facilities.
An expert in engulfment and silo operation was contacted and told DSR investigators that materials such as sawdust are more prone to “bridging” than other granular material.2 Bridging occurs when sawdust in the silo forms a thick, hard crust on the upper portions including the surface. As sawdust is removed from below, a hollow cavity is formed and some sawdust remains suspended above this cavity. This could explain the reason for the sawdust piling up and clinging to the interior walls of the silo. With the use of hopper-bottomed silos or the addition of mechanical devices such as bin vibrators, sawdust buildup would be limited, and workers would not need to enter the silo. In this way, exposure to mechanical and engulfment hazards inside the silo could be avoided.
Recommendation #3: Employers should develop, implement, and enforce a comprehensive written safety program for all workers, including requirements for work in permit-required confined spaces, such as silos.
Discussion: Although employees had received some on-the-job training, they had not received adequate training based on OSHA requirements for a permit-required confined space program. The Occupational Safety and Health Administration standards define a permit-required confined space as a confined space that has one or more of the following characteristics:
- Contains or has a potential to contain a hazardous atmosphere;
- Contains a material that has the potential for engulfing an entrant;
- Has an internal configuration such that an entrant could be trapped or asphyxiated by inwardly converging walls or by a floor which slopes downward and tapers to a smaller cross-section; or
- Contains any other recognized serious safety or health hazard.3
A permit-required confined space program has detailed requirements including, but no limited to:
- implementation of measures necessary to prevent unauthorized entry;
- identification and evaluation of hazards of permit spaces before entering;
- development and implementation of the means, procedures, and practices necessary for safe permit space entry operations;
- providing of equipment for testing, monitor, ventilating, communication, lighting, etc.;
- evaluation of permit spaces conditions when entry operations are conducted.For a complete list of requirements for written programs, see 29 CFR 1910.146 and OSHA Publication 3138.3, 4
The victim’s employer had procedures in place for removing sawdust from inside the silo which allowed workers to enter the silo, a permit-required confined space, without following the strict safety procedures required by OSHA to protect workers in these types of permit spaces.
Employers should identify all permit-required confined spaces in their facilities and compare their safety procedures against the minimum safety requirements found in OSHA standard 29 CFR 1910.146 and make any changes needed to ensure that their programs meet all of these requirements. All employees who work in or around permit-required confined spaces should be aware of potential hazards (e.g., engulfment; mechanical, electrical or other injury hazards; oxygen deficiency; and presence of toxic or explosive gases) possible emergencies, and specific procedures to be followed prior to working in a permit-required confined space. These procedures should include, but not be limited to:
- ensuring that the atmosphere is free of contaminants and contains a safe level of oxygen
- identifying and controlling of the hazards associated with unstable surfaces
- identifying and controlling other hazards, such as mechanical or electrical hazards
- training employees in permit-required confined space entry, testing, and the use of personal protective equipment, safety harnesses, respirators, clothing, etc.
- stationing (a) stand-by person(s) outside the space for communication and visual monitoring
- providing for emergency rescue procedures.3
Even though there were no dangerous air contaminants in the permit-required confined space involved in this incident, entry into a permit-required confined space should not be attempted until atmospheric testing of the confined space ensures that the atmosphere is safe. This testing requirement applies to all permit-required confined spaces. Testing must be done by a qualified person prior to entry. Employers are required to follow OSHA standards for all permit-required confined space entries.
Additional recommendations regarding safe work practices in confined spaces can be found in the NIOSH Publication No. 80-106, Criteria for a Recommended Standard: Working in Confined Spaces;5 NIOSH Alert Publication 86-110, Request for Assistance in Preventing Occupational Fatalities in Confined Spaces;6 NIOSH Publication No. 87-113 A Guide to Safety in Confined Spaces;7 and NIOSH Publication No. 94-103, Worker Deaths in Confined Spaces: A Summary of NIOSH Surveillance and Investigative Findings.8 These publications can be useful in developing confined space safety programs and in training workers as they define hazards found in confined spaces and provide recommendations for ventilation, communication, entry and rescue, posted warning sings, required safety equipment, clothing, etc. These NIOSH publications are available through the NIOSH web site at https://www.cdc.gov/niosh/topics/confinedspace/ or by calling 1-800-356-4674. (Link Updated 3/14/2013)
Despite the hazards involved in this operation, no pre-planning for any type of rescue operation had been made. According to 29 CFR 1910.146 (d)(9), employers are required to “develop and implement procedures for summoning rescue and emergency services, for rescuing entrants from permit spaces, for providing necessary emergency services to rescued employees, and for preventing unauthorized personnel from attempting a rescue.” Consideration should be given to inviting local rescue and emergency services to survey the work site to evaluate and record locations of potentially hazardous areas such as confined spaces. Requirements to develop and implement procedures for summoning rescue/emergency services and for rescuing entrants from permit spaces are found in 29 CFR 1910.146 (k).3
Recommendation #4: Employers should train workers in hazard recognition and safe work practices for all tasks to which they are assigned or allowed to perform, including those pertaining to work in permit-required confined spaces. The use of the workers’ primary language(s) and careful consideration of literacy levels will maximize worker comprehension of these subjects.
Discussion: One of the workers had some training in confined spaces and had warned the victim not to enter the silo. Another worker stated that he had not received any training in confined spaces. At the time of the incident, the newly hired EHS manager was in the process of updating the company’s safety program. Employers must ensure that training is done in accordance with current OSHA standards and with careful consideration for the workers’ primary language(s) and literacy levels. Re-training is recommended at regular intervals. If workers cannot read posted warning signs, they should be given verbal instructions about what each sign means and what procedures they are to follow when working in posted areas. An interpreter should be used if workers require assistance in understanding safety training. The use of posted warning signs does not preclude the need for developing and implementing a confined space entry program including proper and effective training.
For further information on permit-required confined space programs, employers can visit the OSHA web site (https://www.osha.govexternal icon) or call an area OSHA office for assistance to ensure that safety programs meet required safety standards.
Recommendation#5: Employers should post warning signs at entrances to permit-required confined spaces, such as silos, warning of immediate danger and safety requirements for entry in a language(s) that all workers can understand.
Discussion: Employers should post warning signs in the primary languages used by their workforce and post them at the entrance to any permit-required confined space at the workplace. Employers should refer to ANSI standards Z53.19 and Z535.210, and OSHA standards 1910.14511 for guidance on requirements for safety signs. The following examples are warning signs printed in both English and Spanish:

|
When employers post signs at entrances to permit-required confined spaces warning of immediate danger and that special requirements are necessary for entry in the primary language used by their employees, they increase the likelihood that workers will be able to comprehend the procedures they are to follow and be alert to possible danger. The meaning of these signs and their location throughout the facility should be incorporated into the company’s permit-required confined space training program. The use of posted warning signs does not preclude the need for developing and implementing a confined space entry program including proper and effective training.
Back to Top
References
- Code of Federal Regulations [2004]. 29 CFR 1910.147. The control of hazardous energy (lockout/tagout). Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- D. M. Kingman (personal communication. September 27, 2004).
- Code of Federal Regulations [2004]. 29 CFR 1910.146. Permit-required confined spaces. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
- OSHA [2004]. Permit-required confined spaces. Occupational Safety and Health Administration (OSHA) Publication No. 3138-01R 2004. Accessed on April 29, 2005 https://www.osha.gov/Publications/osha3138.pdfpdf iconexternal icon.
- NIOSH [1979]. Criteria for a recommended standard: Working in Confined Spaces. Cincinnati, OH: U.S. Department of Health, Education, and Welfare, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHEW (NIOSH) Publication No. 80-106.
- NIOSH [1986]. NIOSH Alert: Request for assistance in preventing occupational fatalities in confined spaces. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 86-110.
- NIOSH [1987]. A guide to safety in confined paces. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 87-113.
- NIOSH [1994]. Worker deaths in confined spaces: A summary of NIOSH surveillance and investigative findings. Cincinnati, OH: U.S. Department of Health and Human Services, Public Health Service, Centers for Disease Control and Prevention, National Institute for Occupational Safety and Health, DHHS (NIOSH) Publication No. 94-103.
- ANSI [1979]. American National Standard: Safety color coding for marking physical hazards. New York, NY: American National Standards Institute, Inc. ANSI Z53.1-1979.
- ANSI [2002]. American National Standard: Environmental and facility safety signs. New York, NY: American National Standards Institute, Inc. ANSI Z535.2-2002.
- Code of Federal Regulations [2004]. 29 CFR 1910.145. Specifications for accident prevention signs and tags. Washington DC: U.S. Government Printing Office, Office of the Federal Register.
Back to Top
Investigator Information
This investigation was conducted by Gerard deGuzman, M.D., Occupational Medicine Resident at West Virginia University School of Medicine assigned to NIOSH, Division of Safety Research, Special Studies Team and Doloris N. Higgins, Safety and Occupational Health Specialist, Fatality Investigations Team, Surveillance and Field Investigations Branch, Division of Safety Research. Douglas M. Kingman, Ph.D., from Illinois State University provided additional expertise in engulfment and silo design and operation.
Photographs






In-house Reports