
Seventeen-Year-Old Bagger at Retail Grocery Store Suffers Amputation While Operating a Meat Grinder - Pennsylvania
NIOSH In-house FACE Report 2001-05
Summary

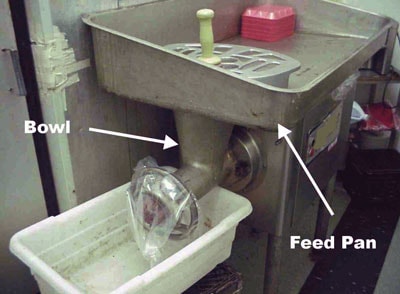
On September 12, 2000, a 17-year-old bagger (the victim) at a retail grocery store suffered amputation of the right arm as a result of being caught in an operating meat grinder. The victim had been working in the family-owned store after school hours. On the day of the incident, a customer asked him to get some ground beef. There was none available, and no one working in the meat room. The youth decided to prepare the ground beef himself and went to the meat room to process the beef through the meat grinder. While he was operating the grinder, some of the meat became stuck in the meat grinder bowl. The youth removed the feed pan, reached with his right hand into the bowl and pushed the meat down into the grinder’s worm.1 When meat fed from the bowl, the worm caught his hand and fed it into the grinder’s barrel, amputating his hand and part of his lower right arm. Coworkers called 911 and emergency medical personnel responded within 5 to 10 minutes.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should
- ensure that workers are trained to recognize the hazard of accessing the internal components of operating or energized machinery
- prohibit workers under the age of 18 from operating power-driven meat-processing machines by implementing youth-appropriate hazardous-energy-control procedures
Additionally, manufacturers of power-driven meat-processing equipment should
- consider design modifications or additions to provide redundant protection against the inadvertent release of hazardous energy through contact with operating machine components.
Introduction
On September 12, 2000, a 17-year-old bagger (the victim) at a retail grocery store suffered amputation of the right arm as a result of being caught in a meat grinder while operating the machine (Photo 1). On January 10, 2001, the U.S. Department of Labor, Wage and Hour Division notified NIOSH’s Division of Safety Research (DSR) of the occurrence. On March 5, 2001, a DSR safety engineer met with the Wage and Hour investigator, reviewed the case file, and discussed the case. On March 6, 2001, the safety engineer visited the grocery store, examined the meat grinder, and interviewed the meat department manager and the company’s bookkeeper. Photographs and measurements of the meat grinder were taken. On March 6, 2001, the safety engineer met with the U.S. Occupational Safety and Health Administration (OSHA) compliance officer assigned to the case and discussed the case.
The employer was a family-owned neighborhood grocery store located in a large city. The store had opened for business in 1992 and employed 10 adult workers. The victim was the only employee under the age of 18. The employer had no written safety and training policy. Three days before the incident the youth had begun working after school. He was assigned to bag groceries at the front of the store and had been given on-the-job training for this task. Because he was not assigned to operate the meat grinder or other meat processing machines, he had not been instructed about their operation or potential hazards. However, since working at the store, he had socialized with the meat-room workers during breaks and idle periods, and it is likely that he had observed adult coworkers operating the meat grinder.
This was the first injury that had occurred at the store.
There were no eyewitnesses to the incident, and when interviewed by the Wage and Hour investigator, the youth could not remember the details of the incident. For this reason, the exact sequence of events is not known. However, during the site visit on March 6, 2001, the meat grinder was examined by the safety engineer, assisted by the meat department manager. Measurements and tests were conducted in an effort to identify a likely sequence of events to explain the manner of energy transfer between the meat grinder and the victim.
Back to Top
Investigation
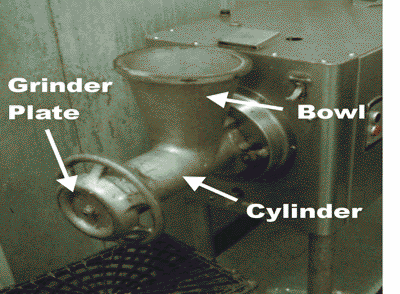
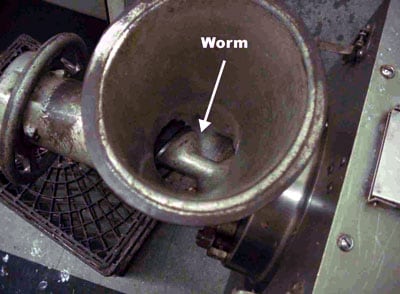
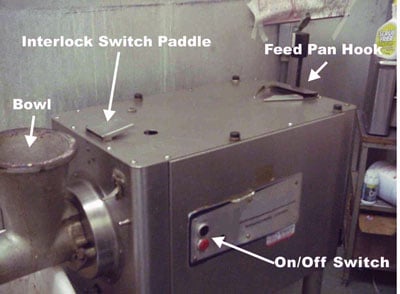
The meat grinder involved in this incident had been previously owned and was purchased by the employer when the store opened. The age of the machine was not known. The machine was powered by a 5-horsepower electric motor that drove a worm through a geared transmission. The motor and transmission were enclosed in an equipment cabinet with the grinder assembly (a cylinder and bowl housing, a grinder plate and locking ring, and the worm) mounted on one end. The worm, mounted under the bowl, rotates inside the grinder cylinder (Photo 2a and Photo 2b). Meat fed manually into the bowl from the feed pan drops onto the rotating worm, which forces it through the cylinder, past a set of four knife blades mounted on the end of the worm, and through the grinder plate at the end of the cylinder. A stuffer is supplied with the machine to assist in feeding the meat down into the bowl.
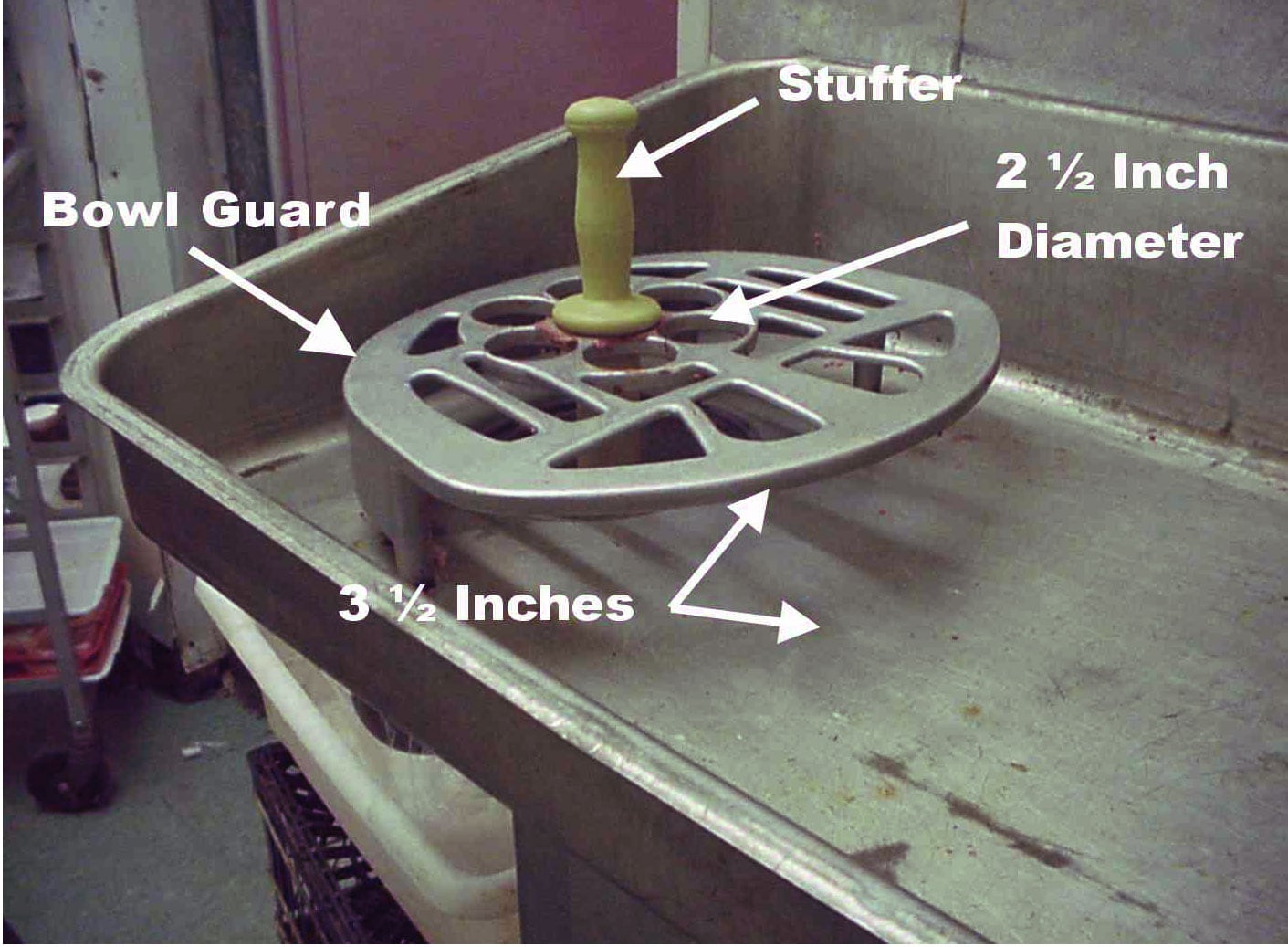
The machine is equipped with several safety features designed to protect an operator from becoming caught by the worm. The feed pan is equipped with a permanently attached aluminum bowl guard covering the feed pan bowl opening (Photo 3). There is a safety interlock switch mounted between the top of the equipment cabinet and the bottom of the feed pan that interrupts power to the motor when the pan is removed (Photo 4). The motor cannot be restarted until the feed pan is replaced and the interlock switch paddle depressed. The feed pan is secured to the top of the equipment cabinet by a hook at the end of the cabinet opposite the grinder assembly and two toggle latches just above the grinder assembly. A push-button-operated start/stop switch is located on the side of the equipment cabinet. This switch type and its location minimize the likelihood of inadvertent startup by persons leaning or bumping against it.
On the day of the incident, the victim had been at work for several hours after school dismissal. He had gone about his assigned duties as a bagger. Shortly before 4:30 p.m., he was walking from the front of the store to the rear, when a customer stopped him and requested assistance in obtaining some ground beef. To accommodate the customer’s request, the youth went to the meat room which was unoccupied because the meat department manager had left the store to deliver groceries to a customer. The store’s supply of ground beef had been depleted so the youth started the meat grinder to process more. While he was grinding the meat, some of it stuck in the feed bowl, just above the worm. As previously stated, the exact sequence of events after this point could not be established. However, an evaluation of the machine’s physical and operational characteristics indicate that the youth removed the feed pan and pushed the stuck meat down into the bowl with his hand. At this point, one of the following occurred (see Appendix):
- The youth may have shut down the machine before raising the feed pan, but did not wait for the worm to come to a complete stop before inserting his hand. The worm coasts to a complete stop 6 to 7 seconds after the machine is shut down and retains enough energy to feed material into the cylinder while coasting to a stop.
- The interlock switch may have shut down the machine as the feed pan was raised but the youth inserted his hand before the worm was completely stopped.
- The youth may not have shut the machine down and the interlock switch may have malfunctioned, allowing the machine to operate as the youth inserted his hand.
When his fingers went below the bottom of the bowl his hand was caught by the worm and fed into the cylinder, amputating his arm below the elbow near his wrist. Coworkers heard his cries for help and called 911. EMS responded within 5 to 10 minutes and the youth was transported to a local trauma center.
Back to Top
Injury
As a result of the incident, the victim suffered amputation of the lower right arm.
Recommendations/Discussion
Recommendation #1: Employers should ensure that workers are trained to recognize the hazard of accessing the internal components of operating or energized machinery.
Discussion: Because the youth was not assigned to operate the machine or perform work tasks in the meat room, he had not received instruction in the hazards of operating the meat grinder. His assigned task was to bag groceries at the front of the market. However, he had socialized with the meat room employees during breaks and may have observed other workers grinding meat or disassembling the machine for cleaning at the end of the day. Further, the operation of the grinder is not complicated from the standpoint of starting and stopping the machine, feeding meat through the bowl guard, and collecting the ground meat as it is discharged from the grinder plate. In some respects, the machine is nothing more than a large kitchen appliance and the basic operating procedure is intuitive. However, what is not so apparent is the risk of being caught by the grinder worm if the worker reaches into the bowl while the machine components are still in motion. Even though workers may not be assigned to operate certain types of equipment, training them to recognize hazards associated with the equipment’s operation could further reduce their risk of injury from contact with the machine’s components.
Recommendation #2: Employers should prohibit workers under the age of 18 from operating power-driven meat-processing machines by implementing youth-appropriate hazardous-energy-control procedures.
Discussion: The Fair Labor Standards Act (FLSA) includes provisions to protect youth by prohibiting their employment under conditions that would be detrimental to their health or well-being. Because operating power-driven meat grinders has been found to be particularly hazardous, a minimum age of 18 has been established for workers who operate these machines. These employment standards are listed and explained in bulletin WH-1330, U.S. Department of Labor, Employment Standards Administration, Wage and Hour Division. [1] It should be noted that the victim had not been assigned to operate the meat grinder or the other power-driven meat processing machines in the store; his task was to bag groceries at the check-out, and if adult workers had been present, he may not have been motivated to operate the machine and the incident may not have occurred. To prohibit youth in similar situations from operating power-driven meat processing equipment, it may be necessary for employers to implement youth-specific hazardous-energy-control procedures. Procedures designed to isolate workers from contact with uncontrolled hazardous energy during repair, maintenance, or servicing of equipment are required by OSHA regulation 29 CFR 1910.147.[2] A similar hazardous energy control program specific to the needs of youth could include:
- Training workers to recognize tasks prohibited to workers under 18 years of age
- Posting signs on power-driven meat-processing equipment to notify workers that operation by persons under 18 years of age is prohibited.
- Disconnecting equipment from its power source when not in use or when it is unattended by adult workers
- Securing the equipment against unauthorized use
For example, the machine in this incident was connected to the power supply by a line cord and plug inserted into a wall receptacle. When not in use, the power could be disconnected, the line cord plug locked in a lockout/tagout box, and the key for the box kept in the custody of an adult worker (Photo 5).
Recommendation #3: Employers and manufacturers should consider design modifications or additions to provide redundant protection against the inadvertent release of hazardous energy through contact with operating machine components.
Discussion: The machine in this incident was equipped with several features that protect workers from the uncontrolled release of hazardous energy. The push button start/stop switch mounted on the side of the motor/transmission cabinet was unlikely to be inadvertently activated. The machine was equipped with a safety interlock switch mounted on the top of the motor/transmission cabinet so that the machine could not be started or would not continue to operate if the feed pan was removed. The feed pan was equipped with a permanently mounted bowl guard to prevent workers from reaching into the grinder bowl. However, as noted during the testing and examination of the machine, the grinder worm continued to turn for 6 to 7 seconds after the motor was deenergized and possessed enough energy to feed meat into the grinder cylinder (see Appendix). Redundant protection could be provided by equipping machines of this type with additional or redesigned interlock systems that would prevent removal of the feed pan until the grinder worm had come to a complete stop. This could be accomplished through the use of motion detectors or centrifugal switches.
Back to Top
References
- DOL [1991]. Child Labor Requirements in Nonagricultural Occupations Under the Fair Labor Standards Act, U. S. Department of Labor, Employment Standards Administration, Wage and Hour Division, WH-1330, revised September 1991.
- 29 CFR 1910.147 [1998]. The control of hazardous energy (lockout/tagout), Washington, DC: U.S. Government Printing Office, Office of Federal Register.
Investigator Information
This investigation was conducted by Paul H. Moore, Safety Engineer, NIOSH, Division of Safety Research, Surveillance and Field Investigation Branch, Fatality Assessment and Control Evaluation Team.
Back to Top
Appendix
Evaluation of the meat grinder. As previously stated, the event was unwitnessed and the youth was unable to remember the sequence and manner of energy transfer. Additionally it was not known if the machine and its safety features had been operating correctly at the time of incident. For these reasons, the operation of the machine and its safety features was evaluated during the site visit of March 6, 2001. A description of the testing and examination performed follows:
Machine guarding. The length of the stuffer from its support shoulder to the end was found to be 11¾ inches. The distance from the stuffer support on the bowl guard to the top of the worm flights was found to be 12½ inches. This 1¼-inch difference accounts for the tendency of the last piece of meat fed into the bowl to sometimes fail to feed into the worm.
The bowl guard is permanently mounted at a height of 3½ inches above the floor of the feed pan. The largest opening in the bowl guard surface was 2½ inches in diameter. It is unlikely that a worker’s hand and arm could be inserted through these holes.
The bowl guard is open on one side only to allow meat to be fed into the bowl. The distance from the open edge of the bowl guard to the bowl opening in the feed pan was about 6 inches. It is very unlikely that a worker could insert a hand and arm through the feed opening for a horizontal distance of 6 inches and then vertically for 12½ inches through the bowl to reach the worm flights.
Safety interlock switch. With the machine running, the feed pan was unlatched and raised up at the feed end. The pan was raised about 6 inches and the interlock failed to shut down the machine. The test was repeated and this time the interlock successfully shut down the machine. The test was performed 4 additional times with the interlock functioning correctly. It was thought that the malfunction of the first test was due to a sticking switch plunger or a sticking switch paddle. The feed pan was completely removed, the interlock switch paddle depressed by hand, and the machine was started. The safety engineer slowly released the switch paddle and the interlock shut down the machine. This test was repeated numerous times, releasing the paddle slowly and quickly. The switch continued to function correctly. In an effort to repeat the malfunction first encountered, hand pressure was exerted on the switch paddle from both sides and front to back while allowing it to raise. No tests were able to repeat the malfunction.
The feed pan was reassembled on the machine but left unlatched. The pan was positioned in several misaligned configurations in an effort to find a position that would provide a large enough opening between the pan and the bowl for access to the interior while still depressing the interlock switch paddle and allowing the machine to operate. No position could be found.
Operating characteristics, time-to-stop and stored energy. With the machine running, the motor was shut down by the push button switch and the time for the worm to come to a complete stop was observed at 6 to 7 seconds. After this was observed, it was decided to evaluate the potential for the coasting worm to inflict injury. The feed pan was removed, and with the interlock switch depressed by hand, the machine was started. A piece of beef, 1 x 2 x 10 inches long, was dropped into the bowl immediately after the stop button was pushed. The worm fed the meat completely into the grinder cylinder. The test was repeated, only this time the worm was allowed to coast for several seconds after the stop button was pushed before the meat was dropped into the bowl. Again, the meat was fed completely into the cylinder. The test was repeated for a third time except that the worm was allowed to coast even longer before the meat was dropped into the bowl. The meat was fed completely into the cylinder while the worm was observed to coast to a stop after only three revolutions.
Back to Top
Photographs
|
|
|
|
|

|
|
Photo 5. Typical Method of Locking Out Line Cord Plug
|
The FACE investigation project is the cornerstone of the overall NIOSH program to prevent occupational fatalities. The objectives for this effort include the investigation of occupational fatalities to assess and characterize the circumstances of these events in order to develop succinct descriptive and evaluative reports for distribution to occupational safety and health groups across the country. This work is being conducted by the FACE investigation team. It is expected that the reports alone will have a major impact by better defining the causal factors behind occupational fatalities, calling national attention to the problem, and providing insights into the prevention efforts that are needed. However, the program does not determine fault or place blame on companies or individual workers.