
Sanitation Worker Dies After Being Caught In Chiller At Poultry Processing Plant--South Carolina
FACE 9602
SUMMARY
A 37-year-old male sanitation worker (the victim) died as a result of crushing injuries he sustained after being caught in a poultry chiller at a poultry processing plant. The victim and four other sanitation workers were engaged in cleaning three chillers at the processing plant. The drive motors for the chillers had been de-energized but not locked out prior to commencement of cleaning activities. Two co-workers had been assigned to clean the #2 and #3 chiller while the victim and another co-worker had been assigned to clean the #1 chiller. While the victim was inside the #1 chiller and engaged in cleaning, a co-worker attempted to energize the drive motor to the #2 chiller paddles. Instead, he inadvertently activated the control switch for the #1 chiller paddles. The paddles for the #1 chiller began to rotate and pinned the victim between a paddle blade and the side of the chiller, crushing him. The plant manager heard the noise of the incident from his office and went to the chiller area. He directed co-workers to begin removal of the victim and notified 911. After the paddle wheel shaft was cut, the victim was removed and transported to a local emergency room where he died the following evening.
NIOSH investigators concluded that, to prevent similar occurrences, employers should:
- ensure that comprehensive hazardous energy control procedures, including proper lockout/tagout procedures are established and followed
- ensure that all components of new or modified equipment, including safety devices, are properly installed and functioning before implementing use
- ensure that hazard evaluations are performed before process and system modifications are implemented
- ensure that safety programs include procedures requiring workers to communicate potential hazards to safety managers.
INTRODUCTION
On September 16, 1995, a 37-year-old sanitation worker at a poultry processing plant (the victim), died after he was caught between the paddles and side of a poultry chiller during cleaning operations. On September 18, 1995, officials of the South Carolina Occupational Safety and Health Administration (SCOSHA) notified the Division of Safety Research (DSR) of the occurrence and requested technical assistance. On October 31, 1995, a DSR safety engineer reviewed the SCOSHA investigation file and conducted an investigation at the plant. While at the plant, the safety engineer interviewed the company’s regional safety coordinator and obtained photographs of the incident site.
The employer in this incident was a multi-state poultry producer established in 1982 which employed over 1300 workers. The incident occurred in a processing plant which operated two production and one sanitation shift (4 to 11 pm.) daily. The company employed a full-time regional safety coordinator who was based at the incident location. The company had written safety procedures including lockout/tagout requirements for cleaning and maintenance. The sanitation shift employed 38 workers. The victim was a probationary employee who had been working only 4 days at the incident plant. He was receiving on-the-job training from the lead man assigned to the chillers. This was the company’s first fatality.
INVESTIGATION
On the day of the incident, the victim, along with four co-workers, began work on the processing plant’s sanitation shift, at 4:00 p.m. Just before 5:40 p.m. the four workers were engaged in their normal procedures of cleaning the plant’s three chillers which cool cleaned chicken carcasses, to facilitate cutting them into parts before packaging. The chillers are refrigerated, open-topped, water-filled, cylindrical tanks approximately 5-feet in diameter and 36-feet long. During operation, chicken carcasses enter the chiller and float to the exit end where they are removed and discharged onto a conveyor by rotating scoops. Inside the chiller is a series of electrically driven paddle wheels which rotate at 5 rpm and agitate the refrigerated water. The paddle wheels are split into entrance and exit wheels, each having its own motor and control switch. The control panel had recently been relocated from the compressor room to the east wall of the chiller room (Figure). The relocation had been completed except for the installation of lockable covers over the individual control switches; covers had been back-ordered from the supplier.
On this day, two of the co-workers were assigned to clean chillers #2 and #3, while the victim and the lead man were assigned to the #1 chiller. During cleaning, the chiller motors were de-energized at the control panel; however, since the lockable switch covers had yet to be installed, the switches were not locked out according to the employer’s lockout/tagout policy. While the victim was cleaning inside the chiller, he was being observed by the co-worker as part of on-the-job training. Shortly before 5:40 p.m. as the victim was inside the #1 chiller, the worker assigned to clean the #2 chiller went to the chiller control panel, intending to energize the entrance paddle wheel in the #2 chiller. He reached up to activate the #2 chiller entrance paddle, but instead inadvertently activated the #1 chiller exit paddle. The #1 chiller paddle wheel began rotating and one blade struck the victim in the back and pinned him to the wall of the chiller. His co-worker immediately jumped up on the chiller and pulled the paddle off the victim while simultaneously yelling to cut the power to the chiller. He was able to momentarily pull the paddle off and tried to help the victim climb out. The victim however, could not move and the co-worker was unable to continue holding the paddle blade off of the victim. One co-worker de-energized the power but the victim remained caught between the paddle blade and the side of the chiller. While this was occurring, the plant manager heard the noise of the incident from inside his office and went to the chiller area. He directed the lead man to take the workers to the break room and directed the processing manager to call 911. He then directed other workers to begin cutting the paddle wheel drive shaft to enable the paddles to be moved off the victim. This work was still in progress when the emergency medical service (EMS) arrived 4 minutes after notification. The victim was removed from the chiller and transported to a local emergency room where he died the following evening at 8:20 p.m.
CAUSE OF DEATH
The cause of death was established as cardiovascular decompensation secondary to massive crushing injury of the upper thorax.
RECOMMENDATION/DISCUSSION
Recommendation # 1: Employers should ensure that comprehensive hazardous energy control procedures, including proper lockout/ tagout procedures, are established and followed.
Discussion: A lockout/tagout policy and procedure implemented by the employer gave sole lockout control to the employee who was exposed. However, the control system for the chillers had recently been modified by the relocation of the control panel to the east wall of the building near the chillers. This panel contained six clearly marked rotary switches, located side by side, which controlled the entrance and exit paddles for each chiller. The necessary parts to provide secure lockout for each switch had not been installed because the parts were on order. Because of this, it was not possible to follow the established lockout/tagout procedure requiring each sanitation worker to lock out and control the key for the individual chillers. The employer has since installed hinged lockable covers over each switch. These covers must be lifted to gain access to each switch and provide for individual lockout with separate keys for each worker cleaning the chillers. The employer has also revised the lockout/tagout procedure to include specific procedures for each machine in the plant.
Recommendation #2: Employers should ensure that all components of new or modified equipment, including safety devices, are properly installed and functioning before implementing use.
Discussion: Relocating the control panel had been implemented to remove it from the high noise area of the compressor room and to place it nearer to the chillers for communication purposes. However, safety enhancements due to the relocation were not realized when the system was used without the safety devices which were necessary to establish adherence to the employer’s lockout/tagout procedure. Revised systems should not be activated until all safety devices have been installed, or other measures are taken. In this incident, although the parts to provide individual lockout of each switch were not available, the control panel cover could have been fitted with a hasp and lock as a temporary measure until the needed parts were obtained.
Recommendation # 3: Employers should ensure that hazard evaluations are performed before process and system modifications are implemented.
Discussion: In this incident, both the chiller-control system and the cleaning process had been revised without involvement of the employer’s safety department or engineering department. The controls for the chillers had been located in a separate room from the chiller area; this room also contained compressors for the plant’s refrigeration units. The controls had been moved on September 9, 1995, to eliminate worker exposure to the noise of the compressors and improve worker communication between the control-panel location and the chillers. Additionally, the cleaning procedure for the chillers had been changed about 6 weeks prior to the incident, as a result of USDA inspections which observed oil film on the water in the chiller. The change involved the workers climbing inside the chillers to scrub them, as opposed to remaining outside and cleaning with high-pressure hoses. This appeared to eliminate the oil film; however, these changes in process and systems were not communicated to the plant safety personnel or the engineering department. Including safety managers in the decision-making process prior to implementing process and system changes would allow for safety evaluation to safeguard against the introduction of new hazards to the workplace.
Recommendation # 4: Employers should ensure that safety programs include procedures requiring workers to communicate hazards to safety managers.
Discussion: After the incident, it was learned that there had been two prior instances when a chiller paddle wheel had been inadvertently turned on while workers were inside. On each occasion, the worker was able to jump out of the chiller before being caught by the paddle blades. These near misses were part of the reason for moving the control panel to the same location as the chillers; however, this information was not communicated to the sanitation supervisor.
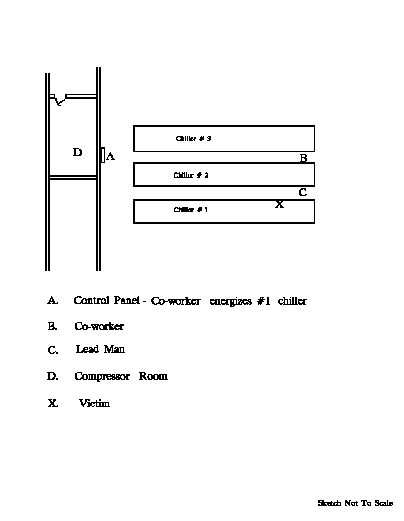
Figure.
Return to In-house FACE reports