
Shipping Department Employee Dies After Falling Into Floor Opening on Conveyor Line--Virginia
FACE 9515
SUMMARY
On July 12, 1995, a 37-year-old male loader/unloader (the victim) was fatally injured when he fell through a floor opening of a conveyor line at a furniture manufacturing company warehouse. The victim was transferring cardboard cartons containing furniture from one conveyor line to another prior to their being lowered through a floor opening from the third to the second floor of the warehouse. The victim had already removed a furniture carton from the incoming conveyor line, and was attempting to position it on the adjacent line. A co-worker working nearby heard the victim call out, and turned to see his feet disappearing over the edge of the floor opening. The victim fell 11 feet 6 inches to the concrete floor below. A co-worker contacted the local emergency medical service (EMS), which responded in approximately 5 minutes, transporting the victim to a nearby hospital. Later that day, he was transferred to a trauma center in a neighboring state, where he died the following day. NIOSH investigators concluded that, to prevent similar occurrences, employers should:
- ensure that floor openings are guarded by standard railings or covers
- establish safe work areas to ensure that work activities take place away from floor openings
- ensure that warning devices incorporating bilingual and/or symbolic signage where appropriate are displayed in work areas with floor openings
- consider installing sensing devices at approaches to floor openings which will activate automatic shutdown of conveyor lines when workers enter danger zones
- ensure that workers who are part of a bilingual workforce comprehend instructions in safe work procedures for the tasks to which they are assigned by designating experienced personnel who share the worker’s native language to act as interpreters and trainers.
INTRODUCTION
On July 13, 1995, a 37-year-old male loader/unloader (the victim) died from injuries sustained the previous day when he fell through a floor opening of a furniture warehouse conveyor line. On August 3, 1995, officials of the Virginia Occupational Safety and Health Administration (VAOSHA) notified the Division of Safety Research (DSR) of the incident and requested technical assistance. On September 12, 1995, a safety engineer and a statistician from DSR reviewed the incident with the VAOSHA compliance officer. The corporate safety director, plant manager, and the co-worker who witnessed the incident were interviewed during the site investigation conducted the following day. The incident site was examined and photographs and measurements were taken.
The employer, a furniture manufacturing firm in business at this location since the early 1900s, now employs approximately 8,000 workers at 40 facilities in 14 states. There were 440 employees at the location where the incident occurred. The warehouse and conveyor system had been in operation since the early 1970s. The victim had been employed at the warehouse for 2 weeks and had received on-the-job training in the task being performed at the time of the incident. The corporate safety director is responsible for the safety program at the site of the incident and oversees the activities of the full-time safety directors employed at each of the company’s other facilities. Safety performance is considered in evaluating the overall performance of plant managers. The company instituted an English-Spanish hazard communication program approximately 1 year prior to the incident, and offers English classes for its Spanish-speaking workers. Safety topics are incorporated into monthly meetings for supervisory staff, who are expected to communicate safety information to workers. The company has its own safety inspection program in which fines are levied against facilities where violations of OSHA standards are found. At the end of each year, the money assessed in fines is awarded to the three plants with the fewest violations and lowest workers’ compensation costs. The corporate safety director reported that there had been approximately four fatalities company-wide during his 30 years of employment there, and that none had been associated with the task being performed by the victim.
INVESTIGATION
On July 12, 1995, workers at the warehouse began work on the 7 a.m. to 3:30 p.m. shift. The normal work week is 32 to 40 hours, depending on the volume of orders to be filled. Two conveyor lines operate on the third floor of the five-story warehouse (Figure 1), one which moves furniture from an adjacent manufacturing plant into and throughout the warehouse (the incoming line), and the other which moves furniture to the first floor for shipment out of the warehouse (the outgoing line). Furniture is loaded onto “hangers,” which are chairlike cars suspended from the powered overhead trolley-type conveyor. The hangers have ¾-inch plywood covered load platforms, 30″ by 31″, bolted to the metal frames. The platforms are about 1 foot above the floor and 7 feet below the conveyor trolleys. The backs of the hangers are covered by another sheet of ¾-inch plywood extending up from the platform about 50 inches. The hangers are spaced approximately 6 feet apart, and travel approximately 42 feet per minute.
The incident occurred at a transfer location where furniture is transferred from the incoming line to the outgoing line before the outgoing line drops through a floor opening to the second floor. The outside edge of the 26 foot 7 inch by 6 foot 6 inch floor opening (the east side) was located 20 inches from the outside wall. A ledge (4¼ inches wide and 2-5/8 inches high) was located 1 foot from the opening, and extended the full width of the south side of the opening (Figure 2). A shutoff switch for the incoming conveyor was located about 12 feet from the southwest corner of the floor opening. The outgoing conveyor’s shutoff switch was located on the outside building wall 5 feet 2 inches across from the conveyor line and 3 feet 6 inches up the line from the edge of the floor opening.
The victim’s duties consisted of removing furniture cartons from hangers of the incoming conveyor line, sliding them across the floor to the adjacent conveyor line, and placing them on hangers on the outgoing line located approximately 8½ feet away. The victim had received on-the-job instruction in his task from the “lead man,” whose duties consisted of monitoring the activities of the loader/unloaders and using an electronic bar code scanner to record information about the outgoing shipments. The lead man stated that he had cautioned the victim several times during the morning of the incident about working too close to the floor opening. He also reported that he had advised him to let cartons proceed if he was having any difficulty handling them.
The employer stated that this particular floor opening, one of 13 throughout the facility, was the only opening located near a work area. Fewer furniture cartons than usual were moving through at the time of the incident. Some pieces of furniture, such as the 135-pound dresser the victim was handling, were packed in cardboard cartons that were partially open on one end, leaving the furniture legs or base exposed. The dresser the victim was loading was approximately 20 inches by 30 inches by 49 inches. The surface of the concrete floor was very smooth, allowing workers to easily slide the cardboard furniture cartons across the floor from one conveyor to the other. The loader/unloaders wore athletic shoes or other rubber-soled shoes to assure safe footing. They also wore rubber-faced gloves provided by the employer to protect their hands and to provide a secure grip on furniture cartons.
Around 1:15 p.m., the time of the incident, there were four workers in the vicinity: the victim, the lead man, and two other loader/unloaders who were working farther up the conveyor line. The lead man was removing a carton from the incoming conveyor line with his back to the victim, and the victim was positioned between the outgoing conveyor and the wall, attempting to place a carton on a hanger. The lead man stated that, before he turned away, he noticed the victim was walking backward attempting to adjust the carton more squarely on the hanger. He heard the victim call out, and turned back and saw the victim’s feet disappear as he tripped over the water ledge across the floor opening. The victim fell 11 feet 6 inches, striking his head on the concrete floor below. A co-worker notified the EMS, which responded in approximately 5 minutes. The victim was transported to a hospital in a nearby town, transferred to a trauma center in the neighboring state, and died the following day without regaining consciousness.
CAUSE OF DEATH
The cause of death was determined to be head and chest injuries.
RECOMMENDATIONS
Recommendation #1: Employers should ensure that floor openings are guarded by standard railings or covers.
Discussion: At the time of the incident, the floor opening was partially guarded by standard railings (i.e., 42-inch high top rail, midrail, and toeboard). One railing extended along the full 26 foot 7 inch length of the west edge of the floor opening. Another extended across the 6½-foot width of the north end of the floor opening and continued to the building wall. At the south end of the opening, the standard railing extended from the southwest corner of the floor opening 20 inches to the building wall. Since the incident, the employer has extended the west 26 foot 7 inch standard railing an additional 8 feet beyond the southwest corner of the floor opening, and has added a standard railing the full length of the east edge of the opening.
At the time of the incident, the south edge of the floor opening providing conveyor access was not guarded. The employer has since covered the opening with an 800-pound-capacity cargo net which extends about 10 feet from the south edge (Figure 2). This method of covering offers fall protection yet still allows the conveyor to descend unimpeded through the opening. In response to reports that workers commonly sat on standard railings during break periods, the employer has also covered the north end with a second net secured to the top rail.
Recommendation #2: Employers should establish safe work areas to ensure that work activities take place away from floor openings.
Discussion: The conveyor lines ran parallel to each other beginning at the edge of the floor opening and continuing for 30 feet until the incoming conveyor line turned west. At the time of the incident, workers manually transferred furniture from the incoming to the outgoing line within this work area. Apparently the victim, while positioning the carton on the hanger, moved progressively closer to the floor opening, ultimately falling backward over the water ledge. After the incident, the employer extended the standard railing 8 feet beyond the threshold of the opening, effectively moving the available work area away from the opening.
Recommendation #3: Employers should ensure that warning devices incorporating bilingual and/or symbolic signage where appropriate are displayed in work areas with floor openings.
Discussion: There were no warning lines or signs in the vicinity of the floor opening at the time of the incident. Since the incident, the employer has marked a danger zone by painting prominent diagonal yellow warning lines on the floor in the 8 foot long by 6½ foot wide area in front of the floor opening. Warning signs in English and Spanish have been affixed to the new 8-foot section of standard railing along the inside length of the opening. The employer has no educational prerequisites for prospective employees, thus there is no guarantee that employees, Spanish speaking or otherwise, can read the signs in either language. Additional signs using symbols rather than text would illustrate the hazards associated with the floor opening to all workers regardless of their literacy or language skills.
Recommendation #4: Employers should consider locating automatic conveyor shutdown devices at approaches to floor openings near areas where material is manually transferred between conveyors.
Discussion: The victim had about 40 seconds to transfer a piece of furniture from one line to the other. The available work area was about 30 feet, and the conveyors travel at a rate of about 42 feet per minute. If in that amount of time the furniture was not securely positioned on the hanger, unwritten company policy dictated that the worker should allow the furniture to continue on the line without regard for its security. During the transfer of material from one line to the other, the victim’s safety depended upon his ability to remain cognizant of his location relative to the floor opening while walking backward with the conveyor line and adjusting the position of the furniture on the hanger. A pressure sensitive mat such as those used to activate automatic doors, placed before the approach to the floor opening, could be used to automatically shut down the conveyor, thereby stopping worker movement toward the opening without relying on the worker’s sense of location.
Recommendation #5: Employers should ensure that workers who are part of a bilingual workforce comprehend instructions in safe work procedures for the tasks to which they are assigned by designating experienced personnel who share the worker’s native language to act as interpreters and trainers.
Discussion: The lead man assigned to explain the victim’s task to him did not speak Spanish, nor did any of the other workers in the area. It is not known to what extent the victim understood English; however, it was not his native language. To safely perform the task assigned to him, the victim needed to understand the importance of avoiding the floor opening, as well as the area available to safely accomplish the transfer of furniture from one conveyor line to the other. The lead man explained the task to him in English, but because of the language difference, had difficulty evaluating the victim’s understanding of the work instructions. The lead man indicated that he and the victim had very little conversation during the morning prior to the incident; however, he had told the victim that if he had difficulty placing a piece of furniture on a hanger he should allow the unstabilized furniture to proceed instead of risking getting too close to the floor opening. Since there were no warning signs or symbols in the work area, the lead man could only demonstrate the work task and signal for the victim to move away from the opening if he approached it too closely. A significant portion of the workforce at this location was Hispanic, and the employer had implemented a bilingual hazard communication program; however, bilingual on-the-job, task-specific training was not necessarily provided. It is difficult to evaluate worker comprehension of training when both trainer and worker share a common language, and more so when there is a language barrier, as may have been the case in this incident. Employers could ensure that workers comprehend training and instructions by designating experienced workers to act as interpreters, trainers, and safety representatives.
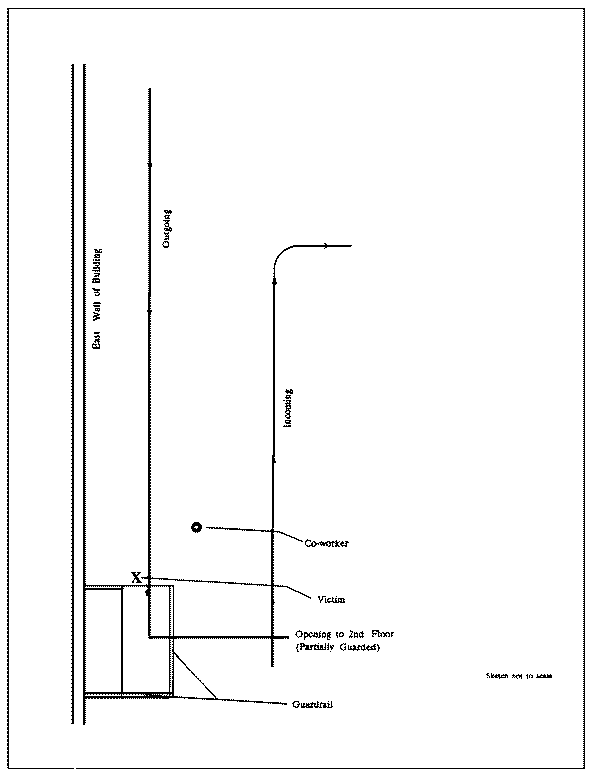
Figure 1.
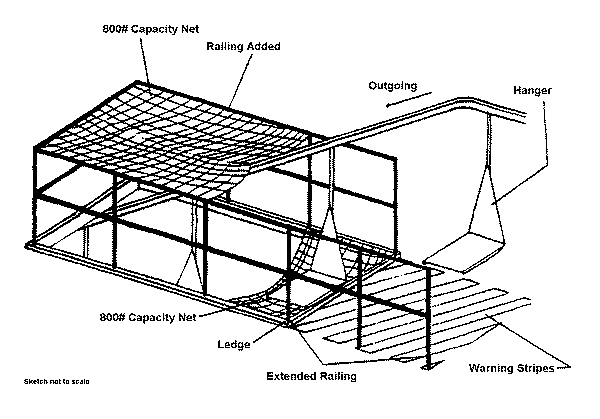
Figure 2.