
FATAL INCIDENT SUMMARY REPORT: FIRE AT A WASTEWATER TREATMENT PLANT
FACE 84ll
INTRODUCTION
The National Institute for Occupational Safety and Health (NIOSH) Division of Safety Research (DSR) is currently conducting the Fatal Accident Circumstances and Epidemiology (FACE) study. By scientifically collecting data from a sample of similar fatal incidents, this study will identify and rank factors which increase the risk of fatal injury for selected employees.
At approximately 10:00 A.M. on December 29, 1983, a fire occurred in the floating cover of a digestion tank at a secondary sewage treatment plant. The fire caused the asphyxiation of two laborers (54 and 34 years of age) who were preparing the tank for painting. The attending medical examiner notified DSR about this incident approximately three hours after it occurred and requested technical assistance with taking and analyzing air samples and collecting information about the circumstances.
CONTACTS/ACTIVITIES
Subsequent to receiving notification, DSR in collaboration with NIOSH’s Division of Respiratory Disease Studies sent a research team, consisting of an epidemiologist, fire protection engineer, civil engineer, and three industrial hygienists to the incident site at approximately 1:30 p.m. on December 29. Upon arrival at the site, activities included air sampling and analysis along with initial collection of information about the circumstances of the incident. An operating 24″ (diameter) Super Vac smoke ejector was observed over the manhole of the floating cover and witnesses said that it had been placed there soon after the incident in order to ventilate the confined space. Direct reading measurements were taken using an MSA Portable Combustible Gas and 02 alarm, Model 260, and an Auer Methanometer, Model M502. Tedler bag samples were collected through an extension tube lowered into the interior of the floating cover where the incident occurred, and also lowered into the digester itself. Charcoal sorbent tube samples, collected using a Dupont P-400 pump operated at one-liter per minute, were also taken from within the floating top and digester. The team also returned to the site at 8:30 a.m. on December 30 in order to repeat the air analyses. During the surveys, 35 mm pictures were taken of the incident site.
Subsequent to these site visits, a conference call was held with officials at ,the company who employed the victims. Information obtained during this interview pertained to the company’s background, management characteristics, training program, safety program, procedures for working in confined spaces, history of activities at wastewater treatment plants and the incident site, and account of the incident background and sequence. Other interviews were held with the job foreman, project engineer, co-workers, and next-of-kin. Two companion workers were randomly selected and interviewed.
SYNOPSIS OF EVENTS
The company employing the victims was contracted by the city government to clean and repaint two sewage digestion tanks at its wastewater treatment’ plant. The company has approximately 135 employees and was also serving as the contractor to do similar jobs at two other wastewater treatment plants in The two victims had started working for this company in August, the state. 1981.
The company had completed work on the number I digestion tank and had begun work on the number 2 tank. In October of 1983, this tank had been taken off line and a subcontractor had cleaned the ‘tank of sewage. The company then sandblasted, scraped, and repainted the inside of the tank. During this activity, propane cylinders and salamander heaters were used inside the tank to minimize condensation and the smoke ejector was used to ventilate the workspace. By Christmas week, the exterior surface of the floating cover was being prepared for cleaning and repainting.
The floating circular cover consisted of a confined space of approximately 6400 cubic feet with a five foot ceiling height at the apex (see figure 1). The only entry into the cover was through a 30″ diameter manhole located approximately ten feet from the apex. Due to the cold and windy winter weather, the carpenters built a temporary roof (2″ x 4″ studs covered with 8-10 mil. plastic sheeting) over the floating cover.
During the week of the incident, preparations were made for painting the exterior of the floating cover. On Monday and Tuesday (December 26 and 27), the areas above and within the cover were heated with propane fueled salamanders. using 100 pound cylinders through a regulator and hose assembly. On Wednesday (December 28), it rained and one or both of the victims helped clear water from the temporary plastic roof. The job foreman was not sure if or how the heaters were used that day. On the day of the incident, the two laborers (victims) and four carpenters reported to the wastewater treatment plant at approximately 7:00 a.m. The victims were to heat the floating cover so that it could be painted that afternoon. The carpenters were there to erect a temporary enclosure for air compressors located on the ground by the side of the number 2 digestion tank. At the beginning of the shift, the laborers checked the propane cylinders that had been used inside and on top of the floating cover and at other locations) at the plant. They reported to the job foreman that six of seven 100 lb. cylinders were empty. After collecting these empty cylinders, the foreman transported them for refilling and then returned them to the laborers. A morning coffee break was then taken at around 9:30 a.m. and the carpenters and laborers went back to work approximately 15 minutes later. The laborers went back to the floating cover while the carpenters resumed work on the temporary enclosure.
At approximately 10:00 a.m., one of the carpenters who was working from a ladder saw flames shooting four feet above the plastic sheeting of the temporary roof. He reported hearing a noise or roar and thought the flames lasted approximately fifteen seconds. By the time carpenters arrived-on the top of the cover, the flame has apparently gone out but smoke was issuing from the manhole. The carpenters were uncertain about the location of the laborers. They found one salamander operating in a normal(burning) mode and two propane cylinders lying on top of the floating cover. Carrying,a flashlight and with a handkerchief over his face, one carpenter entered-the manhole to look for the laborers. After going only a few feet, he began to choke on the smoke and d decided to leave the interior of the cover. The carpenters then placed the 24″ diameter Super Vac smoke ejector on a scaffold section over-the manhole in an attempt to remove the smoke. This-ejector had a rat ed capacity (free air) of 10,000 cfm, and therefore, given adequate make-up air from the outside, calculations show that it could have cleared the area to 1% of its original concentration of smoke within approximately three minutes.
After being notified at approximately 10:10 a.m., firefighters from two local f ire departments arrived at the scene. The first arriving unit stretched a 1-1/2″ water line into the cover but apparently found no fire. Also, one firefighter and a carpenter removed one propane cylinder from inside the manhole. Two firefighters, wearing self-contained breathing apparatus, .entered the floating cover. They reported heavy smoke, low visibility and-a propane like” cloud of vapor hanging in one area of the confined space. They subsequently found and removed a second cylinder, hose and regulator assembly, and salamander from inside the cover a few feet from the manhole. Both cylinder valves were reported tobe closed and there was some question as to whether or not one cylinder was attached to the salamander.
After entering the cover, the two firefighters made a counterclockwise sweep close to the center of the tank. One hard hat was found approximately 201 from the manhole. During a second sweep more towards the outside of the cover, a helmet liner was found and then the two bodies. Both victims were found lying face down and no vital signs were present (see Figure 2). The older victim had overalls which were singed and a cigarette lighter was found near his body. The two victims were pronounced dead on the scene by the attending medical examiner and were transported to the morgue at a local hospital.
The responding firefighter units also took combustible gas readings (presumably with an MSA Model 2 Explosimeter) and values of 10-25 (percent LFL) were reported. However, no oxygen or temperature measurements were reported nor was the calibration of the instrument known.
The area involved in the fire was confined to roughly a circular patch above the manhole. Several 2″ x 4″ boards used to support the plastic roof were badly burned above the manhole. Discoloration extended upward to but not beyond the crossbeams. Areas of plastic sheeting were melted around the burned board, but did not extend as far as the discoloration.
The police confiscated the two 100 lb. propane cylinders, one regulator hose assembly and one salamander heater found within the floating cover. The police reported that the hose and regulator showed some fire damage and that the reset button on the automatic pilot valve stuck in the open position and appeared to be bent. The heater, regulator/hose and tanks located on the top of the floating cover were directly observed in the field by the NIOSH research team. The reset button on this pilot valve had been wired down so that it remained in the open position at all times.
MEDICAL FINDINGS
Both victims died from acute carbon monoxide intoxication. The younger victim had a blood carbon monoxide saturation of 78% while the older victim’s blood carbon monoxide saturation was 73%.
The younger victim had no cutaneous burns. The hair at the sides and back of the head (in a distribution which would be of the hair not covered by a cap), the eyebrows, and the mustache were singed. Toxicologic analysis of the blood was negative for ethyl alcohol and drugs. Urine analysis was negative for common acidic, basic, neutral and narcotic drugs and positive (trace amounts) for benzodiazepins. The endotracheal air specimen was positive for propane.
The older victim had second degree burns on the backs of his-hands and his face. His scalp was lacerated and there were abrasions on one side of his face. Toxicologic analysis of blood and urine samples were negative. The endotracheal air specimen was positive for propane.
CONCLUSIONS
Combustible gas measurements and oxygen readings taken at the incident site by the research team showed no concentration of combustible gas and 21% oxygen at all locations. Air samples taken after cover ventilation by the smoke ejector’ and the next day after the tank had been allowed to “sit” overnight without ventilation, failed to show any significant concentration of flammable gas. Infrared analysis of the grab samples indicated hydrocarbons present in only ppm concentrations similar to those found as background in room air. More sensitive charcoal tube analysis failed to find methane but indicated the presence of propane.
Given these lab results and the toxicologic findings of propane in the endotracheal samples from both victims, the probable fuel source is propane. Both tanks removed from inside the cover after the incident were weighed (gross) and seem to contain most, if not all of the contents. Therefore, the probable source of propane was one (or more) of the empty cylinders that had been refilled the morning of the incident.
Consideration was given to a probable ignition source. operations of sand blasting, scraping or painting had not begun the morning of the incident as evidenced by the failure to find equipment on the scene for any of these operations. Witnesses stated that the younger victim smoked. A cigarette lighter (possibly belonging to the younger victim) was found near the body of the older victim. A co-worker stated that the older victim frequently asked to borrow lighters or matches to start the heaters. Smoking material (discarded cigarette packs and butts) were found on top of the cover and in the digestion tank but not inside the floating cover. The salamander, if burning, would provide an adequate source of ignition for a flammable atmosphere. It is uncertain that it was burning at the time of the fire. Other than the lighter or salamander, no other credible source of ignition could be found.
Since the fire occurred in a confined space, the presence of oxygen throughout the tank cannot be taken for granted. Oxygen measurements were reportedly not taken until at least 3-1/2 hours after the fire and then only after extensive ventilation efforts with the smoke ejector. Oxygen deficiency could result from either consumption(chemical reaction) or displacement. Chemical reaction with the steel tank walls (rusting) seems unlikely since 21% oxygen was found in all measurements taken after the fire. In a confined space with the volume of the floating cover, oxygen depletion and the concurrent displacements by the products of combustion would not allow complete combustion of 100 lbs. of propane. Therefore, if a full cylinder attached to a salamander heater had been placed inside the cover and left to provide continuous heat, both the burner and pilot flames would eventually extinguish.
The heater’s control value along with the heater, cylinder and regulator are currently being tested by an independent laboratory. If the reset button on the value was defective (stuck in the open position) and the flame extinguished from the lack of oxygen, propane would continually be released until the cylinder was emptied. Subsequent mixing with the confined space environment would be incomplete with a higher oxygen level around the only opening, the manhole. Propane concentrations would vary nearly inversely with oxygen concentrations from low around the manhole to very high in stagnant pockets, especially near the floor of the cover. This incomplete mixing may be one explanation of why one or both victims did not react to the odor of the mercaptan in the propane while standing near the manhole.
A factor in the occurrence of this fatal incident was the cold weather. The painting of floating covers of other digestion tanks had been successfully completed by the company in warmer weather without the need to provide supplemental heating. The company had never before needed nor attempted to heat the inside of a floating cover.
Another factor was the lack of recognition of the floating cover as a confined space, both in terms of a,limited environment and limited entry/escape. All company employees interviewed (from the co-workers, job engineer and job foreman to the president of the company) did not fully understand the hazards associated with this confined space.
Insufficient information precludes conclusion about the location of both victims at the time of the fire. Either both were inside the cover or the older victim was inside and the younger victim was outside, on top of the cover. If the latter was the case, the younger victim, a member of a local rescue squad, could have attempted a rescue and entered the confined space after the fire.
Apparently equipment was not available for the workers to assess the. combustible nature of the environment. Neither were emergency respirators readily available. Had either of these items been accessible, the fatal outcome might have been averted. No confined space entry procedures or precautions were followed (for example, testing of the atmosphere, life support equipment, rescue, etc.).
In conclusion, and based upon available information, the major elements of a hypothetical reconstruction are as follows:
1. Day(s) before the fire, workmen place a salamander and propane cylinders) inside the floating cover for space heating.
2. The salamander burns until the available oxygen for combustion is depleted and the products of combustion partially inert the confined space. Also, based upon alleged fire damage, the regulator and/or hose may have leaked propane.
3. The pilot and burner flames go out.
4. The flame out safety device does not prevent unburned propane from being fed through the burner and the tank contents are depleted.
5. The workmen return and find the cylinder empty and remove it for refilling.
6. The workmen lower two refilled 100 lb. propane cylinders through the manhole.
7. One or both workmen enter the confined space.
8. One or both workmen connect or attempt to connect the full cylinder.
9. Ignition occurs in the area around the manhole burning one workman and igniting his clothing. Ignition may have resulted while attempting to light the salamander.
10. Based upon alleged fire damage, fire may have flashed to the leaking regulator and/or hose and damaged them.
11. Fire propagates (approximately 15 seconds) until areas with concentrations outside the flammable range are reached.
12. Flame extends outside the manhole and impinges on plastic roof, melting the plastic and igniting the 2″ x 4″s.
13. One or both men crawl to escape flames and both are overcome by oxygen deficiency and carbon monoxide (note carboxyhemoglobin level).
14. The clothes of one workman are extinguished by the oxygen deficiency.
RECOMMENDATIONS
it is important for all employees (including management) in an organization to be able to recognize work environments which are confined spaces and to fully comprehend the potential hazards associated with those environments. in organizations where such recognition and comprehension is not sufficient, further education and reinforcement efforts are needed.
Once a confined space is identified, any work activity associated with that space should follow the guidelines recommended by NIOSH in its document, Criteria for a Recommended Standard … Working in Confined Spaces” (DHEW (NIOSH) Publication No. 80-106, December 1979). These recommendations include specific procedures for entry and rescue, permit systems, training, testing and monitoring, work practices, etc.
Future efforts should evaluate the feasibility of designing and/or providing automatic pilot valves whose reset buttons cannot be intentionally, or unintentionally made inoperative.
Finally, victims of confined space incidents are often rescuers who attempt to save a worker(s). In this case, there was a near-miss with one carpenter. Also, the possibility exists that the younger victim could have died as the result of a rescue attempt. All organizations who have employees who work in confined spaces should increase educational efforts dealing with entry and proper rescue responses.
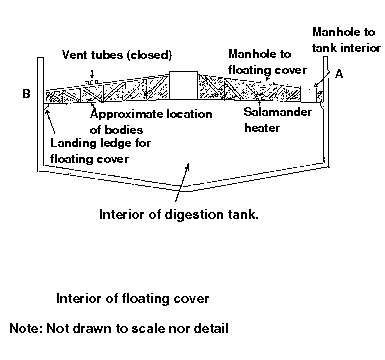
Figure 1. Side view of digestion tank with flashing cover
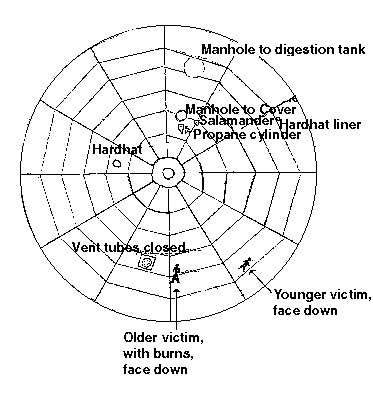
Figure 2. Top view of digestion tank showing location of victims