
Maintenance Mechanic Dies After Being Trapped in the Pneumatic Door of a Vacuum Cooler - South Carolina
NIOSH In-house FACE Report 2002-05
October 29, 2003
Summary
On January 2, 2002, a 37-year-old maintenance mechanic (the victim) died after being caught between the rear of a vacuum cooler tube and the cooler tube’s door. On December 31, 2001, the victim and his shop foreman changed the control valve that controlled the air flow that raised and lowered the vacuum cooler tube’s 2,000-pound door. On the morning of January 2, 2002, the foreman instructed the victim to check to see if the door was operating properly before the vacuum cooler was placed back into service. Using the control on the pneumatic valve, the victim partially raised the door. As he positioned himself between the door and the rear of the cooler tube, one of the air lines on the pneumatic valve blew off, allowing the door to lower, pinning the victim between the door and the rear of the cooler tube. The foreman heard the rush of air and walked around the tube, finding the victim pinned. He held the air line on the pneumatic valve by hand, and raised the door allowing the victim to fall to the shop floor. Coworkers initiated cardiopulmonary resuscitation while the foreman called 911 from the shop office. The emergency medical service (EMS) responded and transported the victim to the hospital where he was pronounced dead.
NIOSH investigators concluded that, to help prevent similar occurrences, employers should:
- develop, implement, and enforce a comprehensive written safety program for all workers which includes training in hazard recognition and the avoidance of unsafe conditions
- continually stress the importance of following standard operating procedures
Additionally, manufacturers should:
- evaluate system components to determine which would be the most reliable and provide workers with the safest work environment
Introduction
On January 2, 2002 a 37-year-old maintenance mechanic (the victim) for a wholesale produce and vacuum cooling service died after being caught between the rear of a vacuum cooler tube and the cooler tube’s door. On February 19, 2002, the National Institute for Occupational Safety and Health (NIOSH), Division of Safety Research (DSR) was notified of the incident by officials of the South Carolina Occupational Safety and Health Administration (SCOSHA). On April 9th and 10th, a DSR lead occupational safety and health manager conducted an investigation of the incident. The incident was reviewed with the county sheriff’s office, personnel from SCOSHA, and the employer’s director of human resources and shop foreman. The cause of death was obtained from the coroner over the phone. Digital images of the vacuum cooler tube were taken during the investigation.
The employer was a wholesale produce and vacuum cooling service establishment that had been in operation since 1957 and employed 53 workers, 17 at the shop where the incident occurred. After the vegetables are harvested from the fields, they are loaded and quick-cooled in the vacuum coolers during transport to the farmers’ market for sale. Prior to the incident, the employer had no written safety program. The victim had worked as a maintenance mechanic for the employer for 18 years. This was the employer’s first fatality.
Back to Top
Investigation
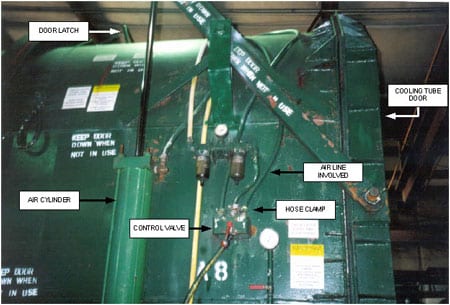
Vacuum coolers, such as the one involved in the incident, are used in the vacuum cooling of almost any type of vegetable. Vacuum cooling is a rapid pre-cooling that preserves vegetables by placing them in an almost complete vacuum. These portable vacuum coolers are transported behind a semi-tractor and can be set up anywhere there is room for a semi-tractor to maneuver. The coolers are powered by self contained diesel engines and weigh approximately 30 tons. The entire unit is 44 feet long, with a cooling tube 22 feet long in a unit that can accommodate five wooden pallets. The employer had a total of 20 vacuum coolers that were manufactured in the company shop. Each cooler was equipped with a back door measuring 114 inches high, 86 inches wide, weighing 2,000 pounds. The tailgate or bottom rear edge of the cooling tube was 29 inches off the ground. Each door was fabricated from 3/8 inch steel plate and 6 inch channel and I-beams. The doors were raised pneumatically by two, 6-inch air cylinders located on each side of the rear of the cooling tube. Air to operate the cylinder was supplied at 125 to 135 pounds per square inch (psi) by a compressor located at the front of the unit when in the field, or by a floor-mounted stationary compressor when at the shop. Air lines rated at 500 psi ran from a manually operated control valve to each air cylinder. The control valves were mounted adjacent to each cylinder. Air line connections to the cylinders and valves were secured with worm drive type hose clamps. When a door was raised to its full upright position, it automatically connected to a latch at the top of the tube that held it in place (Photo 1). Standard operating procedure, though unwritten, stated that employees were never to place themselves between the door and the back of the cooling tube or to enter the tube during loading or maintenance activities unless the door was latched to the top of the tube. At the shop, the door could also be suspended by an overhead crane
|
|
Photo 1. The configuration of the lifting mechanism of the door.
|
The control valves and the air lines on the cooling tubes were replaced on a yearly basis during scheduled maintenance activities. On December 31, 2001, a red tag that read “NO HOOK UP” was placed on the front of the unit that signified the cooling tube was undergoing service. After the door on the cooler was raised to the full upward and locked position, the victim replaced the pneumatic valve and air lines located on the left side of the tube (looking at the rear of the tube), while the supervisor replaced the right-side valve and air lines. At the end of the work day, the door was lowered to the closed and locked position.
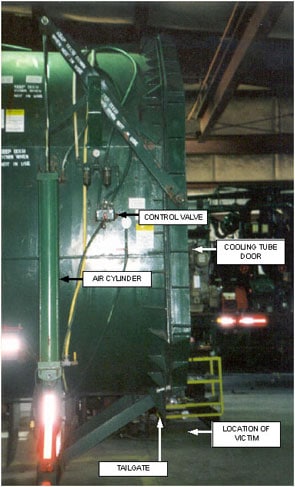
On January 2, 2002, at approximately 8:00 am, the victim was instructed by the foreman to inspect the left-side valve and the valve to air line connections to the air cylinder that he had replaced before the cooling tube was placed back into service. The supervisor then proceeded to the other side of the cooling tube to inspect his own work. At approximately 8:30am. the supervisor could hear air rushing from the other side of the cooling tube. As he walked around the tube, he saw the victim caught between the door and the tailgate of the tube. He also noticed that one of the air lines had disconnected from the valve. He connected the air line to the valve and held it on as he worked the valve, raising the door. As the door raised, the victim fell to the shop floor (Photo2). Coworkers immediately initiated cardiopulmonary resuscitation (CPR) while the foreman called 911 from the shop office. The EMS responded and transported the victim to the hospital where he was pronounced dead.
|
|
Photo 2. The incident scene and the location of the victim.
|
After the incident, the valve, airlines, and clamps were tested after the loose line was reconnected. All functioned properly. Evidence suggests that either the victim did not fully tighten the clamp over the air line on the valve connection, or that he connected it improperly.
A section of a rubber gasket located around the perimeter of the cooling tube was separated from the tube in the tailgate area. A can of adhesive was found open on the floor adjacent to the area where the victim fell to the floor when the door was opened by the supervisor. A putty knife was found on the floor of the cooling tube just inside the tailgate. This evidence would suggest that the victim had noticed the partially hanging seal and after inspecting the air line and valve connections, decided to repair it. He then partially raised the door and stood between the door and the tailgate to make repairs. As he did so, the air line separated from the control valve, allowing the door to lower and pin him against the tailgate. After the airline was reattached to the valve, the door was run through its open and close cycle several times and no malfunction was detected.
Back to Top
Cause of Death
The county coroner listed the cause of death as asphyxiation due to compression of the chest.
Recommendations and Discussion
Recommendation #1: Employers should develop, implement, and enforce a comprehensive written safety program for all workers which includes training in hazard recognition and the avoidance of unsafe conditions.
Discussion: A comprehensive safety program should be developed that includes training in hazard recognition and the avoidance of unsafe conditions. Employers should not allow workers to perform any work until appropriate safety training has been provided for the tasks assigned. In this incident, the victim had not been provided with safety training. OSHA regulations require employers to train workers to recognize and avoid unsafe conditions that may be present in their work environment and to provide training on the regulations applicable to their work (e.g. 29 CFR 1910).1 Employers are to assure that each employee has been trained, as necessary, by a “competent person.” Since the incident, the employer has developed a comprehensive safety program that addresses all tasks performed by the workers. A comprehensive confined space safety program that addresses tasks performed by workers during loading and maintenance of the cooling tubes was developed. The safety program also addressed lockout/tagout, forklift safety, emergency evacuation, and first aid. All workers working on the cooling tubes during maintenance were required to place their personal tags on the “NO HOOK UP” tag at the front of the unit. The tube could not be brought into service until all tags had been removed. Additionally, step by step procedures for all maintenance tasks to be performed on the vacuum cooler unit were developed. After the safety program was developed, all workers received documented training.
Recommendation #2: Employers should continually stress the importance of following standard operating procedures.
Discussion: Although unwritten, standard operating procedures called for the vacuum cooler’s door to be supported by an overhead crane or that the door be raised to the top of the cooler tube and locked into position before work was performed near the rear of or inside the tube. This would prevent the door from closing inadvertently due to the loss of air pressure. It would also eliminate an employee’s exposure to a potential caught-between hazard. Employers could consider developing safety checklists for employees performing maintenance tasks that would take them step by step through the process in the safest possible manner.
Additionally:
Recommendation #3: Manufacturers should evaluate system components to determine which would be the most reliable and provide workers with the safest work environment.
Discussion: Worm drive hose clamps such as those used in this instance can be over tightened to the point that the clamp worm is not fully engaged to the slots in the clamp strap. This reduces the capacity of the clamp. Employers should consider evaluating different types of clamps, such as crimp-type clamps, to determine the most suited for the job.
Back to Top
References
- Code of Federal Regulations 2000 edition. 29CFR Parts 1910. U.S. Government Printing Office, Office of the Federal Register, Washington, D.C.
Investigator Information
This investigation was conducted by Virgil J. Casini, Lead, Safety and Occupational Health Manager, Fatality Assessment and Control Evaluation Team, Surveillance and Field Investigations Branch, Division of Safety Research.