Progress Toward Poliomyelitis Eradication — Afghanistan, January 2015‒August 2016
Weekly / November 4, 2016 / 65(43);1195–1199
Chukwuma Mbaeyi, DDS1; Hemant Shukla, MD2; Philip Smith, MD2; Rudolf H. Tangermann, MD2; Maureen Martinez, MPH1; Jaume C. Jorba, PhD3; Stephen Hadler, MD4; Derek Ehrhardt, MPH, MSN1 (View author affiliations)
View suggested citationSummary
What is already known about this topic?
Afghanistan is one of three countries where indigenous wild poliovirus (WPV) transmission has never been interrupted. The Eastern and Southern regions have been the main areas in Afghanistan with endemic WPV transmission. The last case of WPV type 3 was reported in November 2012, and only WPV type 1 has been detected globally since then. WPV type 2 has been eradicated, with the last case occurring in 1999.
What is added by this report?
The number of WPV type 1 cases reported in Afghanistan in 2015 declined by 29% from levels reported in 2014, indicating progress toward the eradication of polio in the past year. The establishment of national and regional emergency operations centers has led to some improvements in the quality of immunization activities; however, WPV continues to circulate in the Eastern and Southern regions, and sporadic cases are being reported from previously polio-free areas. Worsening conflict in the Eastern and Northeastern regions is imposing significant constraints on immunization activities in both regions, and cross-border transmission of polio to and from Pakistan remains unresolved.
What are the implications for public health practice?
Afghanistan faces considerable challenges in its quest to eliminate indigenous poliovirus transmission by the end of the year. To address these challenges, it is important that leaders of the national Polio Eradication Initiative act with a sense of urgency to implement the revised National Emergency Action Plan, leveraging the assets of the emergency operations centers to improve the quality of polio immunization activities. In addition, the worsening security situation in parts of the country calls for renewed negotiations with local authorities and innovative approaches to gain access to vaccinate children in such areas.
Altmetric:
Only 74 cases of wild poliovirus (WPV) were reported globally in 2015, the lowest number of cases ever reported worldwide (1,2). All of the reported cases were WPV type 1 (WPV1), the only known WPV type still circulating; WPV type 2 has been eradicated, and WPV type 3 has not been detected since November 2012 (1). In 2015 in Afghanistan, WPV detection also declined from 2014, and trends observed in 2016 suggest that circulation of the virus is limited to a few localized areas. Despite the progress, there are concerns about the ability of the country’s Polio Eradication Initiative (PEI) to meet the goal of interrupting endemic WPV transmission by the end of 2016 (3). The deteriorating security situation in the Eastern and Northeastern regions of the country considerably limits the ability to reach and vaccinate children in these regions. Furthermore, because of frequent population movements to and from Pakistan, cross-border transmission of WPV1 continues (4). Although the national PEI has taken steps to improve the quality of supplementary immunization activities (SIAs),* significant numbers of children living in accessible areas are still being missed during SIAs, and routine immunization services remain suboptimal in many parts of the country. This report describes polio eradication activities and progress in Afghanistan during January 2015‒August 2016 and updates previous reports (5,6). During 2015, a total of 20 WPV1 cases were reported in Afghanistan, compared with 28 cases in 2014; eight cases were reported during January‒August 2016, compared with nine cases reported during the same period in 2015. To achieve interruption of poliovirus transmission in Afghanistan, it is important that the 2016–2017 National Emergency Action Plan† for polio eradication be systematically implemented, including 1) improving the quality of SIAs and routine immunization services, 2) ensuring ongoing dialogue between PEI leaders and local authorities, 3) adopting innovative strategies for reaching children in security-compromised and inaccessible areas, and 4) strengthening cross-border coordination of polio vaccination and surveillance activities with Pakistan.
Immunization Activities
Estimated national routine vaccination coverage of infants with 3 doses of oral poliovirus vaccine (OPV3) in Afghanistan increased from 75% in 2014 to 77% in 2015 (7). The proportion of nonpolio acute flaccid paralysis (NPAFP)§ cases among children aged 6‒23 months who were reported to have received ≥3 OPV doses through routine immunization services (a proxy indicator for routine OPV3 coverage) was 65% nationally in 2015, with percentages ranging from 40% in the Southern Region to 88% in the northern province of Badakhshan. The proportion of children aged 6‒23 months with NPAFP who had never received OPV either through routine immunization services or SIAs (i.e., “zero-dose” children) was approximately 1% nationally in 2015.
During January 2015‒August 2016, house-to-house SIAs in Afghanistan targeted children aged <5 years, using trivalent (types 1, 2, and 3), bivalent (types 1 and 3), and monovalent (type 1) OPV. During this period, 28 SIAs were conducted using OPV, including seven national immunization days (NIDs), six subnational immunization days (SNIDs), and 15 short-interval, additional dose, case-response vaccination campaigns.¶ In addition, SIAs using injectable inactivated poliovirus vaccine (IPV) were conducted in selected health districts in the Southern and Eastern regions where children were at high risk for poliovirus transmission. Children aged <10 years entering the country from Pakistan were vaccinated at major transit points and border crossings, and SIAs were conducted in camps for displaced persons.
The worsening security situation in the Eastern and Northeastern regions of the country has imposed considerable limitations on the ability to reach and vaccinate children in these areas. Estimates of children living in inaccessible areas** in the Eastern Region ranged from 22,938 to 131,781 during February‒August 2016. An estimated 165,333 children could not be reached in the Northeastern Region during the May 2016 NIDs. The majority of these children live in the province of Kunduz, where conflict has intensified over the past year. Taken together, the Eastern and Northeastern regions account for >350,000 children who cannot consistently be reached, representing almost 3% of the national target population of approximately 9.5 million children aged <5 years. Intermittent bans on polio SIAs in the Southern Region have also hindered access to children. Despite the constraints of inaccessibility, data indicate that the majority of missed children live in areas that are accessible for vaccination activities. Postcampaign monitoring data from the May and August 2016 NIDs suggest that up to 55% of missed children lived in areas that were accessible during the campaigns.
Lot quality assurance sampling (LQAS),†† which is used to assess the quality of SIAs (8), indicates that there were improvements in the quality of SIAs in 2016, compared with SIAs conducted during 2015. For example, the number of lots (health districts) rejected at the pass threshold of ≥80% in the 47 very high-risk districts§§ decreased from 40% in November 2015 to 17% in May 2016. Considering all assessed districts without regard to risk status, LQAS performance at the threshold of ≥80% improved from 68% in January 2016 to 78% in April 2016.
Poliovirus Surveillance
Acute flaccid paralysis (AFP) surveillance.¶¶ In 2015, the annual national NPAFP rate was 13.8 per 100,000 children aged <15 years (regional range = 9.8‒19.2) (Table). The percentage of AFP cases for which adequate stool specimens were collected was 93% (regional range = 84%‒97%). Three AFP cases were classified as polio-compatible, including two cases from Farah Province in the Western Region and one case from Nimroz Province in the Southern Region.
Environmental surveillance. Supplemental surveillance for polioviruses through sewage sampling began in Afghanistan in September 2013. Environmental surveillance is being conducted at 14 sites in five provinces (Kandahar and Helmand in the Southern Region, Nangarhar and Kunar in the Eastern Region, and Kabul City in the Central Region). WPV1 was first isolated from sewage samples in July 2014. Since then, 37 specimens from 11 sites were positive for WPV1. Nineteen (13%) of 148 sewage specimens tested positive for WPV1 in 2015. WPV1 was most recently detected in sewage samples taken from Nangarhar Province in December 2015. To date, none of the 112 specimens collected in 2016 have tested positive.
Epidemiology of WPV and Vaccine-Derived Poliovirus (VDPV)
Twenty WPV1 cases were reported in Afghanistan in 2015, compared with 28 cases in 2014. Eight WPV1 cases were reported during January‒August 2016, compared with nine during January–August 2015 (Figure 1) (Figure 2). WPV1 cases were reported from 16 (4%) of the 399 districts in Afghanistan in 2015 and from four (1%) districts as of August 31 in 2016. The Eastern Region accounted for half of the 20 WPV cases reported in 2015, and 25% of the cases were reported from the Western Region, including four cases from Farah Province and one from Hirat Province. Four of the remaining five WPV cases reported in 2015 were reported from the Southern Region (two cases from Helmand Province and one each from Kandahar and Nimroz provinces); Faryab Province in the Northern Region reported a single polio case. Among the eight WPV cases reported in 2016 as of August 31, four were from the Eastern Region, all from the district of Shigal Wa Sheltan in Kunar Province. The Southern Region has accounted for two cases (one each from Helmand and Kandahar provinces), and the remaining two cases were reported from Paktika Province in the Southeastern Region. Among the 28 WPV1 cases reported during January 2015‒August 2016, children aged <36 months accounted for 20 (71%) cases. Among these 20 children, 11 (55%) had never received OPV, two (10%) had received only 2 doses, one (5%) had received 3 doses, and six (30%) had received ≥4 doses. All eight WPV1 cases reported in 2016 were in children who had never received OPV through routine immunization services, with ages ranging from 12 to 59 months.
Genetic patterns of WPV1 isolates identified during January 2015‒August 2016 indicate localized circulation within areas with endemic transmission, including Kunar, Kandahar, and Helmand, and evidence of cross-border transmission between districts in the Eastern Region of Afghanistan and northwest Pakistan. No polio cases attributable to WPV type 3 or circulating vaccine-derived poliovirus (cVDPV)*** have been detected in Afghanistan since April 2010 and March 2013, respectively.
Discussion
Signs of progress toward polio eradication in Afghanistan during 2015–2016 include a decline in overall WPV1 incidence, a narrowing of the geographic distribution of cases, and decreased diversity of WPV1 isolates. However, persistent poliovirus circulation in the country’s core poliovirus reservoirs in the Eastern and Southern regions and the emergence of sporadic cases elsewhere highlight the need for urgent action by the country’s PEI to address program vulnerabilities.
In the Eastern Region, a surge in WPV1 cases in Nangarhar Province during July‒October 2015 was followed by sustained transmission in Kunar Province. Genetic sequencing linked some cases in the Eastern Region to active cross-border transmission, but it also indicated sustained local transmission. The Southern Region continues to show encouraging signs of reduced virus circulation, with only a few cases reported in 2015 and just a single case each reported from Helmand and Kandahar provinces to date in 2016; however, inadequate vaccination campaign quality persists. Sporadic polio cases in previously polio-free areas, such as Paktika in the Southeastern Region and Faryab Province in the Northern Region, represent importations from other parts of the country, and raise concerns about gaps in population immunity.
The establishment of emergency operations centers (EOCs) at the national level and in the Eastern, Southern, and Western regions has strengthened the management and coordination of polio eradication activities. A key focus of the EOCs has been rapid improvement in the quality of SIAs. To achieve this, several steps were taken by the country’s PEI, notably updating the list of high-risk districts, and reprioritizing 47 of these districts as very high-risk districts. Microplans in these districts were revised and are being updated before each SIA to analyze local immunization data, prepare an operational map to reach and vaccinate children, and identify special activities for hard-to-reach areas. In addition, frontline polio workers in all districts were trained using a revised training package, and the scope of the fifth-day revisit strategy for vaccinating children missed during earlier days of polio campaigns was expanded. Postcampaign monitoring and LQAS results indicate that these initiatives have yielded improvements in the quality of vaccination campaigns. However, substantial numbers of children are still being missed in accessible areas, indicating the need for further improvement in the quality of supervision and monitoring during SIAs.
There is an urgent need to improve vaccination coverage among children living in areas with security and access limitations. Key strategies already employed to achieve this, such as continued dialogue between the PEI and local authorities to gain access, the use of permanent transit teams to target and vaccinate children at all transit points close to inaccessible areas and cross-border points, and the implementation of several IPV-OPV rounds in newly accessible areas in short succession, need to be continued and scaled up wherever needed. Cross-border coordination of immunization activities and surveillance with neighboring Pakistan must remain a top priority, and immunization activities of the two countries should be synchronized whenever feasible.
Despite recent progress, Afghanistan faces significant constraints in its quest to eliminate WPV circulation by the end of 2016, notably inaccessibility and attendant gaps in population immunity. To address these challenges, it is important that priority be given to ensuring timely implementation of all elements of the updated National Emergency Action Plan.
Acknowledgments
Becky Maholland, Office of Public Health Preparedness and Response, CDC; World Health Organization Global Polio Laboratory Network.
Corresponding author: Chukwuma Mbaeyi, cmbaeyi@cdc.gov, 404-823-7764.
1Global Immunization Division, Center for Global Health, CDC; 2Polio Eradication Department, World Health Organization; 3Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC; 4Division of Bacterial Diseases, National Center for Immunization and Respiratory Diseases, CDC.
* Mass campaigns conducted for a brief period (days to weeks) in which 1 dose of oral poliovirus vaccine is administered to all children aged <5 years, regardless of vaccination history. Campaigns can be conducted nationally or subnationally (in portions of the country).
† http://polioeradication.org/wp-content/uploads/2016/07/4.2_14IMB.pdfpdf iconexternal icon.
§ Vaccination histories of children aged 6–23 months with acute flaccid paralysis who do not test WPV-positive are used to estimate OPV coverage of the overall target population and to corroborate national reported routine vaccination coverage estimates.
¶ Short-interval, additional dose campaigns are used for case-response vaccination after detection of a WPV case or during negotiated periods of nonviolence in otherwise inaccessible areas, to provide 2 doses of monovalent or bivalent OPV within 1–2 weeks.
** Areas where vaccination teams are temporarily unable to operate because of security concerns or local bans on vaccination.
†† A rapid survey method used to assess the quality of vaccination activities after SIAs in predefined areas, such as health districts (referred to as “lots”), using a small sample size. Lot quality assurance sampling involves dividing the population into “lots” and randomly selecting persons in each lot. If the number of unvaccinated persons in the sample exceeds a predetermined value, then the lot is classified as having an unsatisfactory level of vaccination coverage, and mop-up activities are recommended. If the threshold of ≥80% is met, the area/district is classified as having “passed,” although mop-up activities might still be indicated in certain areas
§§ Defined in November 2012, districts with confirmed polio cases in the previous 2 years, or confirmed polio cases in 1 of the previous 2 years, plus one of the following: reported “zero-dose” NPAFP cases in the previous 2 years; <90% estimated OPV coverage in the previous two SIAs; failed LQAS in more than one round of vaccination campaigns; average level of community awareness of SIAs <50% in previous two SIAs; and inaccessibility.
¶¶ The quality of AFP surveillance is monitored by performance indicators that include 1) the detection rate of NPAFP cases and 2) the proportion of AFP cases with adequate stool specimens. World Health Organization (WHO) operational targets for countries with endemic poliovirus transmission are an NPAFP detection rate of ≥2 cases per 100,000 population aged <15 years and adequate stool specimen collection from ≥80% of AFP cases, in which two specimens are collected ≥24 hours apart, both within 14 days of paralysis onset, and shipped on ice or frozen packs to a WHO-accredited laboratory, arriving in good condition (without leakage or desiccation).
*** VDPVs can cause paralytic polio in humans and have the potential for sustained circulation. VDPVs resemble WPVs biologically and differ from the majority of Sabin vaccine–related poliovirus isolates by having genetic properties consistent with prolonged replication or transmission.
References
- Global Polio Eradication Initiative. Independent Monitoring Board: thirteenth report, August 2016. http://polioeradication.org/wp-content/uploads/2016/09/14IMB_Report_EN.pdfpdf iconexternal icon
- Morales M, Tangermann RH, Wassilak SG. Progress toward polio eradication—worldwide, 2015–2016. MMWR Morb Mortal Wkly Rep 2016;65:470–3. CrossRefexternal icon PubMedexternal icon
- Global Polio Eradication Initiative. Polio eradication and endgame strategic plan 2013–2018. Geneva, Switzerland: World Health Organization; 2014. http://www.who.int/immunization/diseases/poliomyelitis/endgame_objective2/about/en/external icon
- Porter KA, Diop OM, Burns CC, Tangermann RH, Wassilak SG. Tracking progress toward polio eradication – worldwide, 2013-2014. MMWR Morb Mortal Wkly Rep 2015;64:415–20. PubMedexternal icon
- Farag NH, Alexander J, Hadler S, et al. Progress toward poliomyelitis eradication—Afghanistan and Pakistan, January 2013–August 2014. MMWR Morb Mortal Wkly Rep 2014;63:973–7. PubMedexternal icon
- Mbaeyi C, Saatcioglu A, Tangermann RH, Hadler S, Ehrhardt D. Progress toward poliomyelitis eradication—Afghanistan, January 2014–August 2015. MMWR Morb Mortal Wkly Rep 2015;64:1166–70. CrossRefexternal icon PubMedexternal icon
- World Health Organization. WHO vaccine-preventable diseases monitoring system: 2015 global summary. Geneva, Switzerland: World Health Organization; 2014. http://apps.who.int/immunization_monitoring/globalsummaryexternal icon
- Global Polio Eradication Initiative. Assessing vaccination coverage levels using clustered lot quality assurance sampling. Geneva, Switzerland: World Health Organization; 2012. http://polioeradication.org/wp-content/uploads/2016/09/Assessing-Vaccination-Coverage-Levels-Using-Clustered-LQAS_Apr2012_EN.pdfpdf iconexternal icon
 TABLE. Acute flaccid paralysis (AFP) surveillance indicators and reported cases of wild poliovirus (WPV), by region and period — Afghanistan, January 2015–August 2016*
TABLE. Acute flaccid paralysis (AFP) surveillance indicators and reported cases of wild poliovirus (WPV), by region and period — Afghanistan, January 2015–August 2016*
| Region of Afghanistan | AFP surveillance indicators (2015) | No. of WPV cases reported | ||||
|---|---|---|---|---|---|---|
| No. of AFP cases | Rate of nonpolio AFP† | % of AFP cases with adequate specimens§ | ||||
| Jan–Jun 2015 | Jul–Dec 2015 | Jan–Aug 2016 | ||||
| All regions | 2,718 | 13.8 | 93 | 6 | 14 | 8 |
| Badakhshan | 57 | 10.2 | 97 | 0 | 0 | 0 |
| Northeastern | 281 | 12.8 | 94 | 0 | 0 | 0 |
| Northern | 343 | 13.9 | 91 | 0 | 1 | 0 |
| Central | 439 | 9.8 | 96 | 0 | 0 | 0 |
| Eastern | 374 | 19.2 | 95 | 0 | 10 | 4 |
| Southeastern | 209 | 10.8 | 97 | 0 | 0 | 2 |
| Southern | 567 | 16.4 | 84 | 1 | 3 | 2 |
| Western | 448 | 17.2 | 95 | 5 | 0 | 0 |
* Data as of August 31, 2016.
† Per 100,000 children aged <15 years.
§ Two specimens collected ≥24 hours apart, both within 14 days of paralysis onset, and shipped on dry ice or frozen packs to a World Health Organization–accredited laboratory, arriving in good condition (without leakage or desiccation).
FIGURE 1. Number of cases of wild poliovirus type 1 (WPV1) and circulating vaccine-derived poliovirus type 2 (cVDPV2), by month and year of paralysis onset — Afghanistan, 2013–2016
FIGURE 2. Cases of wild poliovirus type 1 (WPV1), by region — Afghanistan, January 2015–August 2016*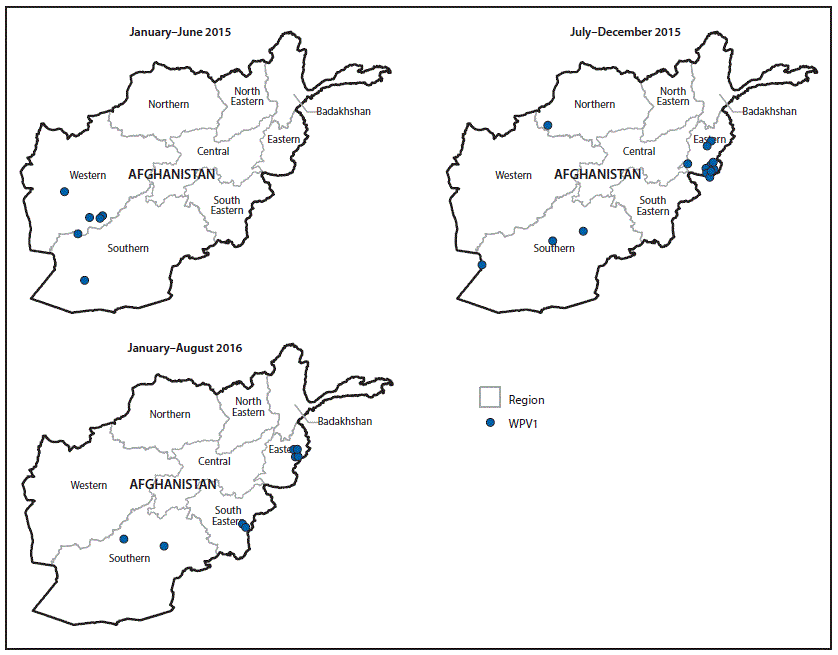
* Each dot represents one case. Dots are randomly placed within regions.
Suggested citation for this article: Mbaeyi C, Shukla H, Smith P, et al. Progress Toward Poliomyelitis Eradication — Afghanistan, January 2015‒August 2016. MMWR Morb Mortal Wkly Rep 2016;65:1195–1199. DOI: http://dx.doi.org/10.15585/mmwr.mm6543a4external icon.
MMWR and Morbidity and Mortality Weekly Report are service marks of the U.S. Department of Health and Human Services.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.
References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All HTML versions of MMWR articles are generated from final proofs through an automated process. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (https://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.