Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Surveillance for Waterborne-Disease Outbreaks --- United
States, 1999--2000
Sherline H. Lee, M.P.H.1
Deborah A. Levy, Ph.D.1
Gunther F. Craun, M.P.H.2
Michael J. Beach, Ph.D.1
Rebecca L. Calderon, Ph.D.3 1Division of Parasitic Diseases
National Center for Infectious Diseases, CDC 2Gunther F. Craun and Associates
Staunton, Virginia 3U.S. Environmental Protection Agency
Research Triangle Park, North Carolina
Abstract
Problem/Condition: Since 1971, CDC, the U.S. Environmental Protection Agency (EPA), and the Council
of State and Territorial Epidemiologists (CSTE) have maintained a collaborative surveillance system for the occurrences and causes of waterborne-disease outbreaks (WBDOs).This surveillance system is the primary source of data concerning the scope and effects of waterborne diseases on persons in the United States.
Reporting Period Covered: This summary includes data regarding outbreaks occurring during January
1999--December 2000 and previously unreported outbreaks occurring in 1995 and 1997.
Description of the System: The surveillance system includes data for outbreaks associated with drinking water
and recreational water. State, territorial, and local public health departments are primarily responsible for detecting and investigating WBDOs and voluntarily reporting them to CDC on a standard form. The unit of analysis for
the WBDO surveillance system is an outbreak, not an individual case of a waterborne disease. Two criteria must be
met for an event to be defined as a WBDO. First,
>2 persons must have experienced a similar illness after either
ingestion of drinking water or exposure to water encountered in recreational or occupational settings. This criterion is waived for single cases of laboratory-confirmed primary amebic meningoencephalitis and for single cases of
chemical poisoning if water-quality data indicate contamination
by the chemical. Second, epidemiologic evidence
must implicate water as the probable source of the illness.
Results: During 1999--2000, a total of 39 outbreaks associated with drinking water was reported by 25
states. Included among these 39 outbreaks was one outbreak that spanned 10 states. These 39 outbreaks caused illness among an estimated 2,068 persons and were linked to two deaths. The microbe or chemical that caused the outbreak was identified for 22 (56.4%) of the 39 outbreaks; 20 of the 22 identified outbreaks were associated with pathogens, and two were associated with chemical poisoning. Of the 17 outbreaks involving acute gastroenteritis of unknown etiology, one was a suspected chemical poisoning, and the remaining 16 were suspected as having an infectious cause. Twenty-eight (71.8%) of 39 outbreaks were linked to groundwater sources; 18 (64.3%) of these
28 groundwater outbreaks were associated with private or noncommunity wells that were not regulated by EPA. Fifty-nine outbreaks from 23 states were attributed to recreational water exposure and affected an estimated 2,093 persons. Thirty-six (61.0%) of the 59 were outbreaks involving gastroenteritis. The etiologic agent was identified in 30 (83.3%) of 36 outbreaks involving gastroenteritis. Twenty-two (61.1%) of 36 gastroenteritis-related outbreaks
were associated with pools or interactive fountains. Four (6.8%) of the 59 recreational water outbreaks were attributed to single cases of primary amebic meningoencephalitis (PAM) caused by
Naegleria fowleri. All four cases were
fatal. Fifteen (25.4%) of the 59 outbreaks were associated with dermatitis; 12 (80.0%) of 15 were associated with hot tubs or pools. In addition, recreational water outbreaks of leptospirosis, Pontiac fever, and chemical keratitis, as well as two outbreaks of leptospirosis and Pontiac fever associated with occupational exposure were also reported to CDC.
Interpretation: The proportion of drinking water outbreaks associated with surface water increased from
11.8% during 1997--1998 to 17.9% in 1999--2000. The proportion of outbreaks (28) associated with groundwater sources increased 87% from the previous reporting period (15 outbreaks), and these outbreaks were primarily associated (60.7%) with consumption of untreated groundwater. Recreational water outbreaks involving
gastroenteritis
doubled (36 outbreaks) from the number of outbreaks reported in the previous reporting period (18 outbreaks). These outbreaks were most frequently associated with
Cryptosporidium parvum (68.2%) in treated water venues (e.g., swimming pools or interactive fountains) and by Escherichia coli O157:H7 (21.4%) in freshwater venues.
The increase in the number of outbreaks probably reflects improved surveillance and reporting at the local and state level as well as a true increase in the number of WBDOs.
Public Health Action: CDC and others have used surveillance data to identify the types of water systems,
their deficiencies, and the etiologic agents associated with outbreaks and evaluated current technologies for providing safe drinking water and safe recreational water. Surveillance data are used also to establish research priorities, which can lead to improved water-quality regulations. Only the groundwater systems under the influence of surface water
are required to disinfect their water supplies, but EPA is developing a groundwater rule that specifies when
corrective action (including disinfection) is required. CDC and EPA are conducting epidemiologic studies to assess the level of waterborne illness attributable to municipal drinking water in nonoutbreak conditions. Rules under development
by EPA --- the Ground Water Rule (GWR), the Long Term 2 Enhanced Surface Water Treatment Rule
(LT2ESWTR), and Stage 2 Disinfection Byproduct Rules (DBPR) --- are expected to further protect the public from
contaminants and disinfection byproducts in drinking water. Efforts by EPA under the Beaches Environmental Assessment, Closure, and Health (BEACH) program are aimed at reducing the risks for infection attributed to ambient recreational water by strengthening beach standards and testing; providing faster laboratory test methods;
predicting pollution; investing in health and methods research; and improving public access to information regarding both the quality of the water at beaches and information concerning health risks associated with swimming in polluted
water. EPA's Beach Watch (available at
http://www.epa.gov/waterscience/beaches) provides online information
regarding water quality at U.S. beaches, local protection programs, and other beach-related programs. CDC partnered with a consortium of local and national pool associations to develop a series of health communication materials for
the general public who attend treated recreational water venues and to staff who work at those venues. CDC has
also developed a recreational water outbreak investigation toolkit that can be used by public health professionals. All of the CDC materials are accessible at the CDC Healthy Swimming website (http://www.cdc.gov/healthyswimming).
Introduction
During 1920--1970, statistical data regarding U.S.
waterborne-disease outbreaks (WBDOs) were collected by multiple
researchers and federal agencies (1). Since 1971, CDC, the U.S. Environmental Protection Agency (EPA), and the Council
of State and Territorial Epidemiologists (CSTE) have maintained a collaborative surveillance system that tracks the
occurrences and causes of WBDOs (2--6). This surveillance system includes data regarding outbreaks associated with drinking water, recreational water, and other types of water exposures. This report includes data for 1999 and 2000 and for
previously unreported drinking water-associated outbreaks that occurred in 1995 and 1997.
CDC's and EPA's surveillance activities are intended to 1) characterize the epidemiology of WBDOs; 2) identify
the etiologic agents that caused WBDOs and determine why the outbreaks occurred; 3) train public health personnel to
detect and investigate WBDOs; and 4) collaborate with local, state, federal, and international agencies on initiatives to prevent waterborne disease. Data obtained through this surveillance system are useful for identifying major deficiencies in
providing safe drinking water and recreational water. Surveillance information can influence research priorities, lead to improved water-quality regulations, and illustrate the burden of illness attributed to water.
Background
EPA Regulations
Drinking Water
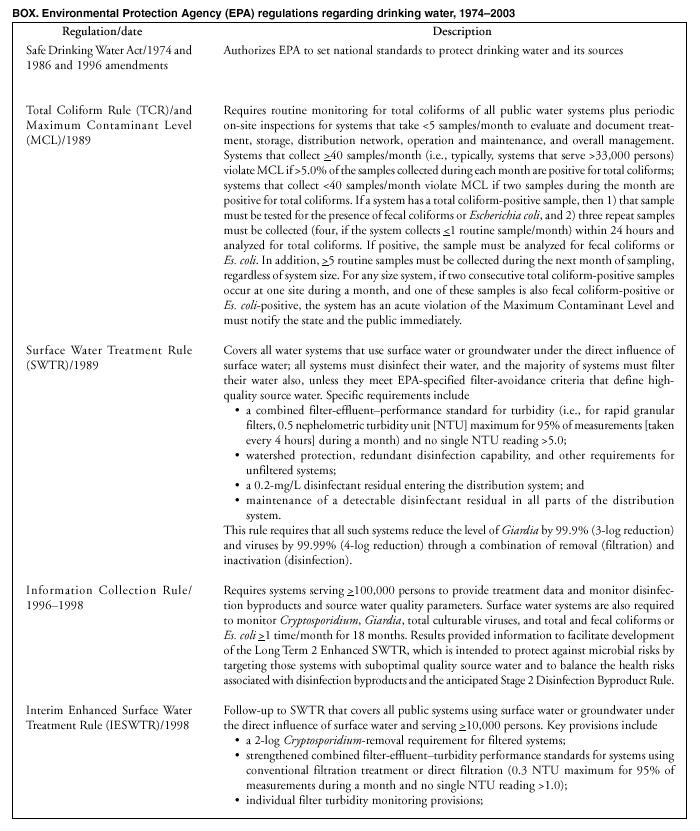
Public water systems are regulated under the Safe Drinking Water Act (SDWA) of 1974 and its subsequent 1986 and
1996 amendments (7--9) (Box. Under SDWA, EPA is authorized to set national standards to protect drinking water and its sources against naturally occurring or man-made contaminants. The 1996 SDWA amendments require EPA to publish a list every
5 years of contaminants that are known or anticipated to occur in public water systems and that might need to be regulated. The first list was called the drinking water Contaminant Candidate List (CCL). CCL contained 60 contaminants/
contaminant groups, included 10 pathogens, and was published in the
Federal Register on March 2, 1998
(10). A decision concerning whether to regulate
>5 contaminants from CCL was required by August 2001. Microbial contamination
is regulated under the Total Coliform Rule (TCR) of 1989 and the Surface Water Treatment Rule (SWTR) of 1989
(11--13). SWTR covers all water systems that use surface water or groundwater under the direct influence of surface water (Glossary). SWTR is intended to protect against exposure to
Giardia intestinalis, viruses, and
Legionella, as well as selected other pathogens. In 1998, EPA promulgated the Interim Enhanced Surface Water Treatment Rule (IESWTR) (14), which provides additional protection against
Cryptosporidium and other waterborne pathogens for systems that serve
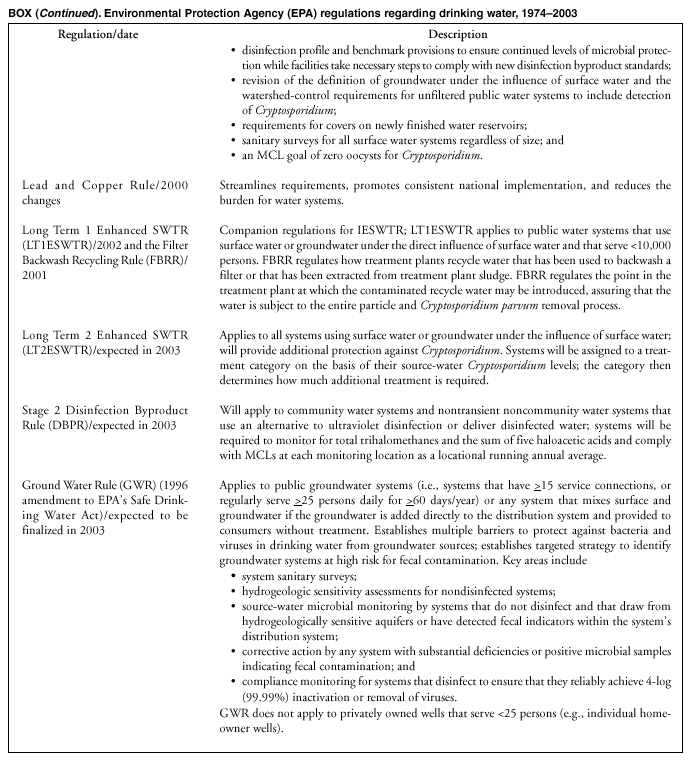
>10,000 persons. In 2002, EPA finalized the Long Term 1 Enhanced SWTR (LT1ESWTR) for public water systems that use surface water
or groundwater under the direct influence of surface water and serve <10,000 persons
(15). LT1ESWTR was proposed in combination with the Filter Backwash Recycling Rule (FBRR), which was finalized in 2001
(16,17).
The 1996 Amendments require EPA to develop regulations that require disinfection of groundwater systems as necessary
to protect the public health; EPA has proposed the Ground Water Rule (GWR) to meet this mandate
(18). GWR specifies the appropriate use of disinfection in groundwater and addresses other components of groundwater systems to ensure public health protection. GWR applies to public groundwater systems (systems that have
>15 service connections or regularly
serve >25 persons/day for >60 days/year). This rule also applies to any system that mixes surface and groundwater if
the groundwater is added directly to the distribution system and provided to consumers without treatment. GWR does not
apply to privately owned wells. Additional protection of groundwater from both chemical and microbial contamination
from shallow wells (including cesspools) is expected to be provided as a result of recent revisions to the Underground Injection Control Regulations, published December 7, 1999
(19).
To fill gaps in existing data regarding occurrence of microbial pathogens and other indicators of microbial contamination, occurrence of disinfection byproducts, and characterization of treatment processes, EPA promulgated the Information Collection Rule in 1996 (20), which required systems serving
>100,000 persons to provide treatment data and
monitor disinfection byproducts and source-water--quality parameters. Surface water systems are also required to monitor for the presence of Cryptosporidium,
Giardia, total culturable viruses, and total* (Glossary) and fecal coliforms or
Escherichia coli >1 time/month for 18 months. The required monitoring ended in December 1998, and data were analyzed.
EPA also made minor changes in 2000 to the Lead and Copper Rule to streamline requirements, promote
consistent national implementation, and in certain cases, reduce the burden for water systems. The action levels of 0.015 mg/L for lead and 1.3 mg/L for copper remain the same
(21).
Recreational Water
Regulation of recreational water is determined by state and local governments. Standards for operating, disinfecting,
and filtering public swimming and wading pools are regulated by state and local health departments and, as a result, are varied.
In 1986, EPA established a guideline for microbiological water quality for recreational freshwater (e.g., lakes and ponds)
and marine water (22). The guideline recommends that the monthly geometric mean concentration of organisms in
freshwater should be <33/100 mL for enterococci or
<126/100 mL for Es. coli. States have latitude regarding their guidelines
or regulations and can post warning signs to alert potential bathers until water quality improves. Unlike treated venues
where disinfection can be used to address problems with microbiological quality of the water, contaminated freshwater can require weeks or months to improve or return to normal. Prompt identification of potential sources of contamination and remedial action is necessary to return bathing water to an appropriate quality for recreational use
(23).
EPA's Action Plan for Beaches and Recreational Waters (Beach Watch) was developed as part of the Clean Water
Action Plan.† The intent of Beach Watch is to assist state, tribal, and local authorities in strengthening and extending programs that specifically protect users of recreational waters. As part of the Beaches Act of 2000, the U.S. Congress directed EPA to
also develop a new set of guidelines for recreational water based on new water-quality indicators. Beginning in 2003, EPA will be conducting a series of epidemiologic studies at recreational fresh and marine beaches in the United States. These studies will be used to develop guidelines for using the new water-quality indicators to be included in new EPA guidelines.
Data collected as part of the national WBDO surveillance system are used to describe the epidemiology of
waterborne diseases in the United States. Data regarding water systems and deficiencies implicated in these outbreaks are used to assess whether regulations for water treatment and monitoring of water quality are adequate to protect the public against
disease. Surveillance also enables identifying etiologic agents and environmental or behavioral risk factors that are responsible for these outbreaks. This information is used to inform public health and regulatory agencies, water utilities, pool operators, and
other
stakeholders of new or reemerging trends that might necessitate different interventions and changes in policies and resource allotment.
Methods
Data Sources
State, territorial, and local public health agencies have primary responsibility for detecting and investigating WBDOs,
and they voluntarily report them to CDC on a standard form (CDC form 52.12, which is available at
http://www.cdc.gov/healthyswimming). The form solicits data related to 1) characteristics of the outbreak, including person, place, time, and location of the outbreak; 2) results from epidemiological studies conducted; 3) specimen and water sample testing; and
4) factors contributing to the outbreak, including environmental factors, water distribution, and disinfection concerns.
Each year, CDC requests reports from state and territorial epidemiologists or from persons designated as WBDO
surveillance coordinators. Additional information regarding water quality and treatment is obtained from the state's drinking water agency as needed. Numerical and text data are abstracted from the outbreak form and supporting documents and are entered into
a database before analysis.
Definitions§
The unit of analysis for the WBDO surveillance system is an outbreak, not an individual case of a waterborne disease.
Two criteria must be met for an event to be defined as a WBDO. First,
>2 persons must have experienced a similar illness
after either ingestion of drinking water or exposure to water encountered in recreational or occupational settings. This criterion is waived for single cases of laboratory-confirmed primary amebic meningoencephalitis and for single cases of
chemical poisoning if water-quality data indicate contamination
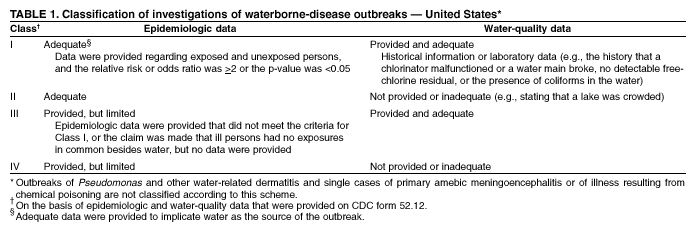
by the chemical. Second, epidemiologic evidence (Table
1) must implicate water as the probable source of the illness. For drinking water, reported outbreaks caused by contaminated water or ice at the point of use (e.g., a contaminated water faucet or serving container) are not classified as WBDOs.
If primary cases (i.e., among persons exposed to contaminated water) and secondary cases (i.e., among persons who
became ill after contact with primary persons) are distinguished on the outbreak report form, only primary cases are included in the total number of cases. If both actual and estimated case counts are included on the outbreak report form, the estimated
case count can be used if the population was sampled randomly or the estimated count was calculated by applying the attack
rate to a standardized population.
Public water systems, which are classified as either community or noncommunity (Glossary), are regulated under
SDWA. Of the approximately 170,000 public water systems in the United States, 113,000 (66.5 %) are noncommunity systems,
of which 93,000 are transient systems (i.e., public water systems that regularly serve
>25 of the same persons for >6
months/year [e.g., highway rest stations, restaurants, and parks with their own public water systems]) and 20,000 are nontransient systems (Glossary). A total of 54,000 systems (31.8%) are community systems. Community water systems serve approximately
264 million persons in the United States (96.0% of the U.S. population). Approximately 11 million persons (4.0%) rely on
private or individual water systems (24,25) (Glossary). These statistics exclude outbreaks associated with these sources because they are not intended for drinking and are not considered to be public water systems. Also excluded from these statistics are
the millions of persons who use noncommunity systems while traveling or working.
In this surveillance system, outbreaks associated with water not intended for drinking (e.g., lakes, springs, and creeks
used by campers and boaters; irrigation water and other nonpotable sources with or without taps) are also classified as
individual systems (Glossary). Sources used for bottled water are also classified as individual systems; bottled water is not regulated by EPA but is subject to regulation by the Food and Drug Administration (FDA).
Each drinking water system associated with a WBDO is classified as having one of the deficiencies in the following list.
If >1 deficiency is noted on the outbreak report form, the deficiency that most likely caused the outbreak is noted. Deficiency classifications are as follows:
1: untreated surface water;
2: untreated groundwater;
3: treatment deficiency (e.g., temporary interruption of disinfection, chronically inadequate disinfection, or inadequate or no filtration);
4: distribution system deficiency (e.g., cross-connection, contamination of water mains during construction or repair,
or contamination of a storage facility); and
5: unknown or miscellaneous deficiency (e.g., contaminated bottled water) or water source not intended for drinking (e.g., irrigation water tap).
Recreational waters include swimming pools, wading pools, whirlpools, hot tubs, spas, water parks, interactive fountains, and fresh and marine surface waters. Although the WBDO surveillance system includes whirlpool- and hot tub-associated outbreaks
of dermatitis caused by Pseudomonas
aeruginosa, wound infections resulting from waterborne organisms are not included.
Outbreak Classification
WBDOs reported to the surveillance system are classified according to the strength of the evidence implicating water as the vehicle of transmission (Table 1). The classification scheme (i.e., Classes I--IV) is based on the epidemiologic and water-quality data provided with the outbreak report form. Epidemiologic data are weighted more than water-quality
data. Although outbreaks without water-quality data might be included in this summary, reports that lack epidemiologic data were excluded. Outbreaks of dermatitis and single cases of either primary amebic meningoencephalitis or illness resulting from chemical poisoning were not classified according to this scheme. Weighting of epidemiologic data does not preclude
the relative importance of both types of data. The purpose of the outbreak system is not only to implicate water as the vehicle for the outbreak, but also to understand the circumstances that led to the outbreak.
A classification of I indicates that adequate epidemiologic and water-quality data were reported (Table 1); however,
the classification does not necessarily imply whether an investigation was optimally conducted. Likewise, a classification of II, III, or IV should not be interpreted to mean that the investigations were inadequate or incomplete. Outbreaks and the
resulting investigations occur under various circumstances, and not all outbreaks can or should be rigorously investigated. In addition, outbreaks that affect fewer persons are more likely to receive a classification of III, rather than I, on the basis of the relatively limited sample size available for analysis.
Results
Outbreaks Associated with Drinking Water
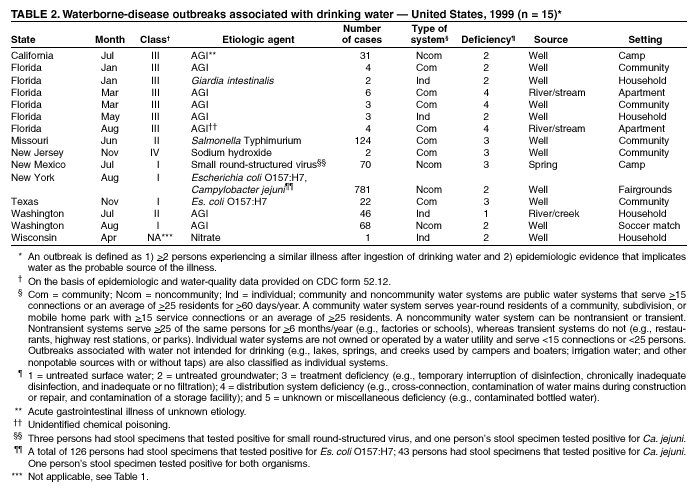
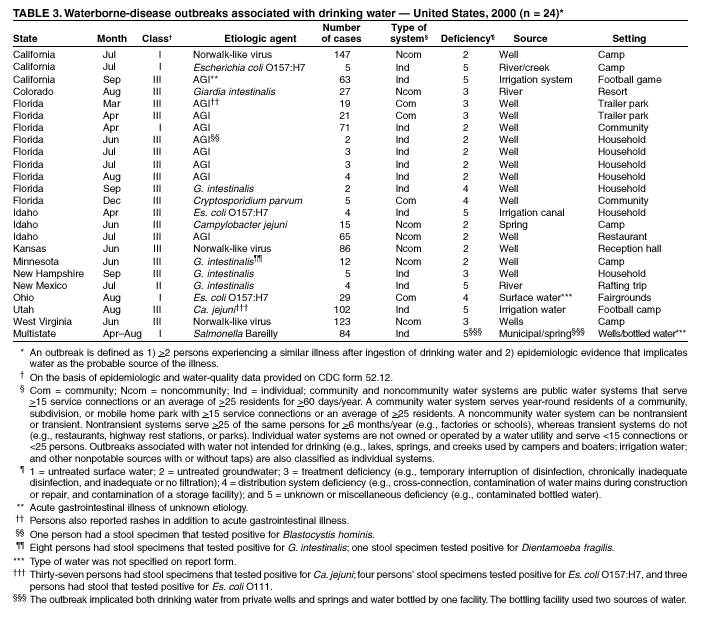
During 1999--2000, a total of 39 outbreaks associated with drinking water were reported by 25 states (see Appendix A
for selected case descriptions). One of the 39 outbreaks was a multistate outbreak of
Salmonella Bareilly that included cases
from 10 states. Of the 39 total drinking water outbreaks, 15 outbreaks were reported for 1999 and 24 for 2000. Florida
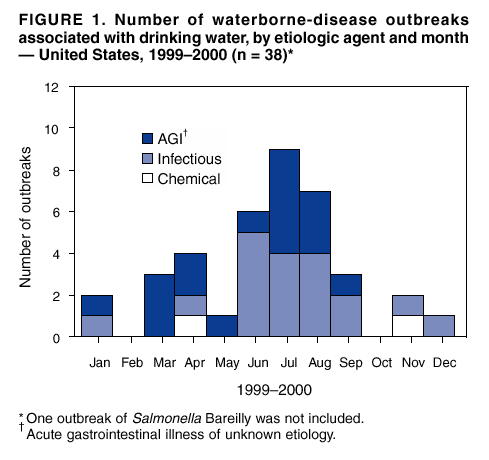
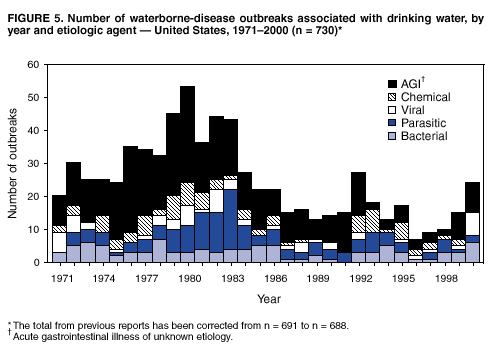
reported the most outbreaks (15) during this period. These 39 outbreaks caused illness among an estimated 2,068 persons; 122 persons were hospitalized, and two died. The median number of persons affected in an outbreak was 13.5 (range: 2--781). Outbreaks peaked during the summer months (Figure 1), June--August.
Nine of the 39 (23.1%) outbreaks were assigned to Class I on the basis of epidemiologic and water-quality data;
three (7.7%) were Class II; 25 (64.1%) were Class III; and 1 was Class IV (Table 1). One of two outbreaks associated with
a chemical etiology was not assigned a class because that outbreak was a single case of illness resulting from nitrate poisoning associated with consumption of water from a private well. Outbreaks are listed by state (Tables 2 and
3) and are tabulated by the etiologic agent, the water system type (Table
4), and by the type of deficiency and type of water system type (Table 5).
Etiologic Agents
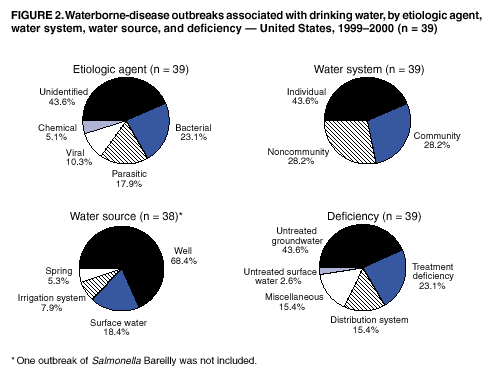
Twenty (51.3%) of the 39 outbreaks were of known infectious etiology; 17 (43.6%) were of unknown etiology; and
two (5.1%) were attributed to chemical poisoning. Of the 20 outbreaks with known infectious etiology, seven (35.0%)
were caused by parasites; nine (45.0%) were caused by bacteria; and four (20.0%) were caused by viruses (Figure 2) (Appendix A).
Parasites. Seven outbreaks affecting 57 persons were attributed to parasitic infection: six
Giardia outbreaks and one
Cryptosporidium outbreak. Six outbreaks of
Giardia associated with drinking water affected 52 persons from five states:
Florida (two outbreaks), New Mexico (one), New Hampshire (one), Minnesota (one), and Colorado (one). These outbreaks
occurred in January (one), June (one), July (one), August (one), and September (two). Four outbreaks were associated with well water
systems, and two were associated with surface water systems. Two outbreaks caused by
G. intestinalis involved possible contamination of wells by animal feces.
G. intestinalis can infect mammalian hosts, which in turn, can serve as reservoirs
for human infection. Water treatment failure was a factor in two other outbreaks of
Giardia.
Bacteria. Nine outbreaks affecting an estimated 1,166 persons were attributed to bacterial infection: four Es. coli O157: H7 outbreaks, one Campylobacter
jejuni, one Salmonella Typhimurium, one Sa. Bareilly, and two mixed Ca. jejuni and shiga toxin-producing Es.
coli (O157:H7 or O111) outbreaks. The two outbreaks with multiple pathogens caused the two
largest bacterial drinking water outbreaks reported during this study period.
Viruses. During this period, four outbreaks involving viral gastroenteritis were reported. A total of 426 persons
reported illness; no hospitalizations or deaths were reported in association with these four viral outbreaks. Three of the four outbreaks occurred in camp facilities in California, New Mexico,
and West Virginia. All three water sources were noncommunity groundwater sources.
Chemicals. During 1999, two outbreaks involving chemical contamination were reported. A total of three persons
were affected by contamination of drinking water from nitrate and sodium hydroxide.
Unidentified Etiologic Agents. Seventeen outbreaks involving gastroenteritis of unknown etiology were reported from four states, affecting an estimated 416 persons and resulting in five hospitalizations. Testing for certain enteric
pathogens (including ova and parasite testing) was attempted in five of the 17 outbreaks. In a June 2000 outbreak affecting 2 persons, stool specimens collected from one person tested negative for
G. intestinalis but positive for Blastocystis
hominis. However, whether B. hominis was the cause of the reported illness is unclear, and the pathogenicity of B. hominis has been debated in the scientific community
(26). Stool specimens were negative for parasitic and bacterial enteric pathogens in two outbreaks
in Washington (July 1999 and August 1999) and in two Florida outbreaks (March 1999 and April 2000) (Appendix A).
In addition, suspected pathogens were noted in four other outbreak reports submitted. On the basis of symptoms of illness, Norwalk-like virus (NLV) was suspected in an Idaho outbreak among firefighters that caused 65 illnesses and four hospitalizations, but the outbreak was not laboratory-confirmed.
G. intestinalis was suspected in an April 2000 outbreak in
a Florida trailer park affecting 21 persons, on the basis of the incubation period and symptoms reported. In another outbreak in a Florida trailer park in March 2000 among 19 persons, a bacterial pathogen was suspected as the cause of the outbreak on the basis of the symptoms, which included conjunctivitis and dermatitis in addition to gastroenteritis. A chemical agent
was suspected as the cause of illness among four residents in a Florida apartment building who had a cross-connection
between their drinking water and a toilet flush-valve. The residents of the apartment had noted
blue tap water before onset of illness on multiple occasions before an improper flush valve in the toilet tank was discovered.
Four outbreaks of gastroenteritis were associated with consumption of untreated water from private wells. These
four outbreaks occurred in Florida and affected 3--4 persons each. In July 2000, flooding was a possible contributor to
two outbreaks. Water in each of the homes tested positive for coliforms and did not have adequate disinfection.
Water-Quality Data
Water-quality data (i.e., information regarding the presence of coliform bacteria, pathogens, or chemical
contaminants) were available for 35 (89.7%) of the 39 drinking water outbreaks. Two reports of outbreaks of confirmed or suspected infectious etiology and two reports of outbreaks of confirmed or suspected chemical etiology did not provide water-quality data.
Of the 36 reports of outbreaks with a suspected or confirmed infectious etiology, 33 outbreaks provided water-quality data. Twenty-six (78.8%) of the 33 outbreaks with a suspected or confirmed infectious etiology reported a positive coliform,
total coliform, or fecal coliform result. Organisms also were detected in the water in two of these outbreaks. In August 2000, Ca. jejuni was detected in the water in a mixed
Ca. jejuni/Es. coli O157:H7 outbreak in Utah, although shiga toxins were
not detected. Es. coli O157:H7 was found in the water in a July 2000 California outbreak. In a 2000 Colorado outbreak,
the presence of G. intestinalis was demonstrated in a sample from the water holding tank, despite the lack of coliform data.
Of the three outbreaks with either a confirmed or suspected chemical etiology, only one demonstrated that the chemical
had been directly in the water. Tap water was tested after the health department was notified that an infant
had methemoglobinemia. Both fecal coliforms and 28 mg/L of nitrate were detected in the water. For an outbreak where
burns and gastroenteritis were reported and linked to a sodium hydroxide spill, a pH test of the water that could indicate
whether NaOH or another basic substance had spilled into the water was not documented. However, the environmental
assessment
indicated the tank contents had emptied into the water. A third suspected chemical outbreak involving a
cross-connection between a toilet flush-valve and the drinking water system did not have water-quality data available.
In 11 of the 35 outbreaks, water was not sampled for coliforms until >1 month after the first case associated with the outbreak was reported (range: 5--16 weeks). In four of these 11 outbreaks, the water samples did not test positive
for coliforms (fecal or total), chemicals, or pathogens. Instead, these were confirmed as outbreaks by epidemiologic data or
by reports that treatment deficiencies had occurred.
Water Systems and Water Sources
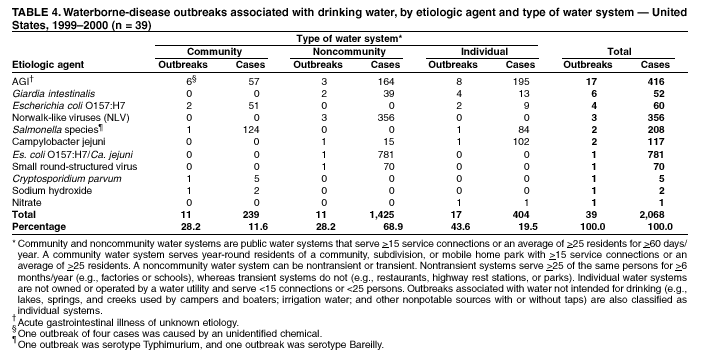
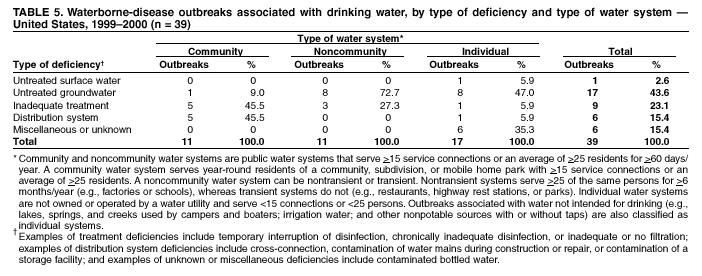
Eleven (28.2%) of the 39 drinking water outbreaks were associated with community systems, 11 (28.2%)
with noncommunity systems, and 17 (43.6%) with individual water systems (Tables 4 and
5). Ten (25.6%) of the 39
drinking water outbreaks were associated with surface water, including three outbreaks that implicated irrigation water not intended for consumption. Twenty-nine (74.4%) of the 39 drinking water outbreaks, including the outbreak associated with bottled
water, were associated with groundwater sources (wells and springs).
Five (45.5%) of the 11 outbreaks associated with community water systems were caused by treatment deficiencies;
one (9.0%) outbreak was related to contaminated, untreated groundwater, and five (45.5%) outbreaks were related to problems
in the water distribution system. Two of the five distribution system problems were related to cross-connections
between the distribution system and an irrigation well. The third outbreak related to a community water source had a household cross-connection between the toilet water and main kitchen tap. One outbreak of
Cr. parvum (Florida, December 2000) was
related to a repeated history of water main breaks. In another outbreak in Ohio in August 2000, deficiencies in the distribution system of a fairgrounds might have allowed back-siphonage of animal manure into the water used by food and beverage vendors.
Ten (90.1%) of 11 outbreaks associated with noncommunity water systems occurred in groundwater systems. Seven of
the 10 groundwater outbreaks were linked to untreated wells, and one of the 10 involved consumption of untreated spring
water. Two of the 10 outbreaks were related to treatment deficiencies in water taken from wells or a spring and were associated with outbreaks of NLV and a small round-structured virus. An outbreak associated with
G. intestinalis related to consumption of surface water occurred when a pump failure and a defective filter cartridge resulted in river water entering the drinking water holding tank without filtration. No information concerning chlorine levels from water samples was provided.
Nine (52.9%) of 17 outbreaks associated with individual water systems occurred in groundwater systems. Eight of
these groundwater systems were wells that were not treated routinely; one outbreak of giardiasis occurred when the filtration system for a well was inadvertently turned off. Five (31.3%) of the 16 outbreaks occurred when persons drank water not intended for direct consumption from irrigation systems or when they consumed surface water that had been ineffectively or
improperly treated. One (6.3%) of the 16 outbreaks in a system occurred in a home where creek water on the property was
directly consumed without treatment.
Of the nine bacterial outbreaks, four occurred in groundwater systems (one was associated with a deficiency in
the distribution system, one with a treatment deficiency, and two occurred in untreated systems). Six of seven parasitic outbreaks occurred in groundwater systems: three occurred in untreated systems; two involved problems in the distribution system; and one was related to a treatment deficiency. All four viral outbreaks occurred in noncommunity groundwater systems.
Two occurred in untreated wells, and two were related to treatment deficiencies in a spring and well. Two chemical outbreaks
were related to treatment deficiencies in well water. Fourteen of the 17 outbreaks of unknown etiology were linked to
groundwater systems. Ten of these 14 outbreaks occurred in untreated systems; two were related to distribution system problems, and two were related to treatment deficiencies.
Outbreaks Associated with Recreational Water
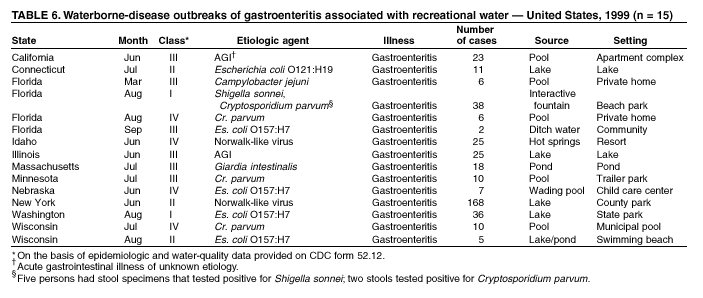
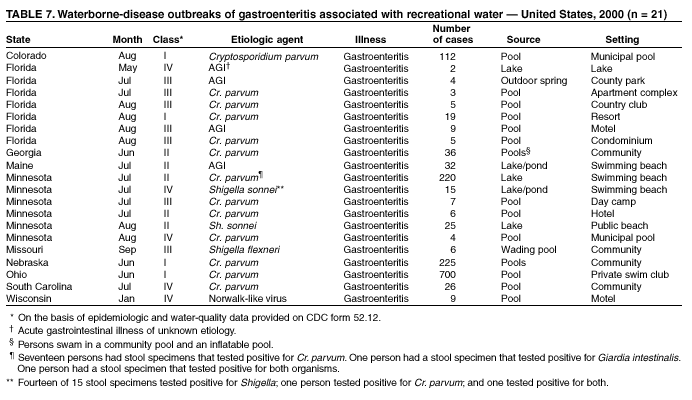
During 1999--2000, a total of 23 states reported 59 outbreaks associated with recreational water (Tables 6--9)
(see Appendix B for selected case descriptions). Twenty-three outbreaks were reported for 1999, and 36 for 2000. The states
that reported the largest number of outbreaks were Florida (14 outbreaks) and Minnesota (eight outbreaks). These 59
outbreaks affected 2,093 persons and resulted in 25 hospitalizations and four deaths. The median size of the outbreak was 10 persons (range: 1--700).
Of the 59 outbreaks, 36 were outbreaks of gastroenteritis (Tables 6 and
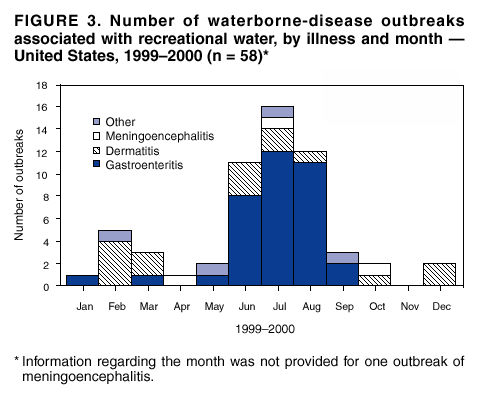
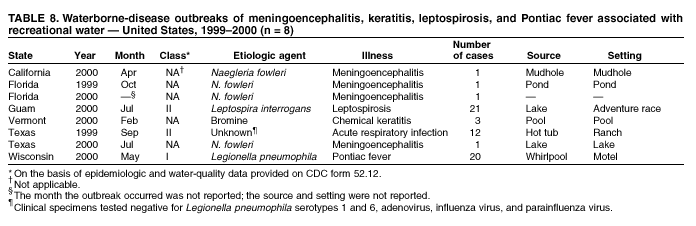
7); 15 were outbreaks of dermatitis (Table 9); four were cases of meningoencephalitis; and the remaining four outbreaks were of leptospirosis, chemical keratitis, acute respiratory infection of unknown etiology, and Pontiac fever (Table 8). Thirty-one (86.1%) of the 36 outbreaks involving gastroenteritis occurred during the summer months (i.e., June--August) (Figure 3). Outbreaks of dermatitis associated with recreational water contact were reported more frequently in February, March, June, and July. The four cases of primary amebic meningoencephalitis occurred in the warmer months (April--October).
Etiologic Agents
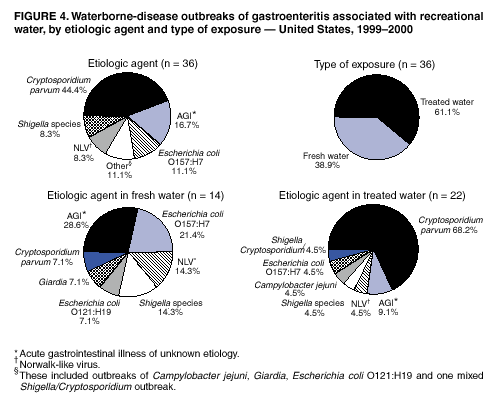
Of the 59 recreational water outbreaks, 44 (74.6%) were of known infectious etiology (Tables 6--9). Of the 36
outbreaks involving gastroenteritis, 17 (47.2%) were caused by parasites; nine (25.0%) by bacteria; three (8.3%) by viruses; one
(2.8%) by a combination of parasites and bacteria; and the remaining six (16.7%) were of unknown etiology (Figure 4).
Of the 23 nongastroenteritis-related recreational outbreaks, seven were attributed to
P. aeruginosa, four to free-living amoebae, one to
Leptospira species, one to
Legionella species, and one to bromine (Tables 8 and
9). Nine nongastroenteritis-related recreational outbreaks were of unknown etiology, eight of which were suspected but not confirmed to be caused by P. aeruginosa or schistosomes. The ninth outbreak of unknown etiology was suspected to be caused by a virus or by
Legionella pneumophila on the basis of observed symptoms and the epidemiologically implicated vehicle of transmission. Of the 59 recreational water outbreaks, 21 (35.6%) were associated with fresh or surface water, and 37 (62.7%) with treated
(e.g., chlorinated) water. Information regarding the water venue for an outbreak of meningoencephalitis was not provided.
Parasites. Sixteen of the 17 parasitic recreational water outbreaks involving gastroenteritis were caused by
Cr. parvum. The seventeenth outbreak was caused by
G. intestinalis. Fifteen of the 17 parasitic outbreaks occurred in chlorinated venues;
in these outbreaks, inadequate treatment, disrupted chlorine disinfection, or suboptimal pool maintenance were
contributing factors to the outbreaks. Cr. parvum
is highly resistant to chlorine disinfection and can survive for days in
adequately chlorinated pools; therefore, suboptimal chlorination of the pool might not be the sole factor contributing to the occurrence of an outbreak.
Three outbreaks of laboratory-confirmed cryptosporidiosis occurred during the 1999 summer swim season. During
the 2000 summer swim season, three substantial outbreaks of
Cr. parvum occurred that were related to swimming in
municipal pools. In August 2000, an outbreak occurred in Colorado that affected 112 persons attending a private pool party. In June 2000, the two other cryptosporidiosis outbreaks, one in Ohio affecting 700 persons and the other in Nebraska affecting 225 persons (27), occurred among members of private swim clubs. In both outbreaks, the protracted nature of the
outbreaks during >2 months was the result of repeated recontamination of the pools by infected persons continuing to swim; 37 (18%) of 205 persons interviewed in the Nebraska outbreak admitted to swimming while symptomatic, and 32% swam while ill
or during the 2 weeks after their illness
(27). Another outbreak (Florida, August 2000) was associated with the outbreak
that occurred in Ohio. A family who were members of the implicated swim club in the Ohio outbreak were vacationing with
a sick child. While in a pool in Florida, the infant had two fecal accidents. The resulting outbreak caused five cases of
diarrheal illness and two hospitalizations.
Eight other outbreaks of cryptosporidiosis occurred in treated venues during the 2000 swim season. Two outbreaks
of gastroenteritis occurred in untreated venues: one in a freshwater lake in Minnesota in July 2000 and one in a Massachusetts pond in July 1999 (Appendix B).
Four cases of laboratory-confirmed primary amebic meningoencephalitis attributed to
Naegleria fowleri occurred during this 2-year reporting period. All four persons were aged
<19 years. Three of the persons died from infection after having
contact with a pond, lake, or mud hole. The fourth person's freshwater exposure could not be determined; that person had fallen from a jet ski into an unspecified body of water, sustained injuries, and died from an infection shortly after it was detected.
Bacteria. Nine recreational outbreaks involving gastroenteritis were attributed to bacterial pathogens, and five of the
nine were linked to freshwater sources. Five cases
(Wisconsin, August 1999) of Es. coli O157:H7 occurred among persons
who had visited the same swimming beach. After a review of potential risk factors, the only common link found was swimming at the implicated beach. The popular beach featured a shallow, dammed area that was used for wading. Total and fecal
coliforms were detected in water samples collected before and during the outbreak, although the levels detected did not exceed levels of EPA-recommended guidelines for microbiologic quality of water
(22). One sample that was tested for Es.
coli O157:H7 was negative. Es. coli O157:H7 was implicated in another outbreak among 36 persons
(August 1999) who visited a state park in
Washington. Es. coli O121:H19 was implicated in an outbreak in a Connecticut community (July 2000).
Shigella sonnei was implicated in two outbreaks that occurred at swimming beaches in Minnesota (July and August 2000).
Nonfreshwater sources were implicated in four bacterial recreational water outbreaks involving gastroenteritis. In
March 1999, an outbreak of Ca. jejuni was associated with a private pool in Florida that did not have continuous chlorine disinfection and reportedly had ducks swimming in the pool. Outbreaks of
Shigella flexneri and Es. coli O157:H7
(Missouri, September 2000 and Nebraska, June 1999) occurred among children using unchlorinated wading pools. Fecal accidents were factors contributing to the contamination of the water in both outbreaks.
Es. coli O157:H7 also was implicated as a cause
of illness in an outbreak (Florida, September 1999) among two young children who had been playing in ditch water.
Both clinical specimens and water samples tested positive for
Es. coli O157:H7.
Two nongastroenteritis-related recreational water outbreaks were also reported. One outbreak of leptospirosis was reported among 21 persons who participated in an adventure race in Guam in July 2000 (Table 8). These persons reported
multiple outdoor exposures, including running through jungles and savannahs, swimming in a river and a reservoir, and bicycling and kayaking in the ocean. Leptospira was confirmed by serology, and an epidemiologic investigation demonstrated that swimming in the reservoir, submerging one's head in the water, and swallowing water while swimming were risk factors for illness. Water samples were not tested, and an environmental assessment of the reservoir was not conducted. The second
nongastroenteritis-related recreational water outbreak was an outbreak of Pontiac fever epidemiologically linked to use of a whirlpool at a hotel.
Viruses. During 1999--2000, three outbreaks of NLV (Calicivirus) that affected a total of 202 persons were reported.
Two NLV outbreaks occurred in untreated systems; one outbreak of NLV occurred (Idaho, June 1999) at a resort and water
park and affected 25 persons. The pool implicated in the investigation was untreated because the source of the pool's water was a natural hot springs that was high in mineral content. The investigators noted that geothermal pools used for swimming
are not required to be regulated by public health officials in that locale. The pool implicated by the investigation also had been implicated in a previous outbreak of NLV in June 1996.
Other. During 1999--2000, six recreational water outbreaks involving gastroenteritis of unknown etiology were
reported. One outbreak (Florida, August) involved a motel pool that was cloudy and dirty at the time of exposure. Nine persons who swam in this pool and did not share any other common exposure became ill with gastroenteritis. Disinfectant residuals
and operation of the filtration system at the time of the investigation were deficient. Problems were also noted with the
equipment used for adjusting pH.
Another outbreak (Florida, August 1999) among 38 persons who visited a beach park was attributed to both
Sh. sonnei and Cr. parvum (28). Illness was epidemiologically linked to playing in an interactive fountain at the park, ingesting water, and consuming food and beverages at the fountain. The fountain's recirculation, filtration, and disinfection systems were
not approved by the health department and were inadequate or not completely operational at the time of its use. Samples of the fountain water tested positive for coliforms but did not test positive for fecal coliforms. Nevertheless, the cause of
the outbreak was determined to be the fountain, which was closed until the health department's concerns could be remedied.
Three cases of chemical keratitis (Vermont, February 2000) resulted from exposure to bromine in a hotel swimming
pool. Bromine levels were >5 ppm (acceptable bromine levels are 1--3 ppm), and the pH level was >8.5. Patrons who spent time with their heads underwater with their eyes open were affected.
Twelve persons affected in an outbreak (Texas, September 1999) reported symptoms that included exhaustion, sore
muscles, headache, chills, and fever after attending a conference at a guest ranch. One woman reported a miscarriage during her illness. Exposure to a hot tub, defined as either immersion or being near the hot tub, was associated with illness. Although clinical specimens (urine, blood, sputum, and throat swabs) were tested for organisms, including
Leg. pneumophila serogroups 1 and 6, influenza virus, parainfluenza virus, and adenovirus, no infectious agent was identified. No testing for biologic or chemical agents was performed on water samples because the hot tub had already been drained, refilled, and hyperchlorinated
before the environmental investigation.
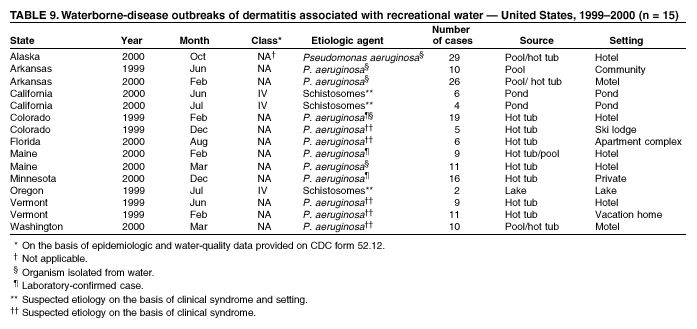
During the 1999--2000 reporting period, 15 outbreaks of dermatitis were identified (Table 9). Three of these
outbreaks were associated with swimming in freshwater and were assumed to be cercarial dermatitis caused by contact with the
larval form (cercariae) of schistosomes, which are present in freshwater environments. Two of these dermatitis outbreaks occurred in lakes in California that were associated with past cases of cercarial dermatitis. The onset of dermatitis occurred within hours after swimming in the lake and resolved after a limited number of days (median days of illness were 2 and 3 days [range: 2--3 and 3--5 days], respectively). The 12 remaining outbreaks were associated with pool and hot tub use and affected
5--29
persons each. P. aeruginosa was confirmed in clinical isolates in 3 of the 12 outbreaks and was confirmed in
water/filter samples in five outbreaks, two of which also had a clinical isolate. In eight of these outbreaks of dermatitis, specific treatment deficiencies or problems were identified. Outbreaks in Arkansas (June 1999), Florida (August 2000), Colorado
(December 1999), and Washington (March 2000) were attributed to deficiencies in treatment.
In one outbreak of dermatitis (Maine, February 2000), nine persons reported rash in addition to headache, fever,
fatigue, and sore throat (29). Swimming in the hot tub or swimming in the pool was a risk factor. The pool and hot tub were
on separate filtration systems, and both were used by the majority of persons in the outbreak. Low levels of free chlorine
were found in the pool and hot tub, but the presence of chlorinate isocyanurates (chlorine stabilizers) might have
influenced measured levels of free chlorine. A clinical isolate of
P. eruginosa was obtained from an ill person;
P. aeruginosa also was isolated from the pool filter even after the pool had been cleaned twice.
P. aeruginosa was isolated from clinical specimens and water samples in an outbreak at a Colorado hotel that affected 19 persons in February 1999 (28), 13 of whom were children aged <15 years. Symptoms were not limited to rash; they included diarrhea, vomiting, nausea, fever, fatigue, muscle aches, joint pain, swollen lymph nodes, and subcutaneous nodules on hands and feet. Because of the severity and range of symptoms, clinical specimens were examined for enteric bacterial and parasitic pathogens as well as Legionella species,
Leptospira species, and Entamoeba
histolytica but did not test positive for any of
these etiologic agents. Swabs taken from the hot tub floor and rail were positive for
P. aeruginosa and other Pseudomonas
species. Pool and hot tub records indicated that chlorine and pH had declined below the state-mandated levels at the time of exposure. Epidemiologic evidence implicated the hot tub as the likely vehicle of exposure for the outbreak. In both the Colorado outbreak and the Maine outbreak that occurred in February 2000, an offsite contractor had been engaged
to monitor disinfectant and pH levels. Insufficient communication between pool staff and the remote monitoring
company might have contributed to extended periods of usage with inadequate disinfection
(28).
Outbreaks Associated with Occupational Exposure to Water
Two outbreaks not associated with drinking or recreational water exposure were reported during this period (Table 10). One outbreak of leptospirosis (Hawaii, August 1999) occurred among persons landscaping a pond. Leptospirosis was
confirmed serologically for the two persons who had contact with the pond. Both persons reported multiple skin abrasions and were exposed to the pond water for a period of 5--10 days. One of the two persons was hospitalized.
An outbreak of acute respiratory illness occurred among sugar beet processing plant workers (Minnesota, August 2000).
Of the 15 cases identified, 13 were hospitalized. Serology for 4 (26.7%) of the 15 persons tested positive for
Leg. pneumophila; three (20.0%) persons were confirmed positive for
Leg. pneumophila by sputum polymerase chain reaction (PCR).
Fourteen (93.3%) of the 15 persons worked on a crew that had performed high-pressure cleaning in one area of the plant; the fifteenth patient had conducted high-pressure cleaning elsewhere in the plant. The sources of water for the high-pressure cleaning contained 105 colony-forming unit (CFU)/mL of
Leg. pneumophila and endotoxin levels of 22,200 endotoxin
units/mL. Although the attack rate, symptoms, and laboratory findings were consistent with an outbreak of Pontiac fever, endotoxin exposure might have contributed to this outbreak.
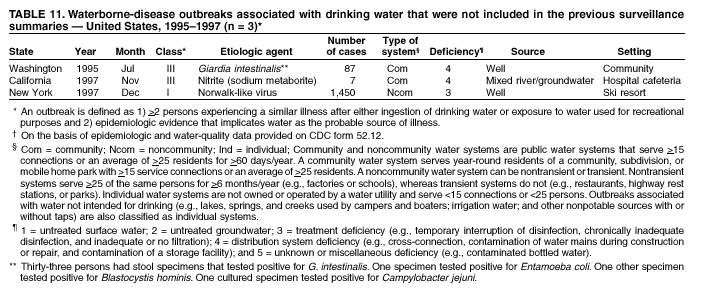
Previously Unreported Outbreaks
Three previously unreported drinking water outbreaks that occurred in 1995 and 1997 were submitted during
this reporting period (Table 11). An illegal cross-connection (Washington, July 1995) between a domestic water supply and an irrigation system at a plant nursery resulted in contamination of multiple wells in a community. Eighty-seven cases
of gastroenteritis were reported, and one hospitalization was recorded.
G. intestinalis was determined in 33 (52.4%) of 63
stool specimens; Entamoeba coli and B.
hominis were each found in one stool specimen. One (7.1%) of 14 stool specimens
that were cultured for Ca. jejuni tested positive.
NLV was implicated as the cause of an outbreak (New York, December 1997) of 1,450 cases at a restaurant at a ski resort. Epidemiologic data implicated water or consumption of ice made from water as the cause of the outbreak. The environmental assessment revealed possible problems with the well operation and location. The chlorinator for the well had been malfunctioning and had already been disconnected before the assessment. Testing of the water by the local health
department determined that neither a free nor total chlorine residual was detectable in the potable water supply and indicated the presence of fecal coliforms. In addition, the well was located <24 inches away from a stream. During the period the chlorinator was not
functioning, the pump for the well had been continuously pumping water. Surface water that might have been
introduced into the water supply, plus a deficiency in treatment of the water, played a key role in the outbreak.
Seven persons who were either employees or visitors at a hospital (California, November 1997) were symptomatic for methemoglobinemia in one outbreak. An epidemiologic investigation indicated that the only shared exposure among
these persons was a visit to the hospital cafeteria and the consumption of a carbonated beverage with ice from the self-service soda dispenser. The onset of symptoms occurred 1--5 minutes after or while drinking a carbonated beverage. One person
was hospitalized, and no deaths occurred. The environmental investigation discovered a cross-connection in the plumbing system that might have allowed water from the cooling tower, which had been recently shock-treated with sodium metaborate, to be drawn into the drinking water system. Sodium metaborate has been associated with nitrate poisoning
and methemoglobinemia in past incidents (30).
Outbreaks Not Classified as WBDOs
Outbreaks attributed to drinking water that was contaminated or potentially contaminated at the point of use rather than at the source or in the distribution system are not classified as WBDOs. Six outbreaks, causing illness among a total of
102 persons, are in this category. None of the six outbreaks reflected a common vehicle of contamination: one outbreak of
Cr. parvum was epidemiologically associated with ice consumption; a school-based outbreak of
Sh. sonnei was related to consumption of water from a dispenser stored in a bathroom facility; a third outbreak involved water taken from a garden hose (the water had been stored in an ice chest before consumption at a private residence); and a fourth outbreak
associated with bottled water that might have been contaminated at the point of use. Two of the six reported point-of-use
outbreaks involving a suspected chemical exposure occurred in food service facilities, but water testing was not performed to verify the presence of the chemical; and, because of the relatively limited number of cases associated with these incidents,
the epidemiologic information was not adequate to include these incidents as outbreaks.
Data from six other possible or confirmed outbreaks were also not included in this analysis. One confirmed outbreak
of leptospirosis was related to travel outside the United States or its territories and therefore was excluded. This outbreak occurred among student travelers who became ill after their return from Ecuador. Three cases of leptospirosis were confirmed by laboratory testing among the cohort, and four additional cases were suspected. Three other outbreaks of
G. intestinalis, Cr. parvum, and NLV could not be included in the analysis. Although these outbreaks were probably caused by a recreational water exposure, the data provided did not meet the criteria for inclusion (i.e., the outbreaks did not meet the criteria for Classes I--IV).
Two additional outbreaks were excluded because of inadequate information: one outbreak of dermatitis caused by
in-home bathing and one potential drinking water outbreak of
Cr. parvum in a New England community. This outbreak of
Cr. parvum occurred in a community near another reported community outbreak of G. intestinalis and Cr. parvum in 1999. The
pond implicated in the recreational water outbreak of
G. intestinalis also served as a surface water source, which was
intermittently mixed into the municipal drinking water that supplied the community. However, not all the persons received their
drinking water from the municipal water source. Although raw surface water samples later tested positive for
Cr. parvum by immunomagnetic spectroscopy (IMS), household water samples either tested negative, were not tested, or the results were not provided. The epidemiologic information and water-quality information provided were not conclusive.
Discussion
Considerations Regarding Reported Results
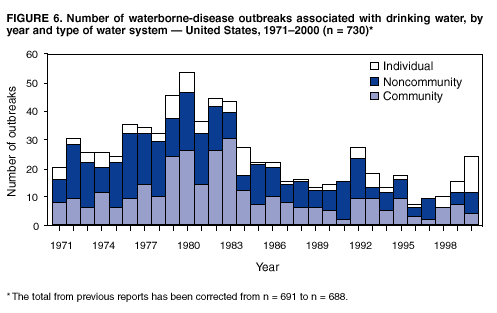
The WBDO surveillance system provides information concerning epidemiologic and etiologic trends in outbreaks. In previous years, a decrease in the number of drinking water-associated outbreaks had been observed. However, the
cumulative number of drinking water outbreaks reported for the 1999--2000 period demonstrates a reversal of this trend (Figures 5 and
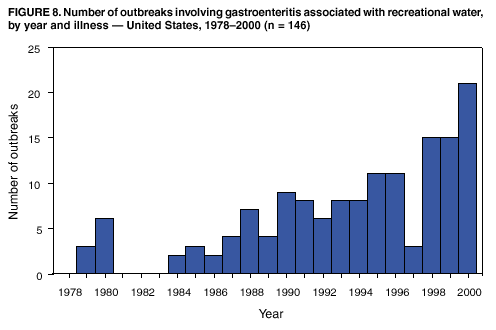
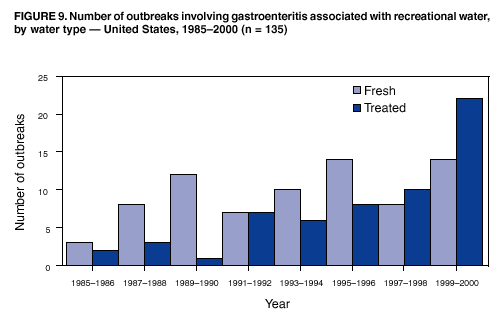
6). The number of recreational water outbreaks has been gradually increasing for the past 15 years and is at the highest level since CDC began receiving such reports in 1978.
Although the number of outbreaks reported through the surveillance system has increased, the significance of this increase
is unclear. Whether this indeed reflects a true increase in the number of outbreaks that occurred in the United States
is
unknown. Not all outbreaks are recognized, investigated, and then reported to CDC or EPA, and studies have not
been performed that assess the sensitivity of this system and indicate what percentage of actual outbreaks this system is able to detect. Multiple factors exist that can influence whether WBDOs are recognized and investigated by local, territorial, and state public health agencies: the size of the outbreak; severity of disease caused by the outbreak; public awareness of the outbreak; routine laboratory testing for organisms; requirements for reporting cases of diseases; and resources available to the local health departments for surveillance and investigation of probable outbreaks. This surveillance system probably
underreports the true number of outbreaks because of the multiple steps required before an outbreak is identified and investigated. In addition, changes in the capacity of local, county, and state public health agencies and laboratories to detect an
outbreak might influence the numbers of outbreaks reported in each state relative to other states. The states with the majority
of outbreaks reported during this period might not be the states where the majority of outbreaks actually occurred. An
increase in the number of outbreaks reported could either reflect an actual increase in outbreaks or an improved sensitivity in surveillance practices.
Recognition of WBDOs also is dependent on certain outbreak characteristics; outbreaks associated with serious illness
or affecting a substantial number of persons are more likely to receive attention from health authorities. Outbreaks involving acute diseases, including those characterized by a short incubation period, are more readily identified than
outbreaks associated with chronic, low-level exposure to an agent (e.g., certain chemicals) or are associated with organisms that have a longer incubation period (e.g., certain parasitic organisms). Outbreaks involving larger drinking water systems
(e.g., community systems) are more likely to be detected than outbreaks that involve noncommunity systems because these
systems serve mostly nonresidential areas and transient populations. Outbreaks associated with individual systems are the most likely to be underreported because they typically involve a limited number of persons. Recreational outbreaks where
persons congregate in one venue and then are geographically dispersed can be difficult to document.
The identification of the etiologic agent of a WBDO depends on the timely recognition of the outbreak so that
appropriate clinical and environmental samples can be collected. The laboratory involved in the testing of specimens must have
the capacity and capability to test for a particular organism. In certain cases, specific tests must be requested. Routine testing of stool specimens at laboratories will include tests for the presence of enteric bacterial pathogens and might also include an ova and parasite examination. However, Cr.
parvum, one of the most commonly reported waterborne parasites, is not
often included in standard ova and parasite examinations and in certain instances, must be specifically requested
(31). During 1999--2000, tests for NLV and other possible agents of viral origin were rarely performed or documented in the outbreaks that were reported to CDC. Collection of water-quality data depends primarily on local and state statutory requirements, the availability of investigative personnel, and the technical capacity of the laboratories that test the water. Furthermore, certain outbreaks can substantially alter the relative proportion of cases of waterborne disease attributed to a particular agent. The number of reported cases is typically an approximate figure, and the method and accuracy of the approximation vary
among outbreaks.
One key limitation of the data collected as part of the WBDO surveillance system is that the information collected
pertains only to outbreaks of waterborne illness. The epidemiologic trends and water-quality concerns observed in outbreaks might not necessarily reflect or correspond with trends associated with endemic waterborne illness. CDC and EPA are
collaborating on a series of epidemiologic studies to assess the magnitude of nonoutbreak waterborne illness associated with consumption
of municipal drinking water and with exposure to recreational marine and freshwaters.
Outbreaks Associated with Drinking Water
The number of outbreaks reported during 1999 (15) and 2000 (24) is higher than the number reported during 1997
(7) and 1998 (10). As described previously, the number of drinking water outbreaks had declined
(2,3). The increase in reported outbreaks should be carefully interpreted. Although the number of drinking water outbreaks has changed, the total number of persons affected by a drinking water outbreak during 1999--2000 (n = 2,027) is comparable to what was initially reported
in 1997--1998 (n = 2,038) and 1995--1996 (n = 2,567)
(2,3). Changes in surveillance and reporting of outbreaks might
have improved detection of outbreaks affecting limited, private systems that in turn, affect a relatively limited number of
persons. However, the increase in outbreaks that affect persons in limited, private systems merits further investigation by public health and water-quality agencies.
Certain states reported drinking water outbreaks for the first time in >10 years (e.g., Connecticut since 1976 or Utah
since 1986). California reported multiple drinking water outbreaks after reporting no outbreaks in 1997 and 1998, and
compared with other years during 1990--2000, the number of reported outbreaks in California increased slightly. The number
of outbreaks reported by Florida also increased. Although the numbers of reported outbreaks increased overall, the seasonality of the drinking water outbreaks is consistent with previous years, with the number peaking during the summer months.
The observed increase in the number of outbreaks is associated with an increase in outbreaks associated with consumption
of untreated water from both surface and groundwater sources, but specifically private wells.
The percentage of drinking water outbreaks associated with surface water during 1999--2000 was 17.9% (i.e.,
seven outbreaks) (Figure 2). This percentage is higher than the 11.8% reported during 1997--1998 period (i.e., two
outbreaks). However, three of the seven surface water outbreaks reported during 1999--2000 were associated with the direct ingestion of surface water without any treatment or with inadequate individual treatment. Two of these outbreaks were associated
with consumption of water during outdoor excursions where point-of-use treatment (e.g., filtration or disinfection) might have been attempted and was either inadequate to protect health or was inconsistently or incorrectly applied. The third
outbreak occurred after a household had run out of potable water and instead served untreated creek water to their guests. These three outbreaks illustrate that the public might be unaware that surface water, despite its clarity, is prone to contamination by organisms. Surface waters should not be directly consumed without being treated at the point of use or boiled.
Manufacturers of point-of-use devices and the National Sanitation Foundation (NSF) provide information regarding different devices, instructions for use, and their ability to make water safe for human
consumption.¶ The remaining four outbreaks
comprise approximately 11% of all drinking water outbreaks, an equivalent percentage to that reported in 1997--1998. These four outbreaks were associated with systems that routinely received treatment. One outbreak of giardiasis occurred at a resort (Colorado, August 2000) served by a noncommunity system. The increased demand for water during the summer,
coupled with multiple treatment failures, resulted in the delivery of unfiltered and nondisinfected water to the resort. These multiple failures illustrate the importance of routine maintenance, specifically among noncommunity systems, which do not
have consistent demand for water year-round. Two outbreaks (Florida, March 1999 and August 1999) were associated with cross-connections: one to an irrigation well and another to a toilet. Another surface water outbreak (Ohio, August 2000) at a fairgrounds was suspected to have resulted from back-siphonage into the drinking water from an animal manure site.
These outbreaks indicate that even when treatment of water at the source is adequate, deficiencies in the distribution system or
at the home can result in illness. Such deficiencies are preventable, and the public should be informed of how to detect
and avoid creating cross-connections.
Twenty-eight (71.8%) of the 39 outbreaks related to drinking water were associated with groundwater sources. This
number is an 87% increase from the number reported in the previous period (i.e., 15). Seventeen of the 28 outbreaks (60.7%)
were linked to consumption of untreated groundwater; eight of 28 (28.6%) outbreaks were associated with treatment
deficiencies; and three (10.7%) were linked to deficiencies in the distribution system. The observed pattern of deficiencies is contrary to what was observed in the previous reporting period, where the majority of groundwater outbreaks were associated
with treatment or distribution system problems. This pattern indicates that untreated groundwater systems are
increasingly associated with outbreaks of illness. Groundwater systems, with the exception of systems influenced by surface water, are not routinely required to use filtration or treatment that would be expected to reduce the number of pathogens in the water.
EPA's pending GWR** is expected to establish multiple barriers in groundwater systems to protect against bacteria and viruses in drinking water from groundwater sources and should establish a targeted strategy to identify groundwater systems at high risk for fecal contamination.
Twenty-six of these 28 groundwater outbreaks had a well as the implicated water source, and two were linked to a
spring. The percentages of outbreaks associated with wells and springs were similar during this reporting period to the 1997--1998 period. Although GWR is expected to have public health benefits, these protections extend primarily to
community groundwater systems. Of the 26 well-related outbreaks that occurred during the 1999--2000 period, only eight of 26 were associated with community wells. Ten were associated with individual private wells, and eight were associated
with noncommunity wells. These systems would not necessarily benefit from the promulgation of GWR, and therefore, the
quality of water in wells remains a public health concern. Approximately 14--15 million households in the United States rely on a private, household well for drinking water each year, and >90,000 new wells are drilled throughout the United States
each year (32). In addition, contamination of a private well is not only a health concern for the household served by the well,
but
can impact households using other nearby water supplies and could potentially contaminate the
aquifer.†† Additional education efforts should be targeted towards well owners, users, well drillers, and local and state drinking water personnel to encourage practices that best ensure safe drinking water for private well users.
Three outbreaks were associated with direct consumption of water from irrigation systems, comprising approximately
8% of drinking water outbreaks (Figure 2).
Cross-connections to irrigation systems were implicated as contaminating factors in
three other irrigation-related outbreaks. Irrigation waters are not regulated under the Safe Drinking Water Act, because they
are typically intended for agricultural purposes, not for human consumption. Therefore, irrigation water would not be
expected to be treated to reduce the level of microorganisms or other contaminants potentially in the water to the same standards
as water intended for consumption. In one outbreak, children drank directly from an irrigation canal while playing outside a home. In two other outbreaks, water was directly consumed from an irrigation tap by sports team members. In the
first instance, the sports team consumed water from a labeled irrigation tap despite being informed that the water was not intended for consumption. In the second instance, two teams drank from taps on the field because no other source of potable water was available on field.
The multistate outbreak of Sa. Bareilly, which was detected through CDC's
Salmonella Outbreak Surveillance Algorithm (SODA), epidemiologically implicated the consumption of bottled water as a risk factor for illness. This is the first widespread outbreak implicating bottled water in the United States. Previous bottled water outbreaks occurred in New
Jersey in 1973 (33), Pennsylvania in 1980
(34), and in the Northern Mariana Islands in 1993
(4). Bottled water standards and regulations, unlike the majority of drinking water standards, are not set and enforced by EPA but by FDA. FDA regulates bottled water as a packaged food product and bases their bottled water standards on EPA's tap water standards. In
addition, bottled water might be subject to state and voluntary industry regulation. Bottled water, before this outbreak, had not been identified as a vehicle for transmission of infectious organisms in the United States, although a bottled water outbreak of Ca. jejuni associated with consumption of water bottled in Greece was documented during the 1997--1998 surveillance
period (2). Because of the wide geographic distribution of bottled water products, an outbreak associated with the consumption of bottled water would be difficult to recognize. FDA, EPA, CDC, and the bottled water industry together should
address concerns regarding consumption of bottled water and public health.
Overall, the number of outbreaks associated with the five drinking water deficiencies (untreated surface water,
untreated groundwater, treatment deficiency, distribution system deficiency, and unknown/miscellaneous deficiency) increased in
each category from the 1997--1998 levels. The percentage of outbreaks caused by a treatment deficiency and distribution
system problem decreased relative to reported increases in the other three categories. Although problems with treatment and with distribution systems remain critical concerns for safe drinking water, the public's lack of understanding of the risk associated with consumption of untreated water and the assumption that all water is suitable for consumption is a concern also.
The relative proportion and number of outbreaks associated with different water systems also differs from the figures
from the 1997--1998 period (Figure 2). Outbreaks in community systems increased from 8 to 11 outbreaks (37.5%
increase); noncommunity outbreaks doubled from 5 to 11; and individual system outbreaks quadrupled, increasing from 4 to 17 outbreaks. However, the proportion of outbreaks in community systems decreased from 47.1% during 1997--1998 to
28.2% during 1999--2000, whereas the relative proportion of outbreaks in individual systems increased from 23.5% during 1997--1998 to 43.6 during 1999--2000. In addition, the number of outbreaks reported that were associated with individual systems during this period is the highest reported level since 1984. The drinking water quality of community systems, which typically have been the focus of increased EPA regulation, has continually improved. But noncommunity systems and individual systems, which are not regulated to the same extent, are continuing problems. The majority of these individual
system outbreaks are linked to currently unregulated groundwater supplies, specifically private wells. The populations served by these systems merit increased attention by public health officials.
The etiologic agent was not identified in 17 (43.6%) of 39 outbreaks (Figure 2). These outbreaks of unknown
etiology comprised the largest group of outbreaks, followed by outbreaks caused by bacteria (nine), parasites (seven), viruses (four), and chemicals (two). During 1997--1998, parasites accounted for the largest percentage of the 17 outbreaks (six [35.3%]), followed by unidentified pathogens (five [29.4%]), bacteria (four [23.5%]), chemicals (two [11.6%]), and viruses (zero [0%]). The number of outbreaks per type of agent were increased for all categories during 1999--2000, with the exception
of chemicals. Although the number of reported viral outbreaks increased, indicating an improvement in the availability
and usage of laboratory detection methods during previous years, viral outbreaks are probably substantially
underreported.
Although viruses were suspected in other outbreaks, specifically in those of unknown etiology, testing for viruses was
not performed. The technology for detection of viruses in stool and water samples has improved, but testing for viruses is not widely practiced. Investigators are encouraged to submit clinical specimens to CDC or state laboratories that conduct these tests. Guidelines for collecting stool specimens for identification of viral organisms are available from CDC (35). Investigators are also encouraged to contact CDC and EPA regarding testing of water samples.
Only two outbreaks of chemical origin were identified during this surveillance period, the same number as was
reported during the 1997--1998 period. One outbreak related to a spill of sodium hydroxide at a community water treatment plant demonstrated the need for safe water treatment practices. The other outbreak was a single case of methemoglobinemia in an infant who required hospitalization after having been fed boiled water taken from a private well. Coordination of
public health messages is critical; an intervention that was intended to reduce the transmission of infections agents concentrated the chemicals present in the water. These figures, as in the past, probably underrepresent the actual waterborne
chemical poisonings that occur. Multiple factors can explain the low reporting rate, including the likelihood that 1) the majority of waterborne chemical poisonings typically occur in private residences and affect a relatively limited number of persons;
2) exposures to chemicals through drinking water might cause illness that is difficult to link to a chemical exposure; 3)
the mechanisms for reporting waterborne chemical poisonings to the WBDO surveillance system are not as established
for chemicals as they are for WBDOs attributed to infectious agents; and 4) health-care providers and those affected might not as easily recognize chemical poisonings. As a result of these factors, WBDOs of chemical poisonings are less likely to be reported to public health officials.
Strengthening the capacity of local and state public health epidemiologists and environmental health specialists to
detect and investigate outbreaks remains a priority at CDC and EPA. As part of that effort, CDC and EPA should partner with the states, CSTE, and the Association of Public Health Laboratories to develop training materials and online resources that would be useful and easily accessible to local and state public health personnel. Although no federal regulation exists for
monitoring private wells, developing educational materials targeted towards the general public, informing them of ways to maintain the safety and water quality of their wells would be valuable. In addition, health messages regarding the consumption
of nonpotable water and appropriate point-of-use treatment should be developed and distributed to the public.
Outbreaks Associated with Recreational Water
Of the 59 recreational WBDOs, those involving gastroenteritis were most frequently reported (n = 36). The 15
outbreaks reported in 1999 and 21 outbreaks reported in 2000 equal or surpass the number reported in 1998, which previously was the highest number of outbreaks involving recreational water-related gastroenteritis reported in one year since the inception of the surveillance system. Together, the outbreaks involving gastroenteritis reported during the 1999--2000 period are higher
than the 18 outbreaks documented in the previous reporting period (Figures 7 and
8). Since 1989, the number of gastroenteritis-related outbreaks has been gradually increasing, and this increase is statistically significant (p = 0.01).
Because swimming is essentially a shared water activity or communal bathing, rinsing of soiled bodies and overt
fecal accidents cause contamination of the water. Unintentional ingestion of recreational water contaminated with pathogens can then lead to gastrointestinal illness, even in nonoutbreak settings
(36,37). Fresh and marine waters are also subject to
other modes of contamination from point sources (i.e., sewage releases), watersheds (i.e., runoff from agriculture and residential areas), and floods.
Outbreaks involving gastroenteritis are more frequently observed during the swimming season, which usually starts
on Memorial Day weekend (the last weekend in May) and ends Labor Day weekend (the first weekend in September).
However, swimming also occurs year-round in indoor venues and in states with more temperate climates. Outbreaks of illness by month (Figure 3) include two outbreaks that occurred noticeably outside the summer months: one outbreak in a Florida pool
in March and another outbreak in an indoor pool in Wisconsin in January.
As during the previous reporting period, Cr.
parvum accounted for the largest percentage of outbreaks involving gastroenteritis (44.4%), followed by Es. coli O157:H7 (11.1%), NLV (8.3%), and
Shigella (8.3%). An outbreak of G.
intestinalis was also reported in 1999. The last reported recreational water outbreak of Giardia occurred in 1996. Outbreaks of Ca.
jejuni, Es. coli O121:H19, and a mixed
Sh. sonnei/Cr. parvum outbreak were also reported for the first time to
the surveillance system. Outbreaks of unknown etiology comprised 16.7% of the recreational water outbreaks
involving gastroenteritis.
Twenty-two (61.1%) of the 36 outbreaks of gastroenteritis occurred in treated systems (i.e., pools) that would usually be expected to be chlorinated or disinfected to prevent transmission of infectious agents after unintentional ingestion.
However, the term treated system might pertain to systems not routinely treated, including wading pools, interactive fountains, and in one case, an untreated pool that was served by a natural hot springs source. Multiple interrelated factors can
impede disinfection in treated venues, including an increased bather load in a pool, high levels of organic material (e.g., fecal
material or environmental or skin debris) and ultraviolet light, all of which deplete chlorine residuals that usually maintain protection in the system. In certain outbreaks, fecal material was indicated on the report as a contributing factor to the outbreak; the majority of fecal accidents were attributed to young children who were in or near the water at the time the accident occurred.
Unlike previous years, a substantial number of different bacterial and viral organisms were reported as
causing gastrointestinal illness in these treated recreational water venues (Figure 9). Nevertheless, >66% of these outbreaks were attributed to Cr. parvum (Figure 4). Unlike other organisms, which are more susceptible to the levels of chlorine
typically found in a pool, Cr. parvum is highly chlorine-resistant and requires increased levels of chlorine and longer contact times with chlorine for inactivation. Cr. parvum can survive for days in public health-mandated chlorine concentrations required
for pools. In addition, its relatively limited size (4--6 µm) can allow it to pass through particulate filtration systems during recirculation of water in the pool. Because a low number of oocysts might cause illness in a person, even ingestion of a limited amount of water can cause infection. Although the number of
Cr. parvum outbreaks has been steadily increasing during
1990--2000, multiple explanations could exist for the increase. The properties of the organism, coupled with the popularity of swimming and the tendency of persons to aggregate in larger water venues, increases the likelihood that swimming water can become contaminated and that swimmers will ingest the water and become infected. However, the increases in
outbreaks could be explained by a higher awareness of
Cr. parvum as a potential cause of illness among swimmers by the public
health community and the recreational water industry and, as a result, are more likely to be detected.
The majority of these Cr. parvum outbreak investigations noted inadequate pool maintenance. Although low chlorine
levels are unlikely to have been the cause of the outbreaks, the frequent reporting of low chlorine levels in these outbreaks indicates a disturbing lack of awareness concerning the role of chlorine and pH control as the major protective barrier against
infectious disease transmission in pools. Inadequate disinfectant levels in any pool increases the risk for transmission of chlorine-sensitive pathogens (e.g., Es.
coli O157:H7 or Shigella species) if an infected swimmer contaminates the pool. Pool
operators and staff should be appropriately trained regarding the spread of recreational water illnesses and the critical role of pool maintenance (i.e., disinfection, pH control, and filtration) in preventing
WBDOs.§§
Fourteen outbreaks involving gastroenteritis after freshwater exposure were reported during 1999--2000, compared
with eight during 1997--1998. Es. coli O157:H7 accounted for the most outbreaks of known etiology (three), followed by
NLV (two), Shigella species (two), Es.
coli O121:H19 (one), G. intestinalis (one), and
Cr. parvum (one). Four outbreaks were of unknown etiology. Certain outbreaks occurred in beach areas that had substantial numbers of families bathing and swimming in the water. Again, a common element noted in these reports was the presence of diaper-aged children in the water,
diaper-changing on the beach, and even washing off young children in the water. One incident involved persons who swam in a lake that was had posted signs indicating that the lake was unsafe for swimming.
Reports of infants and children swimming when they have diarrhea is a problem common to both freshwater systems
and treated venues. Although health communication messages have been targeted in the past for treated venues, similar messages should be provided to those who swimming in freshwater venues. EPA, as part of the Beaches Action Plan, is developing guidelines and information for users of
freshwaters.¶¶ Geothermal pools and hot springs should be examined closely. In
one outbreak, pools in a complex were exempt from public health regulation because they were naturally occurring hot
springs and mineral waters. Hot springs, which feature high levels of minerals and elevated temperatures, are potentially ideal venues for microbial growth or contamination. These springs and geothermal pools pose an increased risk to swimmers,
compared with treated pools because of their lack of disinfection and filtration. Improved consumer and staff education and supplementary treatment might be necessary to prevent future outbreaks in these enclosed freshwater pools.
Twelve of the 15 outbreaks of dermatitis were associated with hot tub or pool use. The majority of these reports
of dermatitis are associated with deficient maintenance and inadequate disinfection of the water. The higher
temperatures commonly found in hot tubs deplete disinfectant levels at a more rapid rate; hot tub operators should be encouraged to actively check and maintain adequate disinfectant levels. In addition to rashes, reports have been received of other
symptoms. In Alaska, three of 29 persons reported nausea. In the two Maine outbreaks, persons also reported headache, fatigue, and
other
symptoms. The Colorado outbreak was notable for its severe symptomatology and an extended duration of illness.
Extended and painful rashes associated with P. aeruginosa
outbreaks are unusual but have been documented
(38,39). One report (39) also indicates that a substantial number of children are being affected by these outbreaks. In the Colorado outbreak of P. aeruginosa, the persons affected were primarily children, but no indication was provided that age was a risk factor
for infection. More remarkable is the observed duration of illness. Certain persons reported chronic illness (i.e., rash, joint pain, abdominal pain, and chest pain) that lasted
>6 weeks. Using remote pool monitoring services in two of these
outbreaks underscores the need for training pool staff regarding the role of monitoring service and prompt communication between service and pool operators when problems are detected.
Three outbreaks of dermatitis that occurred after persons swam in fresh or marine water were presumed to be caused by
an allergic reaction to the cercariae, the larval form of certain nonhuman species of schistosomes. Cercarial dermatitis was
an identified problem in two of these lakes, and signs posted by the health department regarding this problem were ignored
by swimmers. The extent of the problem of cercarial dermatitis caused by freshwater exposure is unknown, although it
probably occurs more frequently than what is reported to the surveillance system. As schistosomes occur naturally in ecosystems that bring snails and birds or aquatic mammals close together, a substantial number of freshwater lakes in the United States might cause illness among swimmers. Swimmers should pay careful attention to where they swim, avoid shallow swimming
areas known to be appropriate snail habitats in lakes associated with cercarial dermatitis, and report any incidents to their local health department to prevent further illnesses.
The four deaths associated with primary amebic meningoencephalitis (PAM) reported during the 1999--2000 period
were all linked to freshwater exposure. Typically, these cases are associated with swimming in freshwater bodies in the late summer months because N. fowleri, which has been implicated in >90% of the cases reported to CDC, proliferate in warm, stagnant waters. Previous cases of PAM have been reported from states with more temperate climates (e.g., California, Florida, and Texas) or from areas with hot springs. The amoebas associated with PAM are believed to enter through the nasal
passage. Preventing forceful entry of water up the nasal passages during jumping or diving by holding one's nose or wearing nose plugs could reduce the risk for infection.
Swimming in waters contaminated by animal urine was the likely explanation for an outbreak of leptospirosis
among persons participating in an adventure race in Guam.
Leptospira species can be found frequently in wild animal urine, and
can be contracted through inhalation of aerosolized water or ingestion of water while swimming. Leptospirosis can also
be acquired through abrasions. In this instance, the exposure was associated with immersion of persons' heads in a body of
water while they swam and swallowed water. Although outdoor swimming is not necessarily dangerous, swimmers should
be educated regarding the potential risks resulting from swimming in areas that are not secured from wild animal use.
An increased level of bromine, which is used to disinfect pools and hot tubs, caused certain cases of chemical
keratitis. Inadequate disinfection of a whirlpool resulted in an outbreak of legionellosis among 20 persons who stayed at a motel. Safe disinfection practices and appropriate pool maintenance protocols should be communicated to operators and managers
of facilities that treat recreational water.
Outbreaks Associated with Occupational Exposures to Water
Two outbreaks that do not fit into the previous categories were reported to CDC by Minnesota and Hawaii.
Outbreaks associated with exposure to aerosolized water have previously occurred but have not been reported to the WBDO
surveillance system (40,41). These outbreaks are discussed in this report to demonstrate that water exposures are not limited to ingestion and contact (e.g., through swimming), and these outbreaks are preventable. Using barrier masks to prevent inhalation
of aerosolized water or disinfection of water that is not being used for drinking or swimming purposes could have prevented
the respiratory illnesses associated with these two outbreaks.
Conclusion
Data collected as part of the national WBDO surveillance system are used to describe the epidemiology of
waterborne diseases in the United States. Data regarding water systems and deficiencies implicated in these outbreaks are used to assess whether regulations for water treatment and monitoring of water quality are adequate to protect the public's
health.
Identification of the etiologic agents responsible for these outbreaks is also critical because new trends might
necessitate different interventions and changes in policies and resource allotment.
Surveillance for waterborne agents and outbreaks occurs primarily at the local and state level. Local and state public
health agencies need to detect and recognize WBDOs and implement appropriate prevention and control measures.
Improved communication among local and state public health departments, regulatory agencies, water utilities, and recreational water facilities would aide the detection and control of outbreaks. Routine reporting or sharing of water-quality data with the health department is recommended. Other means of improving surveillance at the local, state, and federal level could include the additional review and follow-up of information gathered through other mechanisms (e.g., issuances of boil-water advisories or reports of illness associated with agents thought to be waterborne).
One repeated observation regarding outbreak data collected as part of the WBDO system was that the timely collection
of clinical specimens and water samples for testing and commencement of an environmental investigation would have resulted
in an improved ability to detect the outbreak's etiologic agent and the source of water contamination. However, the course of an investigation is influenced by the ability and capacity of public health departments and laboratories to recognize
and investigate potential outbreaks of illness. Even when personnel are available to investigate a potential outbreak in a timely manner, a common observation is that investigations cannot always be completed thoroughly. WBDO outbreak
investigations typically require input from different disciplines, including infectious disease epidemiology, environmental
epidemiology, clinical medicine, sanitation, water engineering, and microbiology. Either further cross-training of existing personnel needs to be implemented or additional personnel and resources need to be made available or linked to those who typically
investigate reports of WBDOs.
State health departments can request epidemiologic assistance and laboratory testing from CDC to investigate
WBDOs. CDC and EPA can be consulted regarding engineering and environmental aspects of drinking water and recreational
water treatment and regarding collection of large-volume water samples to identify pathogenic viruses and parasites, which require special protocols for their recovery. Requests for tests for viral organisms should be made to CDC's Viral Gastroenteritis Section, Respiratory and Enterovirus Branch, Division of Viral and Rickettsial Diseases, National Center for Infectious Diseases (NCID), at 404-639-3577. Requests for tests for parasites should be made to CDC's Division of Parasitic Diseases, NCID, at 770-488-7760.
Additional information is available from
EPA's Safe Drinking Water Hotline at 800-426-4791, on the Internet at
http://www.epa.gov/safewater, or by e-mail at hotline-sdwa@epa.gov;
CDC's Healthy Swimming website at
http://ww.cdc.gov/healthyswimming; includes recreational water
health communication materials for the general public and pool maintenance staff (e.g., information regarding disinfection, guidelines on response to fecal accidents
[42], fact sheets concerning recreational water illnesses), and an
outbreak investigation toolkit that can be used by public health professionals;
CDC's Voice and Fax Information System, 888-232-3228 (voice) or 888-232-3299 (fax). Choose cryptosporidiosis in
the disease category; and
for reporting WBDOs, CDC's Division of Parasitic Diseases, NCID, at 770-488-7760 or by fax at 770-488-7761.
Acknowledgments
The authors thank the following persons for their contributions to this report: state waterborne-disease surveillance coordinators; state epidemiologists; state drinking water administrators; Susan Shaw, M.S., M.P.H., Office of Ground Water and Drinking Water,
EPA; Robert Tauxe, M.D., Division of Bacterial and Mycotic Diseases, NCID, CDC; Roger Glass, M.D., Ph.D., Steve Monroe, Ph.D., and Marc-Alain Widdowson, M.A., Vet.M.B., M.Sc., Division of Viral and Rickettsial Diseases, NCID, CDC; Matthew Arduino, Dr.P.H. and Joe Carpenter, Division of Healthcare Quality and Promotion, NCID, CDC; Mark Eberhard, Ph.D., Mary Bartlett, Ali Khan, M.D., James Maguire, M.D., and Dennis Juranek, D.V.M., Division of Parasitic Diseases, NCID, CDC; and Lorraine Backer, Ph.D., Division of Environmental Hazards and Health Effects, National Center for Environmental Health, CDC.
References
Craun GF, ed. Waterborne diseases in the United States. Boca Raton, FL: CRC Press, Inc., 1986.
Environmental Protection Agency. 40 CFR Part 141. Water programs: national interim primary drinking water regulations. Federal
Register 1975;40:59566--74.
Pontius FW, Roberson JA. Current regulatory agenda: an update. Journal of the American Water Works Association 1994;86:54--63.
Pontius FW. Implementing the 1996 SDWA amendments. Journal of the American Water Works Association 1997;89:18--36.
Environmental Protection Agency. Announcement of the drinking water contaminant candidate list; notice. Federal Register 1998;63:10274--87.
Environmental Protection Agency. 40 CFR Parts 141 and 142. Drinking water; national primary drinking water regulations; filtration,
disinfection; turbidity, Giardia lamblia, viruses,
Legionella, and heterotrophic bacteria; final rule. Federal Register 1989;54:27486--541.
Environmental Protection Agency. 40 CFR Parts 141 and 142. Drinking water; national primary drinking water regulations; total
coliforms (including fecal coliforms and E.
coli); final rule. Federal Register 1989;54:27544--68.
Environmental Protection Agency. 40 CFR Parts 141 and 142. Drinking water; national primary drinking water regulations; total
coliforms; corrections and technical amendments; final rule. Federal Register 1990;55:25064--5.
Environmental Protection Agency. 40 CFR Parts 9, 141, and 142. National primary drinking water regulations: interim enhanced surface
water treatment; final rule. Federal Register 1998;63:69477--521.
Environmental Protection Agency. 40 CFR Parts 9, 141, and 142. National primary drinking water regulations: long term 1 enhanced
surface water treatment rule; final rule. Federal Register 2002;67:1812--44.
Environmental Protection Agency. 40 CFR Parts 9, 141, and 142. National primary drinking water regulations: long term 1 enhanced surface
water treatment and filter backwash rule; proposed rule. Federal Register 2000;67:19046--150.
Environmental Protection Agency. 40 CFR Parts 9, 141, and 142, National primary drinking water regulations: filter backwash recycling rule;
final rule. Federal Register 2001;66:31085--105.
Environmental Protection Agency. 40 CFR Parts 141 and 141. National primary drinking water regulations: ground water rule; proposed
rules. Federal Register 2000;65:30193--274.
Environmental Protection Agency. 40 CFR Parts 9, 144, 145, and 146. Underground injection control regulations for class V injection
wells, revision; final rule. Federal Register 1999;64:68545--73.
Environmental Protection Agency. 40 CFR Part 141. National primary drinking water regulations: monitoring requirements for public
drinking water supplies; final rule. Federal Register 1996;61:24353--88.
Environmental Protection Agency, 40 CFR Parts 9, 141, and 142. National primary drinking water regulations for lead and copper. Final
rule. Federal Register 2000;65:1949--2015.
US Environmental Protection Agency, Office of Water. Ambient water quality criteria for bacteria---1986. Cincinnati, OH: National Service
Center for Environmental Publications, 1986. EPA publication no. 440584002.
Dufour AP. Health effects criteria for fresh recreational waters. Research Triangle Park, NC: US Environmental Protection Agency, Office
of Research and Development, Health Effects Research Laboratory, 1984; EPA publication no. 600184004.
US Environmental Protection Agency, Office of Water. Factoids: drinking water and ground water statistics for 2000. Washington, DC:
US Environmental Protection Agency, Office of Water, 2001. EPA publication no. 816K01004. Available at
http://www.epa.gov/cgi-bin/claritgw.
US Environmental Protection Agency. EPA safe drinking water information system factoids: FY 1999 inventory data. Washington, DC:
US Environmental Protection Agency, 2002. Available at
http://www.epa.gov/safewater/data/99factoids.pdf.
Anonymous. Blastocystis
hominis: a new pathogen in day-care centers? Can Commun Dis Rep 2001;27:76--84.
Jones JL, Lopez A, Wahlquist SP, Nadle J, Wilson M. Survey of clinical laboratory practices, parasitic diseases. Clinical Infectious Diseases (in press).
US General Accounting Office. Drinking water: information on the quality of water found at community water systems and private
wells. Washington, DC: US General Accounting Office, 1997. GAO publication no. GAO/RCED-97-123.
CDC. Foodborne & waterborne disease outbreaks [Annual summary 1973]. Atlanta, GA: US Department of Health, Education, and
Welfare, CDC, 1974. Publication no. 76-8185.
CDC. Water-related outbreaks [Annual summary 1980]. Atlanta, GA: US Department of Health and Human Services, CDC, 1981. Publication
no. 82-8385.
Calderon RL, Mood EW, Dufour AP. Health effects of swimmers and nonpoint sources of contaminated water. International Journal
of Environmental Health Research 1991;1:21--31.
Seyfried PL, Tobin RS, Brown NE, Ness PF. Prospective study of swimming-related illness. I. Swimming-associated health risk. Am J Public
Health 1985;75:1068--70.
Berrouane YF, McNutt LA, Buschelman BJ, et al. Outbreak of severe
Pseudomonas aeruginosa infections caused by a contaminated drain in
a whirlpool bathtub. Clin Infect Dis 2000;31:1331--7.
Fiorillo LM, Zucker M, Sawyer D, Lin AN.
Pseudomonas hot-foot syndrome. N Engl J Med 2001;345:335--8.
* Total coliforms are considered indicator organisms that typically do not cause disease but might be associated with the presence of other disease-causing organisms. Additional information regarding total coliforms is available at
http://www.epa.gov/safewater/dwa/electronic/tcr.pdf.
† Additional information is available at
http://www.cleanwater.gov. § Additional terms are defined in the glossary. ¶ Additional information is available at
http://www.nsf.org.
** Additional information is available at
http://www.epa.gov/safewater/gwr.html.
†† Although EPA does not regulate private wells and will not regulate them as part of the proposed GWR, EPA lists recommendations
for protecting private water supplies at
http://www.epa.gov/safewater/pwells1.html and provides links to other sources of information.
§§ Guidelines for pool operators and other information related to recreational water illnesses is available at
http://www.cdc.gov/healthyswimming.
¶¶ Additional information is available at
http://www.epa.gov/waterscience/beaches.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
Disclaimer
All MMWR HTML versions of articles are electronic conversions from ASCII text
into HTML. This conversion may have resulted in character translation or format errors in the HTML version.
Users should not rely on this HTML document, but are referred to the electronic PDF version and/or
the original MMWR paper copy for the official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents,
U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800.
Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.