Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail.
Prevention of Herpes Zoster
Recommendations of the Advisory Committee on Immunization
Practices (ACIP)
NOTE: A Continuing Education Activity has been
approved for this report and will be included in the print and
electronic format on June 06, 2008, in Vol. 57, No. RR-5. The credits
awarded are as follows: CME, 2.75; CNE, 2.75; CEU, .25; and CHES, 3.0.
Prepared by
Rafael Harpaz, MD, Ismael R. Ortega-Sanchez, PhD, Jane F. Seward, MBBS,
Division of Viral Diseases, National Center for Immunization and Respiratory Diseases
The material in this report originated in the National Center for Immunization and Respiratory Diseases, Anne Schuchat, MD, Director; and the
Division of Viral Diseases, Larry Anderson, MD, Director.
Corresponding preparer: Rafael Harpaz, MD, National Center for Immunization and Respiratory Diseases, CDC, 1600 Clifton Rd., NE, MS
A-47, Atlanta, GA 30333. Telephone: 404-639-6284; Fax:
404-639-8665; E-mail: rzh6@cdc.gov.
Summary
These recommendations represent the first statement by the Advisory Committee on Immunization Practices (ACIP)
on the use of a live attenuated vaccine for the prevention of herpes zoster (zoster) (i.e., shingles) and its sequelae, which
was licensed by the U.S. Food and Drug Administration (FDA) on May 25, 2006. This report summarizes the
epidemiology of zoster and its sequelae, describes the zoster vaccine, and provides recommendations for its use among adults aged
>60 years in the United States.
Zoster is a localized, generally painful cutaneous eruption that occurs most frequently among older adults
and immunocompromised persons. It is caused by reactivation of latent varicella zoster virus (VZV) decades after initial
VZV infection is established. Approximately one in three persons will develop zoster during their lifetime, resulting in
an estimated 1 million episodes in the United States annually. A common complication of zoster is postherpetic
neuralgia (PHN), a chronic, often debilitating pain condition that can last months or even years. The risk for PHN in patients
with zoster is 10%--18%. Another complication of zoster is eye involvement, which occurs in 10%--25% of zoster episodes
and can result in prolonged or permanent pain, facial scarring, and loss of vision. Approximately 3% of patients with
zoster are hospitalized; many of these episodes involved persons with one or more immunocompromising conditions.
Deaths attributable to zoster are uncommon among persons who are not immunocompromised.
Prompt treatment with the oral antiviral agents acyclovir, valacyclovir, and famciclovir decreases the severity
and duration of acute pain from zoster. Additional pain control can be achieved in certain patients by supplementing
antiviral agents with corticosteroids and with analgesics. Established PHN can be managed in certain patients with
analgesics, tricyclic antidepressants, and other agents.
Licensed zoster vaccine is a lyophilized preparation of a live, attenuated strain of VZV, the same strain used in
the varicella vaccines. However, its minimum potency is at least 14-times the potency of single-antigen varicella vaccine. In
a large clinical trial, zoster vaccine was partially efficacious at preventing zoster. It also was partially efficacious at
reducing the severity and duration of pain and at preventing PHN among those developing zoster.
Zoster vaccine is recommended for all persons aged
>60 years who have no contraindications, including persons
who report a previous episode of zoster or who have chronic medical conditions. The vaccine should be offered at the
patient's first clinical encounter with his or her health-care provider. It is administered as a single 0.65 mL dose subcutaneously
in the deltoid region of the arm. A booster dose is not licensed for the vaccine. Zoster vaccination is not indicated to
treat acute zoster, to prevent persons with acute zoster from developing PHN, or to treat ongoing PHN. Before administration
of zoster vaccine, patients do not need to be asked about their history of varicella (chickenpox) or to have serologic
testing conducted to determine varicella immunity.
Introduction
Infection with varicella zoster virus (VZV) causes two distinct clinical conditions. Primary VZV infection
causes varicella (i.e., chickenpox), a contagious rash illness that typically occurs among children. A vaccine for preventing
initial
VZV infection has been available in the United States since 1995, and the Advisory Committee on
Immunization Practices (ACIP) recommends routine varicella
vaccination for all persons aged >12 months who lack evidence
of immunity (1--3). Varicella vaccination has dramatically reduced chickenpox cases among children
(3).
VZV can reactivate clinically decades after initial infection to cause herpes zoster (zoster) (i.e., shingles), a
localized and generally painful cutaneous eruption that occurs most frequently among older adults. Approximately 1 million
new cases of zoster occur in the United States annually. Approximately one in three persons in the general population
will develop zoster during their lifetime. A common complication of zoster is postherpetic neuralgia (PHN), a chronic
pain condition that can last months or even years. In May 2006, a live, attenuated vaccine for prevention of
zoster (ZOSTAVAX®, manufactured by Merck & Co., Inc.) was licensed in the United States for use in persons aged
>60 years. This report provides recommendations for use of zoster vaccine for prevention of zoster and its sequelae.
Methods
In Spring 2005, Merck & Co., Inc. (Whitehouse Station, New Jersey) submitted a Biologics License Application
to the Food and Drug Administration (FDA) for an investigational live, attenuated vaccine for prevention of zoster on
the basis of a phase 3 clinical trial. These results were published in June 2005
(4) and presented at the ACIP meeting later that month. In September 2005, ACIP's measles-mumps-rubella and varicella workgroup expanded its membership
to include experts in adult medicine and in zoster and began review of relevant data on zoster and the
investigational vaccine. Shortly thereafter, this workgroup reformed as the ACIP shingles workgroup and, during subsequent
months, held 19 conference calls to review and discuss scientific evidence related to herpes zoster and zoster vaccine,
including the epidemiology and natural history of zoster and its sequelae, and the safety, immunogenicity, efficacy,
financing, storage, and handling of the zoster vaccine. The workgroup also reviewed several economic analyses on zoster
prevention. Workgroup members participated in 10 additional conference calls to develop and discuss recommendation options
for preventing zoster. When scientific evidence was lacking, recommendations incorporated expert opinions of
the workgroup members.
Presentations of background materials on zoster and the vaccine were made during ACIP meetings in October
2005 and the three meetings in 2006. Following vaccine licensure on May 25, 2006, recommendation options were
presented to ACIP in June 2006, and final options were presented at the October 2006 meeting. During review by CDC
and external partners, modifications were made to the proposed recommendations to update and clarify wording in
the document. As new information on the epidemiology and prevention of zoster becomes available, it will be reviewed
by ACIP and recommendations will be updated as needed.
Background
Biology of VZV
VZV is an exclusively human pathogen that infects approximately 98% of the adult population in the United
States (5). The primary infection typically occurs during childhood and causes varicella. During its viremic phase,
cell-associated VZV gains access to epidermal cells, causing the typical varicella rash. The virus then enters sensory nerves
in mucocutaneous sites and travels through retrograde axonal transport to the sensory dorsal root ganglia adjacent to
the spinal cord where the virus establishes permanent latency in neuronal cell bodies
(6--7). Latent VZV is present in approximately 1%--7% of sensory ganglion neurons, with <10 genomic copies per infected cell
(8--10). Seeding of dorsal root ganglia also might occur during viremia. The magnitude of viremia, the number of skin lesions, and
the burden of VZV that establishes latency during primary varicella infection might be linked
(11). As with other members of the herpesvirus family, VZV is noninfectious in its latent form but can reactivate at a later time to form intact
virions in the involved sensory neurons. These virions then migrate to the skin through axons, spread from cell to cell,
and penetrate the epidermis (12). In its full clinical expression, zoster causes pain, which is followed by a vesicular
rash distributed across closely overlapping dermatomes
of the involved sensory nerve roots.
The triggers for reactivation of VZV have not been identified and probably involve multiple factors. However,
specific components of cell-mediated immunity (CMI) have an important role in controlling the development of zoster
by preventing reactivation within the neuron or the full clinical expression of reactivated VZV as zoster. The
effectiveness of these protective components of CMI is well maintained in immunocompetent persons during childhood and
early adulthood. These CMI components are believed to be partially or substantially maintained by
periodic immunologic boosting. "Endogenous boosting" might occur in response to subclinical reactivation of
latent VZV or to development of zoster itself, and "exogenous boosting" might occur in response to exposure to VZV circulating in the population
as chickenpox (13--19). Although virtually all adults are infected with VZV
(5), specific immunologic parameters have
not been identified to distinguish who will develop zoster. Anti-VZV antibody levels per se are not thought to have a role
in zoster prevention (20). Parameters that have been monitored and correlate with such protection include
anamnestic boost in anti-VZV antibodies in vivo in response to VZV-based vaccination, and the presence of and boost in
memory CD4 T cells as measured in vitro by proliferation of peripheral blood mononuclear cells (PBMC), by frequency
of proliferating PBMC, or by frequency of
interferon-g (IFN-g) releasing PBMC, all in response to VZV-antigens
(21,22). These latter two parameters are generally assessed using a responder cell frequency (RCF) assay and an
IFN-g enzyme-linked immunosorbent spot-forming cell (ELISPOT) assay, respectively
(22). VZV-specific class I-restricted and unrestricted cytotoxicities also have been monitored using target cell lysis
(23). Although CMI is necessary for the control of zoster, other nonimmunologic factors also might be involved
(24).
Clinical Features of Zoster and PHN
The clinical course of acute zoster is variable. It is usually less severe in children and younger adults. Typically,
zoster begins with a prodrome. Headache, photophobia, and malaise might occur, with fever being less
common. Abnormal skin sensations and pain of varying severity are the most common symptoms. These symptoms can
precede the zoster rash by days to weeks
(25) and rarely might be the only clinical manifestation of VZV reactivation
(termed zoster sine herpete) (7). Pain is described as aching, burning, stabbing, or shock-like. Altered sensitivity to touch,
pain provoked by trivial stimuli, and unbearable itching are all frequently reported.
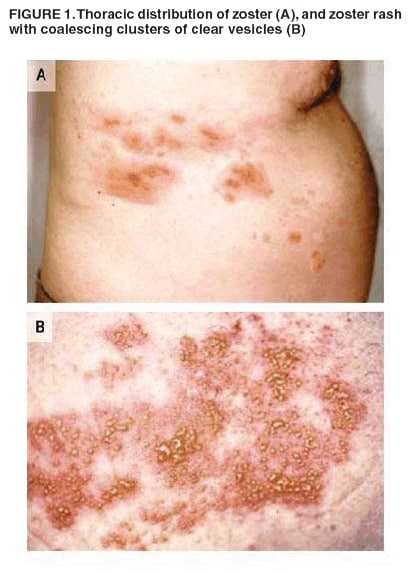
Zoster rash is typically unilateral and does not cross the mid-line, erupting in one or two adjacent dermatomes.
The frequency of zoster occurrence in different dermatomes has been evaluated in certain studies. In general,
thoracic, cervical, and ophthalmic involvement are most common
(Figure 1) (26--28). Small numbers of lesions can occur
outside the primary or adjacent dermatome. The rash is initially erythematous and maculopapular but progresses to
form coalescing clusters of clear vesicles containing high concentrations of VZV (Figure 1). The vesicles form over several
days and then evolve through pustular, ulcer, and crust stages. The rash usually lasts 7--10 days, with complete
healing within 2-4 weeks. However, pigmentation changes and scarring might be permanent. Streptococcal or
staphylococcal superinfections might complicate zoster rash
(29).
A common and potentially debilitating consequence of zoster is PHN, a persistent pain after resolution of the
rash. Pathologic observations thought to distinguish PHN from uncomplicated zoster include axonal and cell
body degeneration, atrophy of the spinal cord dorsal horn, scarring of the dorsal root ganglion, and loss of
epidermal innervation of the affected area. Certain experts believe this neuronal damage might be caused by ongoing
viral replication (30,31). In addition, consensus is lacking regarding criteria needed to distinguish the quality, duration,
or underlying pathophysiology of pain occurring with zoster versus PHN. Therefore, the duration of pain used to
define PHN has been inconsistent, ranging from any duration after resolution of the rash to periods from
>30 days to >6 months after rash onset.
Regardless of definition, the pain of PHN can last for weeks or months and occasionally persists for many years.
The nature of PHN pain varies from mild to excruciating in severity, constant, intermittent, or triggered by trivial
stimuli. Approximately half of patients with zoster or PHN describe their pain as "horrible" or "excruciating", ranging
in duration from a few minutes to constant on a daily or almost daily basis
(32). The pain can disrupt sleep, mood,
work, and activities of daily living, adversely impacting the quality of life and leading to social withdrawal and
depression (Table 1) (31--33). Anecdotes of suicide among
patients suffering from PHN have been reported
(34; Peter Richards, MD, personal communication, 2007). Among persons experiencing zoster, predictors of PHN include the
occurrence
and severity of pain both before and after onset of the rash, the extent of the rash, trigeminal or ophthalmic
distribution (35,36), and the occurrence of viremia
(37).
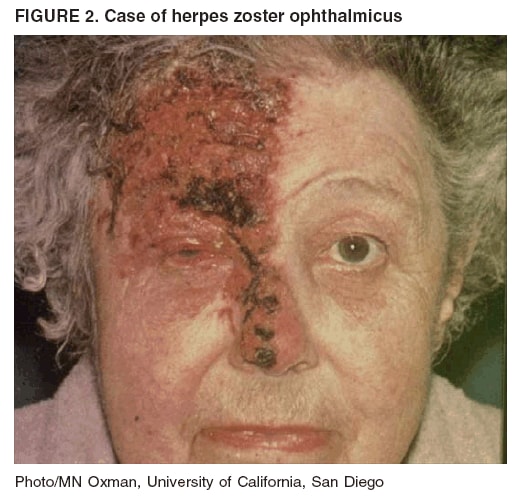
In addition to PHN, zoster is associated with a variety of other complication. Among persons with zoster,
10%--25% have eye involvement, called herpes zoster ophthalmicus (HZO)
(38,39) (Figure 2). HZO can occur when
reactivation involves the nasociliary branch of the trigeminal nerve, sometimes preceded by the presence of zoster vesicles on the
nose (Hutchinson sign). Keratitis occurs in approximately two thirds of patients with HZO
(40), often causing corneal ulceration. Other complications include conjunctivitis, uveitis, episcleritis and scleritis, retinitis, choroiditis,
optic neuritis, lid retraction, ptosis, and glaucoma. Extraocular muscle palsies also occur. Prolonged or permanent sequelae
of HZO include pain, facial scarring, and loss of vision
(41).
An uncommon complication of zoster is Ramsay Hunt syndrome, a peripheral facial nerve palsy accompanied
by zoster vesicles on the ear, hard palate, or tongue
(42). The pathophysiology of this complication involves reactivation
of VZV in the geniculate ganglion of the facial nerve.
Additional signs and symptoms of Ramsey Hunt syndrome
can include pain, vertigo, hearing loss, sensitivity to sound, tinnitus, and loss of taste. Many patients do not
recover completely (42). Idiopathic facial palsy (Bell's palsy) might be caused by inapparent VZV reactivation
(42,43).
Occasionally, zoster can cause motor weakness in noncranial nerve distributions, called zoster paresis
(44,45). The mechanism has not been determined. The weakness develops abruptly within 2--3 weeks after onset of the rash and
can involve upper or lower extremities. Diaphragmatic paralysis also has been described. The prognosis of zoster paresis
is good (46). Zoster also can result in autonomic dysfunction, causing urinary retention and colon pseudo-obstruction.
Rarely, patients will experience acute focal neurologic deficits weeks to months after resolution of the zoster
rash, involving the trigeminal distribution contralateral to the initial rash. This ischemic stroke syndrome,
termed granulomatous angiitis, is believed to be caused by direct extension of VZV from the trigeminal ganglion to
the internal carotid artery or its branches, resulting in inflammation
(30). Mortality from this syndrome is
substantial. Other rare neurologic complications of zoster include
myelitis, aseptic meningitis, and meningoencephalitis.
The prognosis for these conditions is good, although encephalomyelitis can be life threatening. Guillain-Barré syndrome
also has been reported in association with zoster
(47).
In immunocompromised persons, zoster initially might present typically. However, the rash tends to be
more severe and its duration prolonged
(48,49). One specific risk for persons with some immunosuppressive conditions
is dissemination of the zoster rash. True cutaneous dissemination generally occurs only among
immunocompromised patients, occurring in up to 37% of zoster cases in the
absence of antiviral treatment (49--54). Dissemination
usually begins with a dermatomal rash; however, the rash sometimes
begins with no primary dermatomal involvement
(54).
Cutaneous dissemination is not life-threatening; however, it is a marker for VZV viremia that can seed the lungs,
liver, gut, and brain and cause pneumonia, hepatitis,
encephalitis, and disseminated intravascular coagulopathy in
10%--50% of episodes. Visceral dissemination with no skin involvement can occur in profoundly immunocompromised
persons. Even with antiviral treatment, the case fatality rate from visceral dissemination is 5%--15%, with most
deaths attributable to pneumonia (49,54,55).
The risk for neurologic zoster complications is generally increased in immunocompromised persons.
These complications, which can be aggressive and even fatal, include myelitis, chronic encephalitis,
ventriculitis, meningoencephalitis, and cranial palsies
(30). However, the risk for PHN is not appreciably increased
among immunocompromised persons who develop zoster
(30).
Compared with other immunocompromised persons, the clinical features of zoster are less severe and
visceral dissemination less common among persons infected with
human immunodeficiency virus (HIV) (56,57). Some
zoster presentations that are unique to persons infected with HIV include atypical skin eruptions
(58,59) and an aggressive variant of acute retinal necrosis that generally results in blindness
(60). Alveolar bone necrosis and tooth exfoliation also have been reported
(61).
Diagnosis
Zoster diagnosis might not be possible in the absence of rash (e.g., before rash or in cases of zoster sine
herpete). Patients with localized pain or altered skin sensations might undergo evaluation for kidney stones, gallstones, or
coronary artery disease until the zoster rash appears and the
correct diagnosis is made (62). In its classical manifestation, the
signs
and symptoms of zoster are usually distinctive enough to make an accurate clinical diagnosis once the rash has
appeared (63). Occasionally, zoster might be confused with impetigo, contact dermatitis, folliculitis, scabies,
insect bites, papular urticaria, candidal infection, dermatitis herpetiformis, or drug eruptions. More frequently, zoster is confused with
the rash of herpes simplex virus (HSV), including eczema herpeticum
(4,31,64--66). The accuracy of diagnosis is lower
for children and younger adults in whom zoster incidence is lower and its symptoms less
often classic.
In some cases, particularly in immunosuppressed persons, the location of rash appearance might be atypical, or
a neurologic complication might occur well after resolution of the rash. In these instances, laboratory testing might
clarify the diagnosis (67--71). Tzanck smears are inexpensive and can be used at the bedside to detect multinucleated
giant cells in lesion specimens, but they do not distinguish between infections with VZV and HSV. VZV obtained
from lesions can be identified using tissue culture, but this can take several days and false negative
results occur because viable virus is difficult to recover from cutaneous lesions. Direct fluorescent antibody (DFA) staining of VZV-infected cells in
a scraping of cells from the base of the lesion is rapid and sensitive. DFA and other antigen-detection methods also can
be used on biopsy material, and eosinophilic nuclear inclusions (Cowdry type A) are observed on
histopathology. Polymerase chain reaction (PCR) techniques performed in an experienced laboratory also can be used to detect
VZV DNA rapidly and sensitively in properly-collected lesion material, although VZV PCR testing is not available in
all settings. A modification of PCR diagnostic techniques has been used at a few laboratories to distinguish wild-type
VZV from the Oka/Merck strain used in the licensed varicella and zoster
vaccines.
In immunocompromised persons, even when VZV is detected by laboratory methods in lesion
specimens, distinguishing chickenpox from disseminated zoster might not be possible by physical examination
(72) or serologically (73--75). In these instances, a history of VZV exposure, a history that the rash began with a dermatomal pattern,
and results of VZV antibody testing at or before the time of rash onset might help guide the diagnosis.
Zoster Transmission
Zoster lesions contain high concentrations of VZV that can be spread, presumably by the airborne route
(76,77), and cause primary varicella in exposed susceptible persons
(77,78--83). Localized zoster is only contagious after the
rash erupts and until the lesions crust. Zoster is less contagious than varicella
(78). In one study of VZV transmission from zoster, varicella occurred among 15.5% of susceptible household contacts
(78). In contrast, following household exposure to varicella, a more recent study demonstrated VZV transmission among 71.5% of susceptible contacts
(84). In hospital settings, transmission has been documented between patients or from patients to health-care personnel,
but transmission from health-care personnel to patients has not been documented. Persons with localized zoster are
less likely to transmit VZV to susceptible persons in household or occupational settings if their lesions are covered
(85).
Epidemiology of Zoster and Complications
Risk Factors
Infection with VZV
Wild-type VZV. Because zoster reflects reactivation of
latent VZV, the primary risk factor and a necessary
precondition for zoster is previous VZV infection. Approximately 99.5% of the U.S. population aged
>40 years has serologic evidence of previous infection, including all evaluated subgroups; therefore, all older adults are at risk for zoster
(5), although many cannot recall a history of varicella
(86--90). Varicella vaccine is effective at preventing initial wild-type
VZV infection in persons not previously infected. Any wild-type VZV infections prevented cannot reactivate as
zoster.
The age at the time of initial VZV infection influences the age at which zoster occurs. Persons acquiring
an intrauterine or early childhood infection with VZV are at
increased risk for pediatric zoster (91--93). When
VZV infections occur before age 2 months, the risk for zoster occurring by the age of 12 years is increased >35-fold
compared with the risk for VZV infections occurring after
infancy (92). Other case series suggest that the risk for
pediatric zoster also might be increased in children who experienced varicella at older ages
(94). Conversely, the risk for zoster might
be diminished in persons born in countries
(95) or living in communities (96) where varicella
infection tends to occur at
later ages. These observations suggest that changes in the epidemiology of varicella caused by varicella vaccination or
by other factors can alter the epidemiology of zoster, particularly pediatric zoster.
Oka/Merck Strain VZV. Among vaccine recipients, the attenuated Oka/Merck strain of VZV included in
varicella vaccine also can establish a latent infection and clinically reactivate as zoster
(97). Zoster caused by Oka/Merck strain VZV cannot be distinguished on clinical grounds from zoster caused by wild-type VZV. The risk for zoster
caused specifically by Oka/Merck strain VZV is unknown because recipients of varicella vaccine might have already
been infected with wild-type VZV or might have become
infected with wild-type VZV following vaccination (i.e., due
to vaccine failure) that could also reactivate. Therefore, the rate of all episodes of zoster among varicella vaccine
recipients define the upper bound for the risk of the subset of episodes caused by Oka/Merck strain VZV. The risk for zoster
in immunocompromised children was approximately 65% less for those who had received the
varicella vaccine compared with those with previous wild-type varicella infection
(98,99). In immunocompetent children, the risk also appears
to be reduced among 1-dose vaccine recipients compared with children with a history of wild-type varicella,
although longer follow up is needed
(99--101). The risk for zoster in immunocompetent children following 2 doses of
varicella vaccine has not been studied. Collectively these studies suggest that the risk for Oka/Merck strain zoster
following varicella vaccination is no higher, and likely considerably lower, than that following wild-type varicella infection,
even though the acquisition of the Oka/Merck VZV through vaccination generally occurs at a young age (i.e.,
varicella vaccination is recommended for children aged
>12 months [1--3]), which might be a risk factor for pediatric zoster.
As varicella vaccine recipients age, the risk for and manifestation of Oka/Merck strain zoster in older persons at greater
risk for zoster complications can be evaluated.
Age
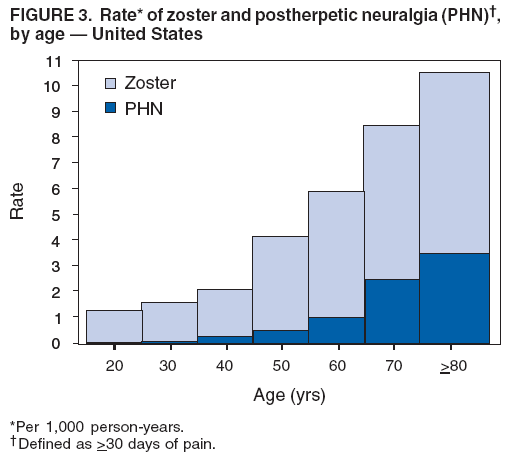
Influence on zoster. Age is the most important risk factor for development of zoster
(Figure 3). Virtually all studies conducted in numerous settings and with various study designs have indicated an association between age
and increasing zoster incidence, extending to the oldest cohorts
(4,62,95,102--104). One study indicated that
zoster incidence increased with age by a factor of >10, from 0.74 per 1000 person years in children aged <10 years to 10.1
per 1000 person years in persons aged 80--89 years, with much of the increase beginning at age 50--60 years
(13). Approximately 50% of persons who live to age 85 years will have experienced zoster
(105,106).
The important role of age as a risk factor for zoster is presumably related to a loss of components of
VZV-specific CMI response because of aging (i.e., immune
senescence) possibly combined with waning immunity that might occur
over time following initial varicella infection. Loss of specific immunity allows VZV to complete the process of
reactivation and spread to the epidermis to produce the fully expressed clinical illness
(12). Although precise correlates of
protection against zoster have not been identified, certain CMI responses to VZV antigen decline with age
(21,22,107,108).
Influence on PHN. Among persons experiencing zoster, the primary risk factor for the development of PHN is
age. Several studies have indicated that the risk for PHN among persons with zoster increases with age, particularly
for persons aged >50 years
(13,35,62,109,110) (Figure 3). In one study, the risk for experiencing at least 2 months of
pain from PHN increased 27.4-fold among patients aged
>50 years compared with those aged <50 years
(109). Approximately 80%-85% of PHN occurs in zoster patients aged
>50 years (62).
Sex
Results from a large, randomized, controlled vaccine trial in the United States
(4) indicated that the incidence of confirmed zoster cases in a cohort of immunocompetent persons aged
>60 years was 11% higher among the women (11.8 versus 10.7 cases per 1000 person years in women and men, respectively). A prospective cohort study in
the Netherlands documented 38% more cases among women than men (odds ratio = 1.38 [95% confidence interval [CI]
= 1.22--1.56) after controlling for age and other zoster risk factors
(111). Other studies
(13,102--104,112) using a variety of methods also demonstrated an age-standardized excess of zoster among women. However, some researchers
did not find a difference by sex
(36,38,105,113--115). Women with zoster might also be at increased age-specific risk
for developing PHN compared with men (35,62).
Race
Certain studies have suggested racial differences in the risk for zoster. In North Carolina, reported lifetime
zoster occurrences and reported incidence were lower in blacks by 65% and 75%, respectively, compared with
whites after controlling for relevant confounders
(115,116). A study in the United Kingdom indicated that zoster risk
in patients was 54% lower among blacks after adjusting for age, sex, country of birth, or household childhood
contacts (95). The reasons for these racial differences are unknown.
Geographic or Seasonal Variation
Most studies have not documented a seasonal pattern to zoster incidence
(13,38,92,95,105,117). Certain studies have reported summer seasonality, particularly for exposed skin sites. This pattern might be related to ultraviolet
irradiation that peaks during summer months and might serve as a trigger for zoster
(28,118,119). No studies exist regarding variation in zoster incidence by latitude. Urban/rural status does not appear to be a risk factor for zoster
(95).
Altered Immunocompetence
Unlike other vaccine-preventable diseases, zoster epidemiology is not directly related to exposure but to the
biology underlying the virus-host relation that allows reactivation of latent VZV. Because CMI plays a key role in
controlling both development of zoster and the features of its clinical expression, deficiencies in CMI, regardless of their etiology,
are risk factors for both zoster and its severe manifestations. Although the magnitude of zoster risk can be extremely
high among immunocompromised persons, the overall population attributable risk is modest because
immunosuppression is uncommon (62,103,114).
The incidence of zoster is increased substantially in persons with hematologic malignancies and solid tumors
(120). Rates are highest among children with these conditions. The magnitude of risk depends on both the nature of
the underlying cancer and the type of treatment
(121). Although the incidence of zoster in patients with solid
tumors is <5%, this rate is many-fold higher than that in unaffected age-matched persons
(120). Patients with Hodgkin's disease are at particularly high risk for zoster, with cumulative risks during the illness and its treatment as high as
27.3% (51,53,120,122--127).
Zoster is common following hematopoietic stem cell transplantation (HSCT); rates are 13%--55% during the
first year (54,128,129). Rates are increased following solid organ transplants (renal, cardiac, liver, and lung)
(5%--17%). Incidence is highest during the months immediately following the procedure, and the majority of zoster cases
occur within a year of transplantation
(130--132).
The risk for zoster and its recurrence is elevated in persons infected with HIV. Zoster rates of 29.4--51.5 per
1000 person years have been reported among HIV-infected adults, reflecting 12- to 17-fold increase compared with
HIV-negative persons (56,133--136). For HIV-infected children, the risk is even higher (467 per 1000 person
years), especially among children who acquire VZV infection when they are profoundly immunosuppressed
(137). Most studies have documented increasing zoster risk as CD4+
T-lymphocyte counts decline, but the risk is increased
nine-fold even among HIV-infected women with CD4+
T-lymphocyte counts >750/µL compared with
HIV-negative controls (135). However, the risk might decline at CD4+ T-cell counts <50
cells/µL (136). Persons infected with HIV also are
at increased risk for recurrences of zoster.
Other Co-morbidities
The risk for zoster appears to be elevated in persons with inflammatory diseases; however, for most of these
conditions, data are insufficient to determine how much of the risk is attributable to the underlying disease versus its
treatment. Zoster has been associated with systemic lupus erythematosus (SLE), with rates of 15--91 per 1000 person years
(138--143). The risk for zoster also is increased among persons with rheumatoid arthritis (adjusted hazard ratio = 1.9 [95%
CI = 1.8--2.0]), with an incidence of approximately 10 cases of per 1000 person years reported
(144,145). Patients with Wegener's granulomatosis have a reported incidence of 45 zoster cases per 1000 person years
(146), and recurrences in these patients are common. In one study, Crohn's disease and ulcerative colitis were both associated with a
significantly increased risk for zoster (incident rate ratios = 1.6 and 1.2, respectively). The
increase was, in part, caused by use of immunosuppressive medications
(147). For all these conditions, zoster is generally not life-threatening,
although cutaneous dissemination is more common, and deaths have been reported in such patients
(138,141,142).
Certain studies have evaluated the risk for zoster in persons with other noninflammatory co-morbid
conditions, although findings have not been consistent. Two studies have documented an association between zoster and
diabetes mellitus (148,149). However, this association was not indicated in two other studies
(150,151). Another study documented an increased risk for zoster in persons who subsequently had multiple sclerosis diagnosed
(152).
Exposure to VZV/External Boosting
VZV can be transmitted from zoster lesions to cause primary varicella in susceptible persons. Although
some experts have suggested that zoster can be caused directly by exposure to VZV from varicella or from other cases of
zoster (72,153,154), in general, zoster is not associated with epidemics of varicella. In addition, zoster does not have a
seasonal pattern to suggest it is spread directly from varicella
(13,28,38,92,105,117). Theoretically, reactivation of latent
VZV might be triggered by exposure to exogenous VZV
(123,153); however, no evidence suggests that such episodes
occur more frequently than would be expected to occur by chance.
Conversely, exposure to varicella might reduce the risk for zoster
(13). Protection might be partially maintained
by exposure to varicella circulating in the population and the resulting exogenous boosting of VZV-specific
immunity (15,117,155). An analysis of surveillance data from the United Kingdom indicated an inverse relation between
annual varicella incidence in children aged <5 years and zoster incidence in adults aged 15--44 years
(117). A case-control study in the United Kingdom
(15) documented a graded reduction in zoster risk as a function of number of
varicella contacts over a 10-year period. Multivariate analysis suggested a 74% reduction in risk for zoster among persons
with three to four varicella exposures compared with those with no exposures, with a significant trend suggesting
some reduction with fewer than three exposures. Social contacts with children (as a proxy for
varicella exposure) and occupational contact with sick children were protective
(15). A cohort analysis based on data from a sentinel
physician network in the United Kingdom
(155) suggested that adults living with children had both increased varicella
exposure and a 25% decrease in zoster incidence. The analysis estimated that this boosting effect lasted an average of 20
years (95% CI = 7--41 years). However, persons living or interacting with children might have different underlying
health compared with persons without exposure to children, which might be a confounder in these studies. Other
evidence that varicella exposure might protect against zoster includes possible effects household
exposure to varicella had against subsequent development of zoster among children with leukemia
(156). Finally, the efficacy of the zoster vaccine
(4) supports the concept that exposure to exogenous VZV can reduce risk for zoster, presumably by boosting
specific immunity against VZV.
Contrary evidence also exists that varicella exposure does not reduce the risk for zoster. Women are at greater risk
for zoster (13,102,103,110,111) despite the fact that women probably have more exposure to young children
who experience varicella. A Japanese study indicated that the risk for zoster in children was not diminished by
repeated varicella exposures (92).
Although a sufficient number of varicella exposures could reduce the risk for zoster in select populations, it is
unclear whether such levels of exposure play an epidemiologically important role in reducing the risk for zoster among
the general population of older adults who are at the highest risk for the disease, and, if so, how long such effects would
last in the elderly.
Other Risk Factors
As with orofacial and genital flairs of HSV, zoster has been anecdotally linked to stress. However, only two
rigorous evaluations of the role of psychological stress on zoster have been conducted. A case-control study documented
a significant association with number of stressful life events within 6 months of reported zoster (p = 0.012)
(157). A prospective cohort study indicated a nonsignificant association (p = 0.078) between zoster risk and negative life events.
Trauma or surgery could lead to reactivation of VZV in the affected dorsal root ganglion and increase the risk for
zoster rash in that dermatome. Such a development would seem to be specific and easily ascertained, and certain
reports and case series describe such events
(158--161). One case-control study collected information about recent trauma
and/or surgery in patients who developed zoster and in matched controls. The frequency of trauma in nonzoster sites
was similar between the two groups, but zoster patients
were significantly more likely than controls to report
trauma at the site of their zoster during the month before zoster onset (adjusted OR = 12.1 [95% CI = 1.5--97.6]; p = 0.002)
(24).
The basis by which these stimuli provoke zoster is unclear, but they suggest that nonimmunologic factors can
play important roles in the pathophysiology of zoster.
Finally, one study indicated that dietary micronutrient intake was protective against zoster. Body mass index did
not appear to be associated with zoster risk
(162). Genetic predisposition for zoster also has been reported
(163).
Population Rates of Zoster and PHN
Zoster
Zoster is not a reportable condition in the United States; therefore, incidence has been inferred from a variety
of studies. Observed rates have varied substantially on the basis of methods for case ascertainment, access to health
care, and case definitions. The age distribution in the population being studied also is an important consideration
when comparing these studies because zoster can vary dramatically across study sites. Conclusions cannot be drawn from
cross-study comparisons without adjusting for age or comparing age-specific rates directly. Differences in the prevalence
of immunosuppression or in racial makeup also can influence population-wide zoster incidence. In addition, the
incidence of zoster appears to have been increasing over recent
decades, even after adjusting for other factors, although this
increase has not been observed consistently.
Despite these limitations, certain analyses of zoster incidence in the United States have been conducted. The
incidence in all studies ranged from 3.2--4.2 per 1000 population per year (age-adjusted to the 2000 U.S.
population) (62,103,104,114,164,165), translating into an
estimated 1 million cases annually. In all studies, a
substantial increase in zoster incidence occurred with age and extended to the oldest strata; for all persons aged
>60 years, the annual incidence was approximately 10 per 1000 persons
(62,103,104,114,164,165), similar to the annual
incidence of 11.1 per 1000 observed during the zoster vaccine trial
(4). On the basis of these data, an estimated 32% of persons
in the United States will experience zoster during their lifetime (CDC unpublished data, 2007).
Certain studies provide evidence of increasing
age-specific zoster incidence in the United States
(38,62,165,166), although other studies have shown no such trend
(104). The observed increases cannot be solely attributed to changes
in the epidemiology of varicella, because documentation of increases predated licensure of varicella vaccine in the
United States in 1995 (38) and because age-specific increases over time also are being
reported in certain international settings, including in the absence of varicella vaccination programs
(105,167,168). Because the basis for this increase
remains unclear, predicting whether the age-specific risk for zoster will continue to increase in the future is difficult.
Recurrent Zoster
Effectively evaluating the risks for recurrent zoster
(i.e., second or subsequent episodes) in
immunocompetent persons requires large populations, long-term follow up,
adequate duration, and laboratory confirmation. Although data
are limited, certain studies suggest a recurrence rate that is comparable to the rate of initial episodes
(13,38,114). A community-based study of clinician-diagnosed zoster was conducted in Olmsted County, Minnesota. The
observational period lasted 6 years. Of 1,669 persons that experienced an episode of zoster during that period, 24 experienced
a second episode, suggesting a high incidence of zoster
recurrence and providing no evidence that an episode of
zoster protects against recurrence (62). Similar observations were noted in an older survey-based study
(169). In the Shingles Prevention Study, two of approximately 20,000 vaccine placebo recipients had two episodes of zoster within 3 years
of the initial episode. These cases provide the first laboratory-confirmed evidence that zoster can recur
in immunocompetent persons, even soon after the initial
episode (4).
Zoster Hospitalizations and Deaths
Hospitalizations. Conclusions about hospitalization for zoster should be interpreted carefully if they are derived
from administrative data. Hospital administrative data
often do not distinguish zoster episodes that were reasons
for hospitalizations from those episodes that were incidental to the hospitalization or that occurred during
prolonged hospital stay. PHN at the time of an unrelated hospitalization also might be coded as zoster. In addition,
underlying immunosuppressive conditions might not be available or might not be collected from administrative data. These
factors preclude determination of the portion of hospitalizations that could be prevented by a live-attenuated vaccine that
is contraindicated for immunosuppressed persons.
Given these limitations, crude annual rates of zoster hospitalization have ranged from 2.1 per 100,000 population in
a Northern California managed care population
(170) to 4.4 per 100,000 population in England
(171). A crude rate of 16.1 per 100,000 population was identified in an analysis of Connecticut-wide hospitalization data that
included all zoster episodes, not just primary discharge
diagnosis (172).
In a community-based study in Olmsted County, Minnesota, approximately 3% of patients with zoster
were hospitalized for the illness (62). Although values differ substantially, all studies indicate that zoster hospitalization
rates increase with age (170,172--174). In the Connecticut study, zoster hospitalization rates were approximately
75-fold greater among persons aged >85 years than in persons aged <30 years
(172). Although precise denominators are
not available, risks for hospitalization also increased among persons with altered immunocompetence; approximately 30%
of all persons hospitalized with zoster episodes had one or more immunocompromising conditions, primarily
malignancies (82%) and HIV infection (8%)
(62,172). Central nervous system and ophthalmologic complications accounted for
most of the reported complications among hospitalized zoster cases
(172--174), although bacterial superinfection
was common in one series (175). Another study indicated that 0.5% of patients with confirmed zoster were
hospitalized before their zoster rash developed for prodromal pain syndromes including suspected myocardial infarction, severe
new-onset headache, back pain, and abdominal pain resulting in appendectomy
(62).
Deaths. On the basis of clinical experience and in the absence of zoster-related deaths in cohort studies, certain
experts believe that zoster mortality appears to be uncommon, particularly among healthy persons
(176). Vital records might not distinguish deaths attributed to zoster from
incidental deaths occurring merely in the presence of zoster, and
they might not capture information on the immunologic status among those deaths. An Australian study
using administrative data indicated that 1% of patients hospitalized with a primary zoster diagnosis died; the number
of deaths directly attributable to zoster was not validated
(174). Certain analyses have indicated that almost all
zoster deaths occur in the elderly, with a rate
>10-fold higher among persons aged >65 years
(171,173,174). Immunosuppression also appears to be a risk factor for zoster mortality. In one study, 52% of patients hospitalized
with zoster who died had one or more immunocompromising condition (e.g., malignancies, leukemia, and HIV). In
that study, the risk for death in persons with immunocompromising
conditions was 8.7%; the risk in persons without
these conditions was 3.7% (172).
PHN
Drawing conclusions from studies on the risk for PHN is difficult because definitions for PHN vary and results
are influenced by many factors, including the source and age of the study population. Among zoster patients treated with
a placebo in clinical trials of antiviral drugs, approximately one third still had pain after 3 months and approximately
one fourth had pain at 6 months (177,178). However, these trials might include a population of patients with more
severe zoster pain, thereby introducing a detection bias that could inflate estimated risks for PHN. In a phase 3 clinical trial
of zoster vaccine (4), zoster occurred among 642
placebo recipients; the risk for pain persisting at least 30, 60, 90, 120
or 180 days among these person was 30.3%, 17.6%, 12.5%, 8.4%, and 5.1%, respectively. Results from the trial
might not reflect risks for progression to PHN in community settings because ascertainment, diagnosis, and antiviral
treatment of zoster were standardized and thorough. However, in a community-based study in Olmsted County, Minnesota,
in which almost all medical events were captured, the risk for PHN in patients with zoster was 18%, 13%, and 10%
when defining PHN as at least 30, 60, and 90 days of pain, respectively
(62).
Treatment and Nonspecific Management of Zoster and PHN
The treatment of acute zoster, the prevention of PHN development among patients with acute zoster, and
the treatment of patients with current PHN are complex clinical problems with ongoing uncertainties and active
research (31). Acyclovir, famciclovir, and valacyclovir are approved by the FDA for treatment of zoster in
immunocompetent patients. All three are nucleoside analogs that inhibit replication of human herpes viruses, including VZV. Clinical
trials have indicated that these agents, taken orally, reduce the duration of viral shedding and lesion formation,
reduce the time to rash healing, and decrease the severity and duration of acute pain from zoster and the risk for progression
to PHN. Because all three antiviral agents are safe and well tolerated, many experts recommend that treatment should
be considered for all eligible patients with zoster, and specifically recommend treatment for persons aged
>50 years who
have moderate or severe pain, moderate or severe rash, or involvement of nontruncal dermatomes
(31). In clinical trials, treatment has been initiated within 72 hours of rash onset, a biologically arbitrary time point that often is not
feasible in clinical practice. The benefits of later treatment have not been studied
(31). If treatment cannot be initiated
within 72 hours of rash onset, experts recommend that it should be initiated as soon as possible, particularly in the presence
of new vesicle formation or of complications.
Two clinical trials have assessed the role of corticosteroids in combination with acyclovir for treatment of zoster
and prevention of subsequent PHN (179,180). Patients at risk for steroid-related toxicities (e.g., those with diabetes
mellitus or gastritis) were excluded from the trials. A
3-week tapering course of corticosteroids diminished acute zoster pain
and decreased the time to cutaneous healing, cessation
of analgesic therapy, and return of uninterrupted sleep and
normal daily activities. However, no evidence indicated
that use of corticosteroids prevented development of PHN.
Theoretically, corticosteroids should be equally effective in combination with valacyclovir or famciclovir; however, combinations
of these agents have not been studied in clinical trials. No evidence indicates that topical
antiviral therapy or corticosteroids without systemic
antiviral therapy have a role in treatment of zoster.
A variety of approaches have been used with varying
degrees of success for control of acute zoster pain,
including acetaminophen, nonsteroidal anti-inflammatory agents, tricyclic antidepressants, opiates, anticonvulsants, capsaisin,
and topical anesthetics (31). In more severe instances of pain, referral to a pain specialist, or even hospitalization
and administration of epidural analgesics, is often considered. Many of these same modalities are used with varying
degrees of success for control of chronic PHN pain
(26,181,182). Elderly persons, who already have reduced physiologic
reserve and typically take multiple medications for pre-existing chronic conditions, might be unable to tolerate
psychotropic and other medications for management of their acute zoster or chronic PHN pain
(31,33).
Patients with uncomplicated zoster should be advised to keep the rash clean and dry, to avoid topical antibiotics,
and, if possible, to keep the rash covered. They should alert their physician if the rash worsens or they have fever, which
could indicate bacterial superinfection (31).
Prevention of Transmission from Zoster
Some health-care institutions might exclude personnel with zoster from work until their lesions dry and crust
(85). Persons with localized zoster should avoid contact with susceptible persons at high risk for severe varicella
in household and occupational settings until lesions are crusted. Such persons include pregnant women, all
premature infants born to susceptible mothers, infants born at
<28 weeks' gestation or who weigh <1000 g regardless of
maternal immune status, and immunocompromised persons of all ages
(85). Persons with opportunities for contact with
such high risk-persons in household or occupational settings should be informed about how to recognize the signs
and symptoms of zoster. If a person susceptible to varicella infection has close exposure to a persons with zoster,
postexposure prophylaxis with varicella vaccine or
VARIZIG™ should be considered
(3,85,183).
Zoster Vaccine
Vaccine Composition, Dosage, and Administration
The zoster vaccine licensed in the United States
(ZOSTAVAX®, Merck & Co., Inc.) is a lyophilized preparation of
the Oka/Merck strain of live, attenuated VZV, the same strain used in the varicella vaccines
(VARIVAX®,
PROQUAD®). The Oka strain was isolated in Japan
(184) in the early 1970s from vesicular fluid from a healthy child who
had varicella; the strain was attenuated through sequential
propagation in cultures of human embryonic lung
cells, embryonic guinea-pig cells, and human diploid cells (WI-38). Further passage of the virus was performed at
Merck Research Laboratories in human diploid cell cultures
(MRC-5). The cells, virus seeds, virus bulks, and bovine
serum used in the manufacturing are all tested to provide assurance that the final product is free of adventitious agents.
Zoster vaccine, when reconstituted as directed in the package label using the supplied diluent, is a sterile
preparation for subcutaneous administration. Each 0.65-mL dose contains a minimum of 19,400 PFU (4.29
log10) of Oka/Merck strain of VZV when reconstituted and stored at room temperature for up to 30 minutes. Zoster vaccine is similar
to VARIVAX®. However, its minimum potency is at least 14-times the potency of
VARIVAX®, which contains a minimum
of 1,350 (approximately 3.13 log10) PFU.
PROQUAD® contains 3.993 log10
PFU, similar in potency to
ZOSTAVAX®. Each dose of zoster vaccine also contains additional VZV antigenic component from nonviable Oka/Merck
VZV. Additional vaccine components in each dose include 31.16 mg of sucrose, 15.58 mg of
hydrolyzed porcine gelatin, 3.99 mg of sodium chloride, 0.62 mg of monosodium L-glutamate, 0.57 mg of sodium
phosphate dibasic, 0.10 mg of potassium phosphate monobasic, 0.10 mg of potassium chloride; residual components of MRC-5 cells including
DNA and protein; and trace quantities of neomycin and bovine calf serum. The product contains no thimerosal or
other preservatives.
Zoster vaccine should be administered as a single
0.65-mL dose subcutaneously in the deltoid region of the
upper arm; a booster dose is not licensed for the vaccine. The vaccine should not be injected intravascularly
or intramuscularly and should only be reconstituted and
injected using a sterile syringe free of preservatives,
antiseptics, and detergents, which can inactivate the vaccine virus.
Storage and Handling
To maintain potency, lyophilized zoster vaccine must be stored frozen at an average temperature of
<5°F (<-15°C) until it is reconstituted for injection. Any freezer that has a separate sealed freezer door and reliably maintains
an average temperature of <5°F
(<-15°C) is acceptable for storing zoster vaccine. Providers should check the adequacy
of their freezer by verifying its temperature before obtaining vaccine. In general, the freezer compartments of
dormitory style units are incapable of reliably maintaining temperatures cold enough to store zoster vaccine and are
unacceptable for storage. For certain refrigerator/freezer models, it is necessary to reduce the temperature to the coldest setting
to maintain zoster vaccine at the correct temperature. However, this might reduce the temperature in the
refrigerator compartment and result in freezing of any vaccines or other pharmaceutical products being refrigerated. As a result,
both the refrigerator and freezer temperatures should be monitored and the temperature recorded at least twice a day.
Any out-of-range temperature readings require immediate and documented corrective action. When a freezer is
temporarily unavailable (e.g., during transport or equipment failure), zoster vaccine should be stored in a suitable container (i.e.,
the original shipping container or a comparable container with a properly fitting lid) with an adequate quantity of dry
ice (i.e., a minimum of six pound per box) so that dry ice would persist in the container if unreconstituted vaccine must
be transported back to the freezer. Dry ice placed in a suitable container will maintain a temperature of
<5°F (<-15°C). The diluent, which does not contain preservative or other antiviral substances that could inactivate the vaccine virus,
should be stored separately, either at room temperature or in the refrigerator. The vaccine should be reconstituted according
to the directions in the package label and only with the diluent supplied. Before reconstitution, zoster vaccine should
be protected from light. Once reconstituted, the vaccine should be used immediately to minimize loss of potency.
The vaccine must be discarded if not used within 30 minutes after reconstitution. Information regarding stability
under conditions other than those recommended is available from the manufacturer at 800-637-2590.
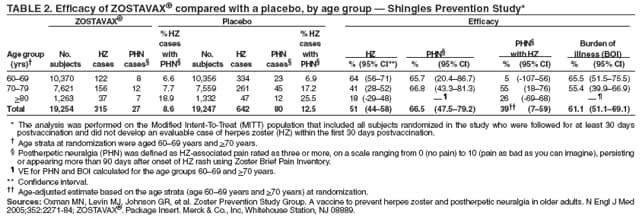
Efficacy
The efficacy of zoster vaccine was evaluated in a phase 3 vaccine trial termed the Shingles Prevention Study, a
double-blind randomized, placebo-controlled trial involving 38,546 healthy adults aged
>60 years who had a history of varicella or at least 30 years of residence in the continental United States (as a marker of previous infection). Persons
excluded from the trial included those with a history of zoster, with allergies to components of the vaccine,
with immunocompromising conditions, or with conditions that might have interfered with study evaluations (e.g.,
cognitive impairment, <5 year life expectancy, dermatologic disorders, chronic pain, hearing loss, or lack of mobility). The
study population ranged in age from 59--99 years
(median: 69.4 years), and comprised 41.0% females, 95.4% white,
2.1% blacks, 1.3% Hispanics, and 1.2% other or unknown race/ethnicity. On enrollment, approximately 90% of
the participants had at least one underlying chronic medical condition.
Persons were randomized to receive a single subcutaneous dose of zoster vaccine or placebo; the mean duration
of follow up was 3.1 years. Active case ascertainment was conducted through monthly telephone contact supplemented
by a close-out interview. Zoster cases were confirmed by PCR testing (93%), viral culture (1%), or evaluation by a panel
of five physicians with expertise in zoster diagnosis (6%). Patients with confirmed zoster were followed for at least 182
days
to assess the outcome of the condition, including presence and severity of pain. Approximately 95% of persons
were followed to completion of the study. Outcomes evaluated included incidence of zoster, incidence of PHN (defined
as pain level of three or more [on a numerical rating scale of 0-10] persisting at least 90 days after rash onset), and
burden of illness (BOI), measured using a mean value of severity-by-duration index for each treatment group, thus
incorporating the incidence, severity, and duration
of pain and discomfort from zoster). A total of 957 confirmed cases of
zoster occurred among study participants: 315 among vaccine recipients and 642 among placebo recipients. The proportion
of vaccine and placebo recipients that received antiviral treatment within 72 hours of rash onset, as clinically indicated,
was 64.1% and 65.9%, respectively.
The vaccine reduced the risk for developing zoster by 51.3% (95% CI = 44.2--57.6; p<0.001
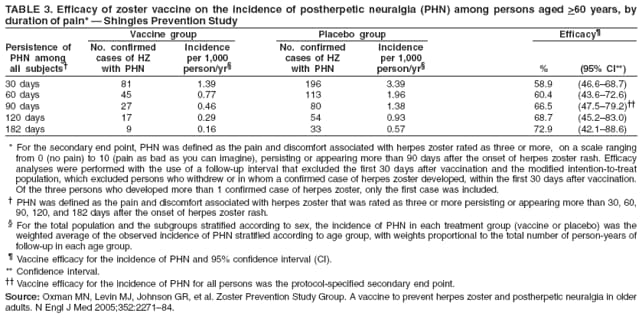
(Table 2) (4). The vaccine was 66.5% (95% CI = 47.5--79.2; p<0.001) efficacious for preventing PHN. When the definition of PHN
was changed from 30 days of pain to 182 days of pain following rash onset, vaccine efficacy increased from 58.9% to
72.9% (Table 3). Zoster vaccine had an independent effect of reducing PHN among patients who developed zoster (39%
[95% CI = 7%--59%]) (Table 2). The mean severity-by-duration of zoster was reduced by 57%
(p = 0.016) in vaccine recipients who developed PHN. Zoster vaccine reduced BOI by 61.1% (95% CI = 51.1--69.1; p<0.001) (Table 2).
The vaccine reduced the degree of interference in activities of daily living (ADLI) caused by zoster, in part because of
the reduction in zoster itself, but also because of a decrease in ADLI among those vaccine recipients who did develop
zoster (185). No evidence indicated that vaccine recipients experiencing zoster were protected from other sequelae such
as scarring, bacterial superinfection, palsies, or ocular or visceral complications
(186).
In general, with increasing age at vaccination, the vaccine retained efficacy against severity of zoster better than
against zoster itself. Thus, efficacy for the prevention of zoster was highest among persons aged 60--69 years and declined
with increasing age (Table 2). Declines in efficacy of preventing zoster were observed with each 5-year increase in
age throughout the age range of participants
(187). However, no significant differences were observed among persons
aged 60--69 years versus those aged >70 years in vaccine efficacy at reducing BOI or PHN, probably
because the independent effect of reducing PHN among patients who developed zoster was greatest among persons aged 70--79 years (Table 2). For persons aged >80 years, efficacy against zoster was 18% (Table 2), but efficacy against PHN (39%) was
better retained (186). No significant differences by sex were observed in the efficacy of the vaccine at reducing BOI, PHN,
or zoster (4). No evidence indicated that the vaccine was less efficacious for prevention of zoster (vaccine efficacy:
51.6%; 95% CI = 41.4--60.1), PHN (vaccine efficacy: 60.9%; 95% CI = 31.3--78.7), or for reduction in BOI (vaccine
efficacy: 60.1%; 95% CI = 46.1--70.4) among subjects with functional limitations
(188).
Twelve clinical lots of zoster vaccine were used in the Shingles Prevention Study, nine of which were heat treated
to accelerate aging of the vaccine. Potency upon shipment to study sites ranged from 21,000--62,000 PFUs/dose,
but potency and accelerated aging did not significantly influence vaccine efficacy with regard to zoster, PHN, or
BOI.
Immunogencity
A substudy of the Shingles Prevention Study was conducted among 1,395 persons to assess VZV-specific
immunity at baseline and 6 weeks following administration of zoster vaccine or placebo. The longer-term duration of
immunogenicity also was assessed. Anamnestic antibody response was evaluated using gpELISA to measure increases in VZV
antibody levels after vaccination. RCF and IFN-g ELISPOT were used to measure the number of memory
T-cells. With all three assays, VZV-specific immunity measured 6 weeks after vaccination increased following receipt of vaccine but
not placebo. In both vaccine and placebo recipients, immune responses were inversely related to the risk for
developing zoster; this association with protection was greatest for anamnestic antibody response following vaccination for
which gpELISA Geometric Mean Titers (GMTs) increased 1.7-fold (95% CI = 1.6--1.8). However, for all three assays,
no threshold level of immunity that predicted complete protection from zoster was observed.
No clear dose response for increases in GMTs was
observed; similar increases were achieved in
vaccine recipients throughout the dosage range used in the Shingles Prevention Study
(189). Peak CMI responses were present 1--3 weeks following vaccination
(187,190,191), as would be expected for anamnestic responses that would occur
in persons with previous VZV infection. The impact of age on CMI response to vaccination also was evaluated. RCF
and IFN-g ELISPOT responses were greater in persons aged 60--69 years than in persons aged
>70 years (p<0.01) (192). The increase in GMTs as a measure of anamnestic antibody response in persons aged 50--59 years was comparable
to
that in persons aged >60 years
(193). In a prelicensure study, subjects aged 55--70 years acquired VZV-specific class
I-restricted and unrestricted cytotoxicity following vaccination with even low levels (4,000 PFUs) of either live or
heat-inactivated Oka/Merck strain of VZV
(23).
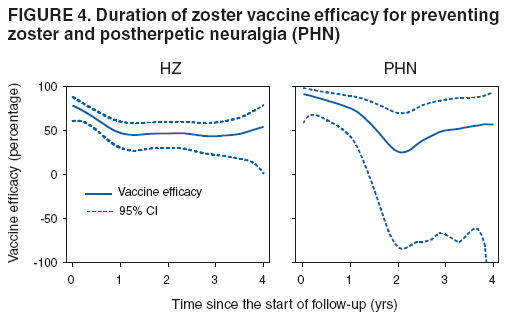
Duration of Efficacy and of Immunity
Vaccine efficacy for zoster prevention declined during the first year following vaccination, but remained stable
through the remaining 3 years of follow up (Figure 4). Vaccine efficacy for PHN prevention had a similar pattern, with an
initial decline and subsequent stabilization. After conclusion of the Shingles Prevention Study, approximately 7,500
vaccine recipients will be followed to extend observation to 10 years. Because placebo recipients were offered zoster vaccine
at the conclusion of the Shingles Prevention Study, zoster rates in these 7,500 persons will be compared with
historic controls. Increases in RCF and IFN-g ELISPOT
responses persisted for 3--6 years following vaccination
(192,194).
Safety and Adverse Events
Serious Adverse Events
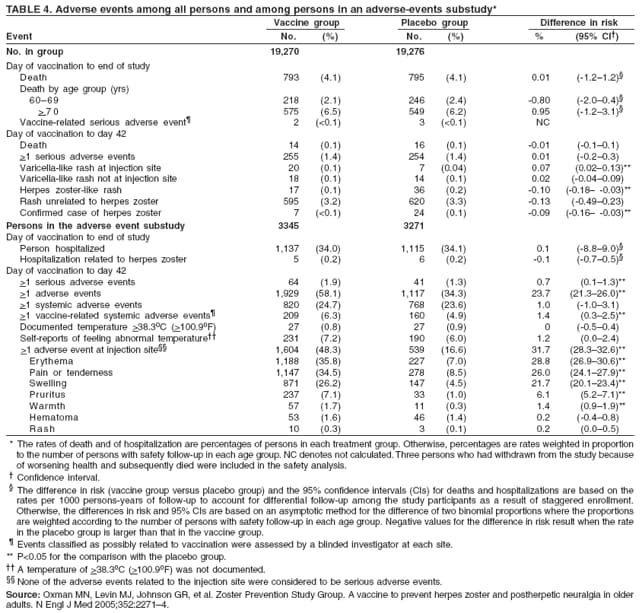
Adverse events were monitored in the Shingles Prevention Study population, with more comprehensive
ascertainment in a safety substudy comprising 6,616 persons (3,345 vaccine recipients and 3,271 placebo recipients)
(Table 4). In the Shingles Prevention Study population, the number and types of serious adverse events
(4) during the 42 days after receipt of vaccine or placebo were similar (1.4%). However, rates of serious adverse events in the safety substudy
were higher in vaccine recipients (1.9%) than in placebo recipients (1.3%), with a relative risk of 1.5 (95% CI =
1.0--2.3). Nonetheless, no temporal or clinical patterns of adverse events were observed in vaccine recipients to suggest a
causal relation (4,186). The incidence of death and hospitalizations was similar in the two treatment groups throughout
the observation time (4,186).
Mild Local and Systemic Reactions
In the Shingles Prevention Study safety substudy, self-reported injection site adverse events (e.g., erythema,
pain, swelling, warmth, and pruritis) were more common among vaccine recipients (48.3%) than placebo recipients
(16.6%) (p<0.05) (Table 4) (4); the risk for these events was higher in vaccine recipients aged 60--69 years (58.3%) than
in persons aged >70 years (41.3%)
(189). Most injection site adverse events were mild and resolved within 4 days
(187). Less-serious systemic adverse events, including headaches, were more common in vaccine recipients (6.3%) than
in placebo recipients (4.9%) (p<0.05) (Table 4)
(4). The risk for fevers after vaccination did not differ between
vaccine recipients and controls.
The safety and tolerability of zoster vaccine was evaluated in a separate study among persons aged 50--59
years, including 62 persons who received the standard potency (approximately 58,000 PFUs) and 123 persons
who received high potency (approximately 207,000 PFUs)
(195). Although the numbers of persons was small, both
vaccines were safe and well tolerated; however, injection site reactions were more common (69.4% and 82.9%,
respectively) than those observed in person aged
>60 years in the Shingles Prevention Study (48.3%).
Vaccine Virus Rash and Transmission
Varicella-like rashes, including injection site varicella-like lesions, generalized varicella-like rashes, and
zoster-like rashes, were evaluated in the Shingles Prevention Study during the first 42 days of observation (Table 4). Twenty
vaccine recipients and seven placebo recipients had lesions at the injection site (p<0.05)
(4); the lesions were tested for VZV by PCR in one of these persons in each group, and results were negative in both. Among the vaccine
recipients, lesions occurred a median of 3--4 days after
vaccination and lasted a median of 5 days.
Generalized varicella-like rashes occurred at similar rates in the two groups (Table 4). Zoster-like rashes were
less common in vaccine versus placebo recipients during this 42-day period (p<0.05). Oka/Merck strain VZV was
not detected in any of 10 lesion specimens from vaccine recipients available for PCR testing. In early studies conducted
as part of the manufacturer's clinical program for development of zoster vaccine, samples from rashes in two
vaccinated persons were confirmed to be Oka/Merck-strain VZV
(186). Both experienced noninjection-site varicella-like rashes;
one
had 21 lesions on day 17 lasting 8 days and the other developed five lesions on day 8 that lasted 16 days. No
varicella-like rashes were documented during any clinical zoster vaccine trials of laboratory-confirmed zoster
attributed to Oka/Merck strain VZV. In addition, no evidence existed of transmission of vaccine virus from vaccine recipients to contacts.
The Economic Burden of Zoster and Cost-Effectiveness of Vaccination
The economic burden of zoster in the elderly is substantial and includes direct costs attributed to health-care use
and indirect costs attributed to losses in productivity from temporary or more permanent disability. In addition, much of
the economic burden of zoster is borne by individual patients as reduced quality of life because of pain and
suffering. Certain studies provide a range of estimates for health-care use among persons aged
>60 years for treatment of zoster and PHN. The estimates vary widely
because of differing assumptions regarding the risk for PHN and of
complications resulting from zoster. Estimated health-care use per case of zoster ranges from 1.3--3.1 for the number of
outpatient visits, 0.005--0.12 for the number of emergency department visits, and 1--5 for the number of medications
prescribed. Approximately 1%--4% of zoster episodes result in hospitalization, with a mean duration of 4.8 days.
(196--199). Health-care use for zoster and PHN increases substantially with the age of patients
(196--198).
Costs associated with acute zoster have been evaluated. Among patients with acute episodes of zoster,
average expenditures ranged from $112--$287 per episode of outpatient care, $73--$180 per antiviral treatment, and
$3,221--$7,206 per hospitalization (2006 dollars). Additional costs associated with managing non-PHN complications
(e.g., ocular, neurologic, and cutaneous) ranged from $1,158--$11,255 per complication, and from $566--$1,914
per episode of PHN. Among the subset of patients with PHN persisting from 30 days to 12 months, annualized
health-care costs, including costs of the acute episode, ranged from $2,159 to $5,387
(200,201). Although indirect costs from death can occur with zoster, these costs
result mostly from losses in work time caused by temporary or more
permanent disability. Patients with zoster (including
those progressing to PHN) lose an average of >129 hours of work per
episode (197,198), including losses of 12 or more hours of work time and 69 hours of leisure time during the first 30
days (196). Data on the national economic impacts of zoster and its complications on
quality of life have not been reported.
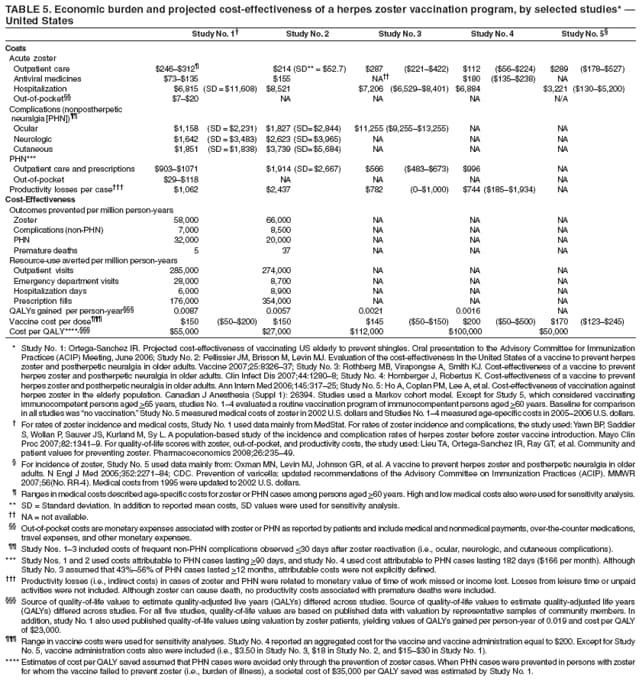
Five studies have estimated the cost-effectiveness of a
1-dose routine vaccination program of
immunocompetent persons aged >60 years
(196,197,199,202,203) (Table 5). One of these studies has not been published
(196). All five studies used a Markov cohort model
(105), followed a cost-utility analytic approach that included a societal
perspective (204,205), and used quality-adjusted life-year (QALY) scores to assess the incremental impact of the vaccine
program on quality of life. Costs and health benefits were measured in 2005--2006 U.S. dollars, and a 3% discount rate was used
to adjust health outcomes and costs. Model assumptions varied regarding duration of vaccine protection, the efficacy of
the vaccine for preventing PHN among vaccine recipients who developed zoster, costs associated with vaccine adverse
events, and costs attributed to losses in work productivity. None of the five models incorporated costs for losses in leisure
time. Assuming a routine vaccination program with 100% coverage, the estimated QALYs gained ranged from 0.0016
(0.6 days) to 0.0087 (3 days). At a vaccine cost of $150 per dose, the societal costs of routinely
vaccinating immunocompetent persons aged
>60 years range from $27,000 to $112,000 per QALY gained. In the
sensitivity analyses, variables with the strongest
influence on outcomes include vaccine costs, duration of vaccine efficacy, risks
for PHN as a complication, and costs and QALY scores for zoster and its complications.
Although costs per QALY gained are most appropriately used to prioritize among competing programs for purposes
of resource allocation, policymakers often decide whether or not to support programs by comparing their cost per
QALY against a standard threshold. A threshold suggested by the World Health Organization is three times the gross
domestic product per capita, which would be $94,431 for the United States
(206). Alternatively, policymakers often decide
about supporting programs by comparing their cost per QALY with the values for other widely accepted
interventions. Compilations of such cost effectiveness data have been published and maintained in on-line registries
(207,208). The estimated cost per QALY for zoster vaccination covers a wide range that appears acceptable in comparison to
either standard thresholds or to other established interventions, but it is at the intermediate-to-high end of that range.
Summary of Rationale for Zoster Vaccine Recommendations
The availability of a safe and effective vaccine for zoster offers an opportunity to decrease the burden of this disease
and its complications among persons with high levels of risk. In the United States, the vaccine is licensed for use
among persons aged >60 years, and routine vaccination of this population is recommended for several reasons. First,
zoster causes substantial morbidity in the United States, with approximately 1,000,000 new cases occurring annually
(62). Many of these cases cause debilitating pain, and when PHN develops, the pain can last for months or even years.
Other complications include involvement of the eye that can threaten sight, bacterial superinfections, and disfiguring
facial scarring. Second, although effective antiviral medications for treatment of zoster are available, administration must
be initiated within 72 hours of rash onset for maximum benefit. Many patients might not obtain such rapid diagnosis
and treatment, and even when they do, the treatment is only partially effective at alleviating the symptoms and
shortening their duration. Third, available treatments for PHN often do not completely alleviate the pain and might be
poorly tolerated by the older patients
(31,33). Finally, available evidence suggests the cost-effectiveness of zoster vaccine
is within the range of some other public health interventions.
In a large, placebo-controlled clinical trial, the zoster vaccine reduced BOI attributed to zoster by 61.1 % and
the incidence of PHN by 66.5 %. The vaccine reduced the overall incidence of zoster by 51.3 % and
substantially reduced its associated pain
(4). Although the vaccine was more efficacious in persons aged 60--69 years,
substantial efficacy against zoster was observed in persons aged
>70 years, and PHN was prevented in older age groups.
Prevention of zoster and its sequelae is particularly important among the oldest persons because they experience the
highest incidence of zoster and PHN, they might be least able to seek medical attention for zoster and PHN and to
request treatment of ongoing pain, they might be least able to tolerate the medications and procedures commonly used to
treat PHN, they might have the least reserve to tolerate zoster and its complications, and they are most likely to suffer
social and psychological consequences from PHN.
Recommendations for Use of Zoster Vaccine
Routine Vaccination of Persons Aged
>60 Years
ACIP recommends routine vaccination of all persons aged
>60 years with 1 dose of zoster vaccine. Persons who
report a previous episode of zoster and persons with chronic medical conditions (e.g., chronic renal failure, diabetes
mellitus, rheumatoid arthritis, and chronic pulmonary disease) can be vaccinated unless those conditions are contraindications
or precautions. Zoster vaccination is not indicated to treat acute zoster, to prevent persons with acute zoster
from developing PHN, or to treat ongoing PHN. Before routine administration of zoster vaccine, it is not necessary to
ask patients about their history of varicella (chickenpox) or to conduct serologic testing for varicella immunity.
Simultaneous Administration with Other Adult Vaccines
Immunogenicity of zoster vaccine and trivalent inactivated influenza vaccine is not compromised when the
two vaccines are administered simultaneously (186). However, no data exist on administration of zoster vaccine with
other vaccines routinely recommended for persons aged
>60 years, which are all inactivated. In general, the
simultaneous administration of most widely used live, attenuated and inactivated vaccines has not resulted in impaired
immune response or an increased rate of adverse events
(209). Therefore, zoster vaccine can be administered with
other indicated vaccines during the same visit (e.g., Td, Tdap, and pneumococcal polysaccharide vaccines). Each vaccine
must be administered using a separate syringe at a different anatomic site. If simultaneous administration is not
possible, zoster vaccine can be administered at any time before or after an inactivated vaccine, but at least 4 weeks before or
after another live, attenuated vaccine (209).
Groups for Which Vaccine is Not Licensed
Vaccination of Persons Aged <60 Years
The vaccine is not licensed for persons aged <60 years, and no recommendation exists for routine vaccination
of persons aged <60 years. In the clinical trial, the zoster vaccine was evaluated among persons aged
>60 years. The vaccine was most effective and well tolerated in the youngest persons (Table 1)
(4). Although the vaccine would probably be
safe and effective in persons aged <60 years, data are insufficient to recommend vaccination of these persons at this time.
Vaccination of Persons Who Have Received Varicella Vaccine
Zoster vaccination is not recommended for persons of any age who have received varicella vaccine. However,
health-care providers do not need to inquire about varicella vaccination history before administering zoster vaccine because
virtually all persons currently or soon to be in the recommended age group have not received varicella vaccine. In the
United States, varicella vaccination began in 1995. Since that time, few adults aged
>40 years would have been susceptible to varicella and thus eligible to receive varicella vaccine
(5). The number of persons eligible for zoster vaccination who
have received varicella vaccine is extremely small and will remain so for at least a decade.
Special Groups and Circumstances
Persons with a Reported History of Zoster
Persons with a reported history of zoster can be vaccinated. Repeated zoster has been confirmed in
immunocompetent persons soon after a previous episode
(4). Although the precise risk for and severity of zoster as a function of
time following an earlier episode are unknown, some studies suggest it may be comparable to the risk in persons without
a history of zoster (62,169). Furthermore, no laboratory evaluations exist to test for the previous occurrence of zoster,
and any reported diagnosis or history might be erroneous
(4,64,65). Although the safety and efficacy of zoster vaccine
have not been assessed in persons with a history of zoster, different safety concerns are not expected in this group.
Persons Anticipating Immunosuppression
The risk for zoster and its severe morbidity and mortality is much greater among persons who are
immunosuppressed. Review of vaccination status for zoster and other vaccines should be a key component of the medical assessment
for immunocompetent patients aged >60 years who might be anticipating initiation of immunosuppressive treatments
or who have diseases that might lead to immunodeficiency. Such patients without a history of zoster vaccination
should receive 1 dose of zoster vaccine at the first possible clinical encounter while their immunity is intact. Zoster
vaccine should be administered at least 14 days before initiation of immunosuppressive therapy, although some
experts advise waiting 1 month after zoster vaccination to begin immunosuppressive therapy if delay is possible
(210).
Persons Receiving Antiviral Medications
Licensed antiviral medications active against members of the herpesvirus family include acyclovir, famciclovir,
and valacyclovir. These agents might interfere with replication of the live, VZV-based zoster vaccine. All three agents
have relatively short serum half-lives and are quickly cleared from the body. Persons taking chronic acyclovir, famciclovir,
or valacyclovir should discontinue these medications at least 24 hours before administration of zoster vaccine, if
possible (209). These medications should not be used for at least 14 days after vaccination, by which time the
immunologic effect should be established
(209).
Persons Receiving Blood Products
Zoster vaccine can be administered to persons at any time before, concurrent with, or after receiving blood or
other antibody-containing blood product because persons with a history of varicella indefinitely maintain high levels
of antibody to VZV, and the levels are comparable to those found in donated blood and antibody-containing
blood products (e.g., whole blood, packed red blood cells, and plasma immune globulin, hyperimmune globulin,
and intravenous immune globulin) (192,211).
Nursing Mothers
Most live vaccines, including varicella vaccine, are not secreted in breast milk
(209,212). Therefore, breast feeding is not a contraindication for zoster vaccination.
However, this situation will be extremely rare in the target age group
for this vaccine.
Contraindications
Allergy to Vaccine Components
Zoster vaccine is contraindicated for persons who have a history of anaphylactic reaction to any component of
the vaccine, including gelatin and neomycin. Neomycin allergy is usually manifested as a contact dermatitis,
which represents a delayed-type immune response. A history of contact dermatitis to neomycin is not a contraindication
for receiving zoster vaccine (209).
Immunocompromised Persons
Zoster vaccine should not be administered to persons with primary or acquired immunodeficiency including:
Persons with leukemia, lymphomas, or other malignant neoplasms affecting the bone marrow or lymphatic
system. However, patients whose leukemia is in remission and who have not received chemotherapy (e.g., alkylating drugs
or antimetabolites) or radiation for at least 3 months can receive zoster vaccine
(209).
Persons with AIDS or other clinical manifestations of HIV, including persons with CD4+ T-lymphocyte values
<200 per mm3 or <15% of total lymphocytes.
Persons on immunosuppressive therapy, including high-dose corticosteroids
(>20 mg/day of prednisone or equivalent) lasting two or more weeks. Zoster vaccination should be deferred for at least 1 month
after discontinuation of such therapy (209). Short-term corticosteroid therapy (<14 days); low-to-moderate dose
(<20 mg/day of prednisone or equivalent); topical (e.g., nasal, skin, inhaled); intra-articular, bursal, or tendon
injections; or long-term alternate-day treatment with low to moderate doses of short-acting systemic corticosteroids are
not considered to be sufficiently immunosuppressive to cause concerns for vaccine safety. Persons receiving this dose
or schedule can receive zoster vaccine. Therapy with low-doses of methotrexate
(<0.4 mg/Kg/week), azathioprine
(<3.0 mg/Kg/day), or 6-mercaptopurine
(<1.5 mg/Kg/day) for treatment of rheumatoid arthritis, psoriasis,
polymyositis, sarcoidosis, inflammatory bowel disease, and other conditions are also not considered
sufficiently immunosuppressive to create vaccine safety concerns and are not contraindications for administration of
zoster vaccine.
Persons with clinical or laboratory evidence of other unspecified cellular immunodeficiency. However, persons
with impaired humoral immunity (e.g., hypogammaglobulinemia or dysgammaglobulinemia) can receive zoster vaccine.
Persons undergoing hematopoietic stem cell transplantation (HSCT). The experience of HSCT recipients with
VZV-containing vaccines (e.g., zoster vaccine) is limited. Physicians should assess the immune status of the recipient on
a case-by-case basis to determine the relevant risks. If a decision is made to vaccinate with zoster vaccine, the
vaccine should be administered at least 24 months after transplantation
(209).
Persons receiving recombinant human immune mediators and immune modulators, especially the antitumor necrosis factor agents adalimumab, infliximab, and etanercept. The safety and efficacy of zoster
vaccine administered concurrently with these agents is
unknown. If it is not possible to administer zoster vaccine to
patients before initiation of therapy, physicians should assess the immune status of the recipient on a case-by-case basis
to determine the relevant risks and benefits. Otherwise, vaccination with zoster vaccine should be deferred for at least
1 month after discontinuation of such therapy.
Pregnancy
Zoster vaccine is not recommended for use in pregnant women, although these women are unlikely to be in
the vaccine target age group. The effects of the live, attenuated VZV-based zoster vaccine on the fetus are unknown.
Women should avoid becoming pregnant for 4 weeks following zoster vaccination. Having a pregnant household member is not
a
contraindication to zoster vaccination. If a pregnant woman is vaccinated or becomes pregnant within 1 month
of vaccination, she should be counseled about potential effects on the fetus. Wild-type VZV poses a small risk to the
fetus (3), and the fetal risk from the attenuated zoster vaccine is probably even lower. Furthermore, virtually all
persons receiving the vaccine will have preexisting VZV immunity, which is expected to limit viral replication and
presumably further reduce fetal risk. In most circumstances, the decision to terminate a pregnancy should not be based on
whether zoster vaccine was administered during pregnancy. Merck & Co., Inc., in collaboration with CDC, has established
a pregnancy registry to monitor the maternal-fetal outcomes of pregnant women who are inadvertently administered
live-attenuated VZV-based vaccines within 1 month of pregnancy (telephone: 800-986-8999). Patients and
health-care providers should report any exposure to zoster vaccine during pregnancy to this registry.
Precautions
Moderate to Severe Illness
Zoster vaccination of persons who have severe acute illness should be postponed until recovery. The decision to
delay vaccination depends on the severity of symptoms and the etiology of the disease. Zoster vaccine can be administered
to persons who have mild acute illnesses with or without
fever (209).
Program Implementation Issues
Following Good Adult Vaccination Practices
Zoster vaccine should be offered to patients aged
>60 years at the first available clinical encounter with their
provider. The average adult in this age group has 5--8 clinical encounters with their provider annually
(213). Strategies to promote zoster vaccination include linking delivery of zoster vaccine to delivery of other indicated adult vaccines
(e.g., influenza) and preventive-health interventions
(214--217), standing orders so that patients will automatically be
offered indicated vaccines rather than requiring case-by-case physicians' orders
(218), and practice-based audits and/or physician-reminder systems
(218). Residents of nursing homes and other long-term--care facilities who are at least
aged 60 years and without contraindications should be included in routine zoster vaccination activities. When
administering zoster vaccine, health-care providers should review the patient's vaccination status for all indicated adult
vaccines (219,220).
ACIP recommends that health-care providers keep permanent documentation of all administered vaccines,
including zoster vaccine, in the vaccine recipient's permanent medical record
(209). The type of the vaccine,
manufacturer, anatomic site, route of delivery, date of administration, lot number, and name of the administering facility should
be recorded. To help avoid the administration of unnecessary doses, every patient should be given a record of
the vaccination.
Administration Errors
The zoster vaccine, ZOSTAVAX®, is a live, attenuated vaccine containing Oka/Merck strain VZV. The vaccine
is similar to the varicella vaccine,
VARIVAX®, except the minimum PFU-content of the
ZOSTAVAX® is at least 14-fold higher than the minimum PFU-content of
VARIVAX®. Opportunities for administration errors are possible.
For providers who serve both children and adults, physical separation of products, careful visual inspection and
reading of labels, and preparation of vaccine for patient use only at time of vaccination can help prevent errors. If a
provider mistakenly administers high-potency zoster vaccine to a child indicated for varicella vaccine, the level of
protection against varicella would probably be at least the same as for conventional doses of varicella vaccine. This
erroneous dose should count as a single valid dose of varicella vaccine. If the erroneous dose was administered in lieu of the first dose
of varicella vaccine, a second dose of varicella vaccine is required. Administration errors involving zoster vaccine should
be reported to VAERS whether or not an adverse event occurs.
Early clinical trials for prevention of varicella were conducted in susceptible children using a formulation of
live-attenuated Oka/Merck strain VZV at doses of 17,430 PFU, approaching the range of PFU in zoster vaccine
(>19,400 PFU). This high-dose formulation was well tolerated and efficacious
(221). The more recently licensed live,
attenuated
Oka-strain VZV vaccine (PROQUAD®) prepared in combination with measles, mumps, and rubella vaccine
(MMRV) is formulated with a broad range of titers that extend to over 60,000 PFU
(222,223).
Varicella vaccine (VARIVAX®) is not indicated for prevention of zoster. MMRV vaccine
(PROQUAD®) is not licensed for use in persons aged
>13 years. If a provider mistakenly administers varicella vaccine to persons indicated for
zoster vaccine, no specific safety concerns exists, but the dose should not be considered valid and the
patient should be administered a dose of zoster vaccine during that same visit. If the error is not immediately detected, a dose of
zoster vaccine should be administered as soon as possible but not within 28 days of the varicella vaccine dose to
prevent potential interference of 2 doses of live attenuated
virus.
Risk for Transmission of Oka/Merck Strain after Receiving Zoster Vaccine
Persons having close household or occupational contact with persons at risk for severe varicella need not take
any precautions after receiving zoster vaccine except in rare
instances in which a varicella-like rash develops, when
standard contact precautions are adequate. Although
transmission of Oka/Merck strain VZV has been documented
following varicella vaccination, such transmission is rare and has only been documented when the vaccine recipient first
developed a varicella-like rash. Rates of varicella-like rash appear to be less common following zoster vaccination than
following varicella vaccination (4), and transmission of the Oka/Merck strain VZV from recipients of zoster vaccine has not
been detected. The risk for transmitting the attenuated
vaccine virus to susceptible persons should be weighed against the
risk for developing wild-type zoster that could be transmitted to a susceptible person. If a susceptible,
immunocompromised person is inadvertently exposed to a person who has a
vaccine-related rash, VARIZIG™ need not be
administered because disease associated with this type of transmission is expected to be mild. Acyclovir, valacyclovir, and
famciclovir are active against live-attenuated Oka/Merck strain VZV and can be used in the unlikely situations in which a
severe illness develops in the susceptible contact.
Reporting of Adverse Events after Vaccination
As with any newly licensed vaccine, surveillance for rare adverse events associated with administration of zoster
vaccine is important for assessing its safety in widespread use. Vaccine safety surveillance in the age group for which
zoster vaccine is recommended (aged >60 years) will present challenges because of the high prevalence of chronic
conditions, the frequent use of multiple medications, and the common occurrence of medical events. Coincident adverse events
can be anticipated following zoster vaccination, but many of these could be caused by the vaccine as well. All
clinically significant adverse events should be reported to VAERS even if causal relation to vaccination is not certain.
VAERS reporting forms and information are available electronically at
http://www.vaers.hhs.gov or by telephone
(800-822-7967). Web-based reporting is also available, and providers are encouraged to report electronically at
https://secure.vaers.org/VaersDataEntryintro.htm.
Future Research and Directions
Key questions remain regarding optimal implementation of zoster vaccination and preventing zoster and
its complications. Areas that need particular focus include:
Surveillance for zoster and its complications. Zoster is not a notifiable condition. Other strategies will be needed
to monitor zoster and its complications include using administrative databases, population-based surveys, or
active surveillance in sentinel sites. Because the primary disease burden associated with zoster is pain, capturing
this condition will be particularly challenging using any surveillance strategy.
Durability of protection against zoster and its complications afforded by the zoster vaccine. In a persistence substudy ongoing at 12 of 22 of the original zoster vaccine study sites, follow up of vaccine recipients will be extended to
an observation time of 10 years. However, no concurrent randomized placebo group exists to which these
vaccine recipients can be compared, and results will be compared against historic controls. Large administrative
databases also will be important in evaluating changes in vaccine effectiveness over time. These and other available data
will help to determine changes in vaccine policy (e.g. a booster dose). However, both of these approaches might
be confounded by secular changes in the incidence of zoster.
Increased understanding of the epidemiology of zoster. Better knowledge of age-adjusted changes in the incidence
of zoster and risk factors for any such changes will help determine the long-term effectiveness of the zoster vaccine
and clarify whether changes in VZV circulation caused by varicella vaccination might be
affecting zoster incidence. A better understanding of the epidemiology and risk factors for zoster might also lead to changes in policy
regarding use of zoster vaccine (e.g., targeting the vaccine to selected risk groups that are not now covered by the
vaccine recommendations or lowering the targeted age group). Additional information is needed to define risks for zoster
in varicella-vaccinated adults attributed to Oka/Merck strain VZV from the vaccine itself or to wild-type VZV
from breakthrough varicella. Although studies involving both immunocompromised and immunocompetent
children provided evidence that the risks for zoster are lower in varicella-vaccinated children than in children with
naturally acquired varicella (3,99,100,224), characterization of these risks in older adults will involve longer follow up.
Better prevention and treatment strategies for zoster and PHN. Although licensure of zoster vaccine represents
an important milestone in prevention of zoster, the vaccine remains only partially efficacious and is not licensed for
all populations and age groups at risk. Although available treatments for zoster and PHN have improved, treatment
of these conditions remains inadequate. Improved prevention and treatment strategies, including better vaccines,
are needed to reduce the disease burden of zoster.
ZOSTAVAX® or other active or inactive formulations of zoster
vaccine should be evaluated in additional cohorts of persons (e.g., persons aged 50--59 years and
immunosuppressed persons at the highest risk for zoster and its complications). Patients infected with HIV, with or without
AIDS, could benefit substantially from the prevention of zoster. A better understanding of immunologic correlates
of protection against zoster would help facilitate the development and evaluation of such new zoster
prevention strategies.
The epidemiology of zoster in persons with a history of varicella vaccination. Available data suggest that
children vaccinated with varicella vaccines are at reduced risk for Oka/Merck strain zoster as compared with the risk for
zoster from wild-type VZV in children with a history of chickenpox. However, this evidence does not extend to
vaccine recipients as they become older. Nor does it include decades of time after vaccination, particularly in the absence
of circulating VZV that could externally boost immunity. Data also are lacking
regarding the risk for zoster from wild-type VZV in vaccinated persons with a history of breakthrough varicella. These issues should be addressed in
future studies to develop zoster vaccination policy for cohorts of vaccine recipients as they age.
Safety of zoster vaccination. Postlicensure studies to evaluate further the safety of the zoster vaccine
are under development and will be conducted by the manufacturer. Clinical trials have been completed to assess
the safety and immunogenicity of simultaneous administration of zoster vaccine and formulations of influenza
vaccine. In addition, independent studies are being developed by CDC to monitor safety through VAERS and the
CDC Vaccine Safety Datalink.
Additional Information About Zoster and Zoster Vaccine
Additional information about zoster and zoster vaccine is available from several sources, and new information will
be available in the future. Updated information about zoster, PHN, and zoster vaccine is available at
http://www.cdc.gov/vaccines/vpd-vac/shingles/default.htm.
Acknowledgments
Gregory S. Wallace, MD, Mary Mulholland, MA, Immunization Services Division, National Center for Immunization and
Respiratory Diseases, CDC, assisted in writing the section on vaccine storage and handling. Meredith Reynolds, PhD, Division of Viral Diseases,
National Center for Immunization and Respiratory Diseases, CDC, assisted with compiling and preparing data on economics. Aisha O. Jumaan,
PhD, MPH, Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC, assisted in writing material related to
the risk of postherpetic neuralgia. Sandra S. Chaves, M.D., M.Sc., assisted in preparing the section on adverse events from zoster vaccine.
Jessica Leung, MPH, and Adriana Lopez, Division of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC, helped
with graphs and tables.
Oxman MN, Levin MJ, Johnson GR, et al. A vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. N Engl J
Med 2005;352:2271--84.
Kilgore PE, Kruszon-Moran D, Seward JF, et al. Varicella in Americans from NHANES III: implications for control through routine
immunization. J Med Virol 2003;70 Suppl 1:S111--8.
Arvin A. Varicella-zoster virus. Clin Microbiol Rev 1996;9:361--81.
Gilden DH, Dueland AN, Devlin ME, Mahalingam R, Cohrs R. Varicella-zoster virus reactivation without rash. J Infect Dis 1992;166
(Suppl 1):S30--4.
Cohrs RJ, Randall J, Smith J, et al. Analysis of individual human trigeminal ganglia for latent herpes simplex virus type 1 and
varicella-zoster virus nucleic acids using real-time PCR. J Virol 2000;74:11464--71.
Levin MJ, Cai GY, Manchak MD, Pizer LI. Varicella-zoster virus DNA in cells isolated from human trigeminal ganglia. J Virol 2003;77:6979--87.
Wang K, Lau TY, Morales M, Mont EK, Straus SE. Laser-capture microdissection: refining estimates of the quantity and distribution of
latent herpes simplex virus 1 and varicella-zoster virus DNA in human trigeminal ganglia at the single-cell level. J Virol 2005;79:14079--87.
Gershon AA, LaRussa P, Steinberg S. The varicella vaccine. Clinical trials in immunocompromised individuals. Infect Dis Clin North
Am 1996;10:583-94.
Arvin A. Aging, immunity, and the varicella--zoster virus. N Engl J Med 2005;352:2266--7.
Hope-Simpson RE. Postherpetic neuralgia. J R Coll Gen Pract 1975;25:571--5.
Krause PR, Klinman DM. Varicella vaccination: evidence for frequent reactivation of the vaccine strain in healthy children. Nat Med
2000;6:451--4.
Thomas SL, Wheeler JG, Hall AJ. Contacts with varicella or with children and protection against herpes zoster in adults: a case-control
study. Lancet 2002;360:678--82.
Arvin AM, Koropchak CM, Wittek AE. Immunologic evidence of reinfection with varicella-zoster virus. J Infect Dis 1983;148:200--5.
Arvin A M. Cell-mediated immunity to varicella-zoster virus. J Infect Dis 1992;166:S35--41.
Wilson A, Sharp M, Koropchak CM, Ting SF, Arvin AM. Subclinical varicella-zoster virus viremia, herpes zoster, and T lymphocyte immunity
to varicella-zoster viral antigens after bone marrow transplantation. J Infect Dis 1992;165:119--26.
Hayward A, Levin M, Wolf W, Angelova G, Gilden D. Varicella-zoster virus-specific immunity after herpes zoster. J Infect Dis 1991;163:873--5.
Webster A, Grint P, Brenner MK, Prentice HG, Griffiths PD. Titration of IgG antibodies against varicella zoster virus before bone
marrow transplantation is not predictive of future zoster. J Med Virol 1989;27:117--9.
Burke BL, Steele RW, Beard OW, Wood JS, Cain TD, Marmer DJ. Immune responses to varicella--zoster in the aged. Arch Intern
Med 1982;142:291--3.
Levin MJ, Smith JG, Kaufhold RM, et al. Decline in varicella-zoster virus (VZV)-specific cell-mediated immunity with increasing age and
boosting with a high-dose VZV vaccine. J Infect Dis 2003;188:1336--44.
Hayward AR, Buda K, Jones M, White CJ, Levin MJ. Varicella zoster virus-specific cytotoxicity following secondary immunization with live
or killed vaccine. Viral Immunol 1996;9:241--5.
Thomas SL, Wheeler JG, Hall AJ. Case-control study of the effect of mechanical trauma on the risk of herpes zoster. BMJ 2004;328:439.
Gilden DH, Dueland AN, Cohrs R, Martin JR, Kleinschmidt-DeMasters BK, Mahalingam R. Preherpetic neuralgia. Neurology 1991;41:1215--8.
Kost RG, Straus SE. Postherpetic neuralgia---pathogenesis, treatment, and prevention. N Eng J Med 1996;335:32--42.
Glynn C, Crockford G, Gavaghan D, Cardno P, Price D, Miller J. Epidemiology of zoster. J R Soc Med 1990;83:617--9.
Gnann JW, Jr. Varicella-zoster virus: atypical presentations and unusual complications. J Infect Dis 2002;186:S91--8.
Gilden DH, Kleinschmidt-DeMasters BK, LaGuardia JJ, Mahalingam R, Cohrs RJ, Neurologic Complications of the reactivation of
varicella--zoster virus. N Engl J Med 2000;342:635--45.
Dworkin RH, Johnson RW, Breuer J, et al. Recommendations for the
management of herpes zoster. Clin Infect Dis 2007;44 (Suppl 1):S1--26.
Katz J, Cooper EM, Walther RR, Sweeney EW, Dworkin RH. Acute pain in herpes zoster and its impact on health-related quality of life.
Clin Infect Dis 2004;39:342--8.
Schmader K. Herpes zoster in the elderly: issues related to geriatrics. Clin Infect Dis 1999;28:736--9.
Fishbain DA. The association of chronic pain and suicide. Semin Clin Neuropsychiatry 1999;4:221--7.
Schmader K. Postherpetic neuralgia in immunocompetent elderly people. Vaccine 1998;16:1768--70.
Jung BF, Johnson RW, Griffin DR, Dworkin RH. Risk factors for postherpetic neuralgia in patients with herpes zoster. Neurology
2004;62:1545--51.
Chidiac C, Bruxelle J, Daures JP, et al. Characteristics of patients with herpes zoster on presentation to practitioners in France. Clin Infect
Dis 2001;33:62--9.
Scott FT, Leedham-Green ME, Barrett-Muir WY, et al. A study of zoster and the development of postherpetic neuralgia in East London. J
Med Virol 2003;(Suppl 1):S24--30.
Ragozzino MW, Melton LJ 3rd, Kurland LT, Chu CP, Perry HO. Population-based study of herpes zoster and its sequelae. Medicine
1982;61:310--6.
Shaikh S, Ta CN. Evaluation and management of herpes zoster ophthalmicus. Am Fam Physician 2002;66:1723--30.
Pavan Langston D. Herpes zoster ophthalmicus. Neurology 1995;45:50--1.
Adour KK. Otological complications of herpes zoster. Ann Neurol 1994;35:S62--S64.
Braverman DL, Ku A, Nagler W. Herpes zoster polyradiculopathy. Arch Phys Med Rehabil 1997;78:880--2.
Vincent KD, Davis LS. Unilateral abdominal distension following herpes zoster outbreak. Arch Dermatol 1998;134;1168--9.
Thomas JE, Howard FM. Segmental zoster paresis---a disease profile. Neurology 1972;22:459--66.
Dolin R, Reichman RC, Mazur MH, Whitley RJ. Herpes zoster-varicella infections in immunosuppressed patients. Ann Intern Med
1978;89:375--88.
Tyring S, Belanger R, Bezwoda W, Ljungman P, Boon R, Saltzman RL. A randomized, double-blind trial of famciclovir versus acyclovir for
the treatment of localized dermatomal herpes zoster in immunocompromised patients. Cancer Invest 2001;19:13--22.
Gnann JW, Whitley RJ. Natural history and treatment of varicella-zoster virus in high-risk populations. J Hosp Infect 1991;18:317--29.
Merselis JG Jr, Kaye D, Hook EW. Disseminated herpes zoster: a report of 17 cases. Arch Intern Med 1964;113:679--86.
Goffinet DR, Glatstein EJ, Merigan TC. Herpes zoster-varicella
infections and lymphoma. Ann Intern Med 1972;76:235--40.
Whitley RJ, Soong SJ, Dolin R, Betts R, Linnemann C Jr, Alford CA Jr. Early vidarabine therapy to control the complications of herpes zoster
in immunosuppressed patients. N Engl J Med 1982;307:971--5.
Mazur MH, Dolin R. Herpes zoster at the NIH: a 20-year experience. Am J Med 1978;65:738--44.
Locksley RM, Flournoy N, Sullivan KM, Meyers JD. Infection with varicella-zoster virus after marrow transplantation. J Infect
Dis 1985;152:1172--81.
Rogers SY, Irving W, Harris A, Russell NH. Visceral varicella zoster infection after bone marrow transplantation without skin involvement and
the use of PCR for diagnosis. Bone Marrow Transplant 1995;15:805--7.
Buchbinder SP, Katz MH, Hessol NA, et al. Herpes zoster and human immunodeficiency virus infection. J Infect Dis 1992;166:1153--6.
Glesby MJ, Moore RD, Chaisson RE. Clinical spectrum of herpes zoster in adults infected with human immunodeficiency virus. Clin Infect
Dis 1995;21:370--5.
Vaughan-Jones SA, McGibbon DH, Bradbeer CS. Chronic verrucous varicella-zoster infection in a patient with AIDS. Clin Exp
Dermatol 1994;19:327--9.
Gilson IH, Barnett JH, Conant MA, Laskin OL, Williams J, Jones PG. Disseminated ecthymatous herpes varicella zoster virus infection in
patients with acquired immunodeficiency syndrome. J Am Acad Dermatol 1989;20:637--42.
Ormerod LD, Larkin JA, Margo CA, et al. Rapidly progressive herpetic retinal necrosis: a blinding disease characteristic of advanced AIDS.
Clin Infect Dis 1998;26:34--45.
Siwamogstham P. Kuansuwan C. Reichart PA. Herpes zoster in HIV infection with osteonecrosis of the jaw and tooth exfoliation. Oral
Diseases 2006;12:500--5.
Yawn BP, Saddier S, Wollan P, Sauver JS, Kurland M, Sy L. A
population-based study of the incidence and complications of herpes zoster
before zoster vaccine introduction. Mayo Clin Proc 2007;82:1341--9.
Opstelten W, van Loon AM, Schuller M, et al. Clinical diagnosis of herpes zoster in family practice. Ann Fam Med 2007;5:305--9.
Rubben A, Baron JM, Grussendorf-Conen EI. Routine detection of herpes simplex virus and varicella zoster virus by polymerase chain
reaction reveals that initial herpes zoster is frequently misdiagnosed as herpes simplex. Br J Dermatol 1997;137:259--61.
Kalman CM, Laskin OL. Herpes zoster and zosteriform herpes simplex virus infections in immunocompetent adults. Am J Med 1986;81:775--8.
Birch CJ, Druce JD, Catton MC, MacGregor L, Read T. Detection of varicella zoster virus in genital specimens using a multiplex polymerase
chain reaction. Sex Transm Infect 2003;79:298--300
Nahass GT, Goldstein BA, Zhu WY, Serfling U, Penneys NS, Leonardi CL. Comparison of Tzanck smear, viral culture, and DNA
diagnostic methods in detection of herpes simplex and varicella-zoster infection. JAMA 1992;268:2541--4.
Solomon AR, Rasmussen JE, Weiss JS. A comparison of the Tzanck smear and viral isolation in varicella and herpes zoster. Arch
Dermatol 1986;122:282--5.
Gnann JW Jr, Whitley RJ. Clinical practice: herpes zoster. N Engl J Med 2002;347:340--6.
Dahl H, Marcoccia J, Linde A. Antigen detection: the method of choice in comparison with virus isolation and serology for laboratory diagnosis
of herpes zoster in human immunodeficiency virus-infected patients. J Clin Microbiol 1997;35:347--9.
Coffin SE, Hodinka RL. Utility of direct immunofluorescence and virus culture for detection of varicella-zoster virus in skin lesions.
J Clin Microbiol 1995;33:2792--5.
Morens DM, Bregman DJ, West CM, et al. An outbreak of varicella-zoster virus infection among cancer patients. Ann Intern Med 1980;93:414--9.
Brunell PA, Gershon AA, Uduman SA, Steinberg S. Varicella-zoster immunoglobulins during varicella, latency, and zoster. J Infect
Dis 1975;132:49--54.
Harper DR, Kangro HO, Heath RB. Serological responses in varicella and zoster assayed by immunoblotting. J Med Virol 1988;25:387--98.
Wittek AE, Arvin AM, Koropchak CM. Serum immunoglobulin A antibody to varicella-zoster virus in subjects with primary varicella and
herpes zoster infections and in immune subjects. J Clin Microbiol 1983;18:1146--9.
Sawyer MH. Chamberlin CJ. Wu YN. Aintablian N. Wallace MR. Detection of varicella-zoster virus DNA in air samples from hospital rooms.
J Infect Dis 1994;169:91--4.
Josephson A, Gombert ME. Airborne transmission of nosocomial
varicella from localized zoster. J Infect Dis 1988;158:238--41.
Seiler HE. A study of herpes zoster particularly in relation to chickenpox. J Hyg 1949;47:253--62.
Wreghitt TG, Whipp J, Redpath C, Hollingworth W. An analysis of infection control of varicella-zoster virus infections in Addenbrooke's
Hospital Cambridge over a 5-year period, 1987--92. Epidemiol Infect 1996;117:165--71.
Behrman A, Schmid DS, Crivaro A, Watson B. A cluster of primary varicella cases among healthcare workers with false-positive varicella zoster
virus titers. Infect Control Hosp Epidemiol 2003;24:202--6.
Brunell PA, Argaw T. Chickenpox attributable to a vaccine virus contracted from a vaccinee with zoster. Pediatrics 2000;106:28.
Wreghitt TG, Whipp PJ, Bagnall J. Transmission of chickenpox to two intensive care unit nurses from a liver transplant patient with zoster. J
Hosp Infect 1992;20:125--6.
Lopez AS, Burnett-Hartman A, Nambiar R, et al. Transmission of a newly characterized strain of the varicella-zoster virus from a herpes
zoster patient in a long term care facility, West Virginia, 2004.
J Infect Dis 2008;197:646--53.
Seward JF, Zhang JX, Maupin TJ, Mascola L, Jumaan AO. Contagiousness of varicella in vaccinated cases: a household contact study.
JAMA 2004;292:704--8.
Kelly PW, Petruccelli BP, Stehr-Green P, Erickson RL, Mason CJ. The susceptibility of young adult Americans to vaccine-preventable infections:
a national serosurvey of US Army recruits. JAMA 1991;266:2724--9.
Alter SJ, Hammond JA, McVey CJ, Myers MG. Susceptibility to varicella-zoster virus among adults at high risk for exposure. Am J Infect
Control 1986;7:448--51.
Ferson MJ, Bell SM, Robertson PW. Determination and importance of varicella immune status of nursing staff in a children's hospital.
J Hosp Infect 1990;15:347--51.
Struewing JP, Hyams KC, Tueller JE, Gray GC. The risk of measles, mumps, and varicella among young adults: a serosurvey of US Navy and
Marine Corps recruits. Am J Public Health 1993;83:1717--20.
McKinney WP, Horowitz MM, Battiola RJ. Susceptibility of hospital-based health care personnel to varicella-zoster virus infections. Am J
Infect Control 1989;17:26--30.
Brunell PA, Kotchmar GS Jr. Zoster in infancy: failure to maintain
virus latency following intrauterine infection. J Pediatr 1981;98:71--3.
Baba K, Yabuuchi H, Takahashi M, et al. Increased incidence of herpes zoster in normal children infected with varicella zoster virus
during infancy: community-based follow-up study. Pediatr 1986;108:372--7.
Terada K, Kawano S, Yoshihiro K, Miyashima H, Morita T. Characteristics of herpes zoster in otherwise normal children. Pediatr Infect Dis
J. 1993;12:960--1.
Nikkels AF, Nikkels-Tassoudji N, Pierard GE. Revisiting childhood herpes zoster. Pediatr Dermatol 2004;21:18--23.
Thomas SL, Hall AJ. What does epidemiology tell us about risk factors for herpes zoster? Lancet Infect Dis 2004;4:26--33.
Ross RT, Nicolle LE, Cheang M. Varicella zoster virus and multiple
sclerosis in a Hutterite population. J Clin Epidemiol 1995;48:1319--24.
Takayama N, Takayama M, Takita J. Herpes zoster in healthy children immunized with varicella vaccine. Pediatr Infect Dis J 2000;19:169--70.
Hardy IB, Gershon A, Steinberg S, et al. The incidence of zoster after immunization with live attenuated varicella vaccine. A study in
children with leukemia. N Engl J Med 1991;325:1545--50.
Black S, Shinefield H, Ray P, et al. Postmarketing evaluation of the safety and effectiveness of varicella vaccine. Pediatr Infect Dis J
1999;18:1041--6.
Fleming DM, Cross KW, Cobb WA, Champion RS. Gender difference in the incidence of zoster. Epidemiol Infect 2004;132:1--5.
Insinga RP, Itzler RF, Pellissier JM. Acute/subacute herpes zoster: healthcare resource utilisation and costs in a group of US health
plans.Pharmacoeconomics 2007;25:155--69.
Jumaan AO, Yu O, Jackson LA, Bohlke K, Galil K, Seward JF.
Incidence of herpes zoster, before and after
varicella-vaccination-associated decreases in the incidence of varicella, 1992--2002.
J Infect Dis 2005;191:2002--7.
Brisson M, Edmunds WJ, Law B, et al. Epidemiology of varicella zoster virus infection in Canada and the United Kingdom. Epidemiol
Infect 2001;127,305--14.
Schmader K. Herpes zoster in older adults. Clin Infect Dis 2001;32:1481--6.
Berger R, Florent G, Just M. Decrease of the lymphoproliferative response to varicella-zoster virus antigen in the aged. Infect Immun
1981;32:24--7.
Berger R, Luescher D, Just M. Enhancement of varicella-zoster-specific immune responses in the elderly by boosting with varicella vaccine.
J Infect Dis 1984;149:647.
Choo PW, Galil K, Donahue JG, Walker AM, Spiegelman D, Platt R. Risk factors for postherpetic neuralgia. Arch Intern Med
1997;157:1217--24.
De Moragas JM, Kierland RR. The outcome of patients with herpes zoster. Arch Dermatol 1957;75:193--6.
Opstelten W, Van Essen GA, Schellevis F, Verheij TJ, Moons K. Gender as an independent risk factor for herpes zoster: a
population-based prospective. Ann Epidemiol 2006;1006;16:692--5.
Parker CJ, Morgan K, Dewey ME. Physical illness and disability among elderly people in England and Wales: The Medical Research
Council Cognitive Function and Ageing Study. J Epidemiol Community Health 1997;51:494--501.
Di Luzio Paparatti U, Arpinelli F, Visona G. Herpes zoster and its
complications in Italy: an observational survey. J Infect 1999;38:116.
Donahue JG. Choo PW. Manson JE. Platt R. The incidence of
herpes zoster. Arch Intern Med 1995;155:1605--9.
Schmader K., George L.K., Burchett B.M, Pieper CF. Racial differences in the occurrence of herpes zoster. J Infect Dis 1995;171:701--4.
Schmader K. George LK. Burchett BM. Hamilton JD. Pieper CF. Race and stress in the incidence of herpes zoster in older adults. J Am
Geriatr Soc 1998;46:973--7.
Garnett GP, Grenfell BT. The epidemiology of varicella-zoster virus infections: the influence of varicella on the prevalence of herpes
zoster. Epidemiol Infect 1992;108:513--28.
Zak-Prelich M, Borkowski JL, Alexander F, Norval M. The role of
solar ultraviolet irradiation in zoster. Epidemiol Infect 2002;129:593--7.
Gallerani M, Manfredini R. Seasonal variation in herpes zoster infection. Br J Dermatol 2000;142:588--9.
Rusthoven JJ, Ahlgren P, Elhakim T, et al. Varicella-zoster infection in adult cancer patients. A population study. Arch Intern
Med 1988;148:1561--6.
Dunst J, Steil B, Furch S, Fach A, Bormann G, Marsch W. Herpes zoster in breast cancer patients after radiotherapy. Strahlenther
Onkol 2000;176:513--6.
Guinee VF, Guido JJ, Pfalzgraf KA, et al. The incidence of herpes zoster in patients with Hodgkin's disease: an analysis of prognostic
factors. Cancer 1985;56:642--8.
Schimpff S, Serpick A, Stoler B, et al. Varicella-zoster infection in patients with cancer. Ann Intern Med 1972;76:241--54.
Sokal JE. Firat D. Varicella-zoster infection in Hodgkin's disease: clinical and epidemiological aspects. Am J Med 1965;39:452--63.
Rusthoven JJ. The risk of varicella-zoster infections in different
patient populations: a critical review. Transfus Med Rev 1994;8: 96--116.
Feld R. Evans WK. DeBoer G. Herpes zoster in patients with carcinoma of the lung. Am J Med 1982;73:795--801.
Wilson JF. Marsa GW. Johnson RE. Herpes zoster in Hodgkin's disease. Clinical, histologic, and immunologic correlations. Cancer
1972;29:461--5.
Arvin AM. Varicella-zoster virus: pathogenesis, immunity, and clinical management in hematopoietic cell transplant recipients. Biol Blood
Marrow Transplant 2000;6:219--30.
Schuchter LM, Wingard JR, Piantadosi S, Burns WH, Santos. GW, Saral R. Herpes zoster infection after autologous bone
marrow transplantation. Blood 1989;74:1424--7.
Gourishankar S, McDermid JC, Jhangri GS, Preiksaitis JK. Herpes zoster infection following solid organ transplantation: incidence, risk
factors and outcomes in the current immunosuppressive era. Am J Transplant 2004;4:108--15.
Luby JP. Ramirez-Ronda C. Rinner S. Hull A. Vergne-Marini P. A longitudinal study of varicella-zoster virus infections in renal
transplant recipients. J Infect Dis 1977;135:659--63.
Rand KH. Rasmussen LE. Pollard RB. Arvin A. Merigan TC. Cellular immunity and herpesvirus infections in cardiac-transplant
patients. N Engl J Med 1977;296:1372--7.
McNulty A, Li Y, Radtke U, et al. B. Herpes zoster and the stage and prognosis of HIV-1 infection. Genitourin Med 1997;73:467--70.
Veenstra J, Krol A, van Praag RM, et al. Herpes zoster, immunological deterioration and disease progression in HIV-1 infection.
AIDS 1995;9:1153--8.
Glesby MJ, Hoover DR, Tan T, et al. Herpes zoster in women with and at risk for HIV: data from the Women's Interagency HIV Study. J
Acquir Immune Defic Syndr 2004;37:1604--9.
Gebo KA, Kalyani R, Moore RD, Polydefkis M. The incidence of, risk factors for, and sequelae of herpes zoster among HIV patients in
the HAART era. JAIDS 2005;40:169--74.
Gershon AA, Mervish N, LaRussa P, et al. Varicella-zoster virus
infection in children with underlying human immunodeficiency virus infection.
J Infect Dis 1997;176:1496--500.
Kahl LE. Herpes zoster infections in systemic lupus erythematosus: risk factors and outcome. J Rheumatol 1994;21:84--6.
Nagasawa K, Yamauchi Y, Tada Y, Kusaba T, Niho Y, Yoshikawa H. High incidence of herpes zoster in patients with systemic lupus
erythematosus: an immunological analysis. Ann Rheumatic Dis 1990;49:630--3.
Kang TY, Lee HS, Kim TH, Jun JB, Yoo DH. Clinical and genetic risk factors of herpes zoster in patients with systemic lupus
erythematosus. Rheumatol Int 2005;25:97--102.
Manzi S, Kuller LH, Kutzer J, et al. Herpes zoster in systemic lupus erythematosus. J Rheumatol 1995;22:1254--8.
Moutsopoulos HM, Gallagher JD, Decker JL, Steinberg AD. Herpes zoster in patients with systemic lupus erythematosus. Arthritis
Rheum 1978;21:789--802.
Pope JE, Krizova A, Ouimet JM, Goodwin JL, Lankin M. Close association of herpes zoster reactivation and systemic lupus erythematosus
(SLE) diagnosis: case-control study of patients with SLE or noninflammatory nusculoskeletal disorders. J Rheumatol 2004;31:274--9.
Antonelli MA, Moreland LW, Brick JE. Herpes zoster in patients with rheumatoid arthritis treated with weekly, low-dose methotrexate. Am
J Med 1991;90:295--8.
Smitten AL, Choi HK, Hochberg MC, et al. The risk of herpes zoster in patients with rheumatoid arthritis in the United States and the
United Kingdom. Arthritis Rheum 2007;57:1431--8.
Wung PK, Holbrook JT, Hoffman GS, et al. Herpes zoster in immunocompromised patients: incidence, timing, and risk factors. Am J
Med 2005;118:1416.e9--e18.
Gupta G, Lautenbach E, Lewis JD. Incidence and risk factors for herpes zoster among patients with inflammatory bowel disease.
Clin Gastroenterol Hepatol 2006;4:1483--90.
Brown GR. Herpes zoster: correlation of age, sex, distribution,
neuralgia, and associated disorders. South Med J 1976;69:576--8.
Heymann AD, Chodick G, Karpati T, et al. Diabetes as a risk factor for herpes zoster infection: results of a population-based study in
Israel. Infection 2008;May 3. [Epub ahead of print].
Arndt V, Vine MF, Weigle K. Environmental chemical exposures and risk of herpes zoster. Environ Health Perspect 1999;107:835--41.
Ragozzino MW, Melton LJ, Kurland LT. Herpes zoster and diabetes mellitus: an epidemiological investigation. J Chronic Dis 1983;36:501--5.
Ross RT, Cheang M, Landry G, Klassen L, Doerksen K. Herpes zoster and multiple sclerosis. Can J Neurol Sci 1999;26:29--32.
Palmer SR, Caul EO, Donald DE, Kwantes W, Tillett H. An outbreak of zoster? Lancet 1985;2:1108--11.
Su WP. Muller SA. Herpes zoster. Case report of possible accidental inoculation. Arch Dermatol 1976;112:1755--6.
Brisson M, Gay NJ, Edmunds WJ, Andrews NJ. Exposure to varicella boosts immunity to herpes-zoster: implications for mass vaccination
against chickenpox. Vaccine 2002;20:2500--7.
Gershon A, LaRussa P, Steinberg S, Lo SH, Mervish N, Meier P. The protective effect of immunologic boosting against zoster: an analysis
in leukemic children who were vaccinated against chickenpox.
J Infect Dis 1996;173:450--3.
Schmader K, Studenski S, MacMillan J, Grufferman S, Cohen HJ. Are stressful life events risk factors for herpes zoster? J Am Geriatr
Soc 1990;38:1188--94.
Massad MG, Navarro RA, Rubeiz H, et al. Acute postoperative zoster after thoracic sympathectomy for hyperhidrosis. Ann Thorac
Surg 2004;78:2159--61.
Gilden DH, Katz RI. Surgical induction of zoster in a contralateral homologous dermatomal distribution. Arch Neurol 2003;60:616--7.
Andrews TR, Perdikis G, Shack RB. Herpes zoster as a rare complication of liposuction. Plast Reconstr Surg 2004;113:1838--40.
Walter R, Hartmann K, Fleisch F, Reinhart WH, Kuhn M. Reactivation of herpesvirus infections after vaccinations? Lancet 1999;353:810.
Thomas SL, Wheeler JG, Hall AJ. Micronutrient intake and the risk
of herpes zoster: a case-control study. Int J Epidemiol 2006;35:307--14.
Haanpaa M, Nurmikko T, Hurme M. Polymorphism of the IL-10 gene is associated with susceptibility to herpes zoster. Scand J Infect
Dis 2002;34:112--4.
Richards P. Shingles in one family practice. Arch Fam Med 1996;5:42--6.
Mullooly JP, Riedlinger K, Chun C, Weinmann S, Houston H.
Incidence of herpes zoster, 1997--2002. Epidemiol Infect 2005;133:245--53.
Yih WK, Brooks DR, Lett SM, et al. The incidence of varicella and herpes zoster in Massachusetts as measured by the Behavioral Risk
Factor Surveillance System (BRFSS) during a period of increasing varicella vaccine coverage, 1998--2003. BMC Public Health 2005;5:68.
Russell ML, Schopflocher DP, Svenson L, Virani SN. Secular trends in the epidemiology of shingles in Alberta. Epidemiol Infect
2007;135:908--13.
Perez-Farinos N, Ordobas M, Garcia-Fernandez C, et al. Varicella and herpes zoster in Madrid, based on the Sentinel General
Practitioner Network: 1997--2004. BMC Infect Dis 2007;7:59.
Molin L. Aspects of the natural history of herpes zoster: a follow-up investigation of outpatient material. Acta Derm-Venereol 1969;49:569--83.
Coplan P, Black S, Rojas C, et al. Incidence and hospitalization rates of varicella and herpes zoster before varicella vaccine introduction: a
baseline assessment of the shifting epidemiology of varicella disease. Pediatr Infect Dis J 2001;20:641--5.
Brisson M, Edmunds WJ. Epidemiology of varicella-zoster virus in England and Wales. J Med Virol 2003;70(Suppl 1):9--14.
Lin F, Hadler JL. Epidemiology of primary varicella and herpes zoster hospitalizations: the pre-varicella vaccine era. J Infect Dis
2000;181:1897--905.
MacIntyre CR, Chu CP, Burgess MA. Use of hospitalization and pharmaceutical prescribing data to compare the prevaccination burden
of varicella and herpes zoster in Australia. Epidemiol Infect 2003;131:675--82.
Chant KG, Sullivan EA, Burgess MA, et al. Varicella-zoster virus infection in Australia. Aust N Z J Public Health 1998;22:413--8.
Oh HM, Ho AY, Chew SK, Monteiro EH. Clinical presentation of
herpes zoster in a Singapore hospital. Singapore Med J 1997;38:471--4.
Schmader, KE. Herpes Zoster Epidemiology. In: Arvin A, Gershon A., eds. Varicella-Zoster Virus, Cambridge,
Massachusetts: Cambridge University Press, 2007.
Dworkin RH, Boon RJ, Griffin DR, Phung D. Postherpetic neuralgia: impact of famciclovir, age, rash severity and acute pain in herpes
zoster patients. J Infect Dis 1998;178:76--80S.
Wood MJ, Kay R, Dworkin RH, Soong SJ, Whitley RJ. Oral acyclovir therapy accelerates pain resolution in patients with herpes zoster: a
meta-analysis of placebo-controlled trials. Clin Infect Dis 1996;22:341--7.
Whitley RJ, Weiss H, Gnann JW Jr, et al. Acyclovir with and without prednisone for the treatment of herpes zoster: a randomized,
placebo-controlled trial. Ann Intern Med 1996;125:376--83.
Wood MJ, Johnson RW, McKendrick MW, Taylor J, Mandal BK, Crooks J. A randomized trial of acyclovir for 7 days or 21 days with and
without prednisolone for treatment of acute herpes zoster.
N Engl J Med 1994;330:896--900.
Dubinsky RM, Kabbani H, El-Chami Z, Boutwell C, Ali H. Practice parameter: treatment of postherpetic neuralgia: an evidence-based report
of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2004; 63:959--65.
Hempenstall K, Nurmikko TJ, Johnson RW, A'Hern RP, Rice AS. Analgesic therapy in postherpetic neuralgia: a quantitative systematic
review. PLoS Med 2005;2:e164.
Takahashi M, Otsuka T, Okuno Y, Asano Y, Yazaki T, Isomura S. Live vaccine used to prevent the spread of varicella in children in
hospital. Lancet 1974;2:1288--90.
Schmader K, Saddier P, Johnson G, et al. The effect of a zoster vaccine on interference of herpes zoster with activities of daily living
(ADL) [Abstract 859]. 44th Annual Meeting of IDSA, Oct. 12--15, 2006, Toronto..
Merck. An overview of herpes zoster/PHN and the Shingles Prevention Study for
Zostavax®. Presentation to the Advisory Committee
on Immunization Practices (ACIP) meeting; February 2006.
Schlienger K, Lange J, Tyring SK, et al. Immunogenicity, kinetics of VZV-Specific CD4+ T-cell g-IFN production and safety of a live
attenuated Oka/Merck zoster vaccine in healthy adults
>60 years of age [Abstract 857]. 44th Annual Meeting of IDSA, Oct. 12--15, 2006, Toronto.
Sperber SJ, Smith BV, Hayden FG.Serologic response and reactogenicity to booster immunization of healthy seropositive adults
with live or inactivated varicella vaccine. Antiviral Res 1992;17:213--22.
Oxman M, Levin M, Johnson G, Zhang J, Caulfield M. The effect of age on clinical and immunologic responses to a herpes zoster
vaccine [Abstract 858]. 44th Annual Meeting of IDSA, Oct. 12--15, 2006, Toronto.
Sutradhar SC, Wang WWB, Schlienger K, et al. Comparison of
immunogenicity and safety of
Zostavax® in adults 50 to 59 years old and
those >60 years old [Abstract S27]. 10th Annual Conference on Vaccine Research, April 30--May 2, 2007, Baltimore MD.
Levin MJ, Barber D, Goldblatt E, et al. Use of a live attenuated varicella vaccine to boost varicella-specific immune responses
in seropositive people 55 years of age and older: duration of booster effect. J Infect Dis 1998;17(Suppl 1)8:109--12.
Tyring SK, Diaz-Mitoma F, Padget LG, et al. Safety and tolerability of a high-potency zoster vaccine in adults
>50 years of age. Vaccine 2007;25:1877--83.
Ortega-Sanchez IR. Projected cost-effectiveness of vaccinating US elderly to prevent shingles. Oral presentation to the Advisory Committee
for Immunization Practices (ACIP) Meeting, June 2006.
Pellissier JM, Brisson M, Levin MJ. Evaluation of the
cost-effectiveness In the United States of a vaccine to prevent herpes zoster and
postherpetic neuralgia in older adults. Vaccine 2007;25:8326--37.
Insinga RP, Itzler RF, Pellissier JM, Saddier P, Nikas AA. The incidence of herpes zoster in a United States administrative database.
J Gen Intern Med 2005;20:748--53.
Rothberg MB, Virapongse A, Smith KJ. Cost-effectiveness of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults.
Clin Infect Dis 2007;44:1280--8.
Dworkin RH, White R, O'connor AB, Baser O, Hawkins K. Healthcare costs of acute and chronic pain associated with a diagnosis of
herpes zoster. J Am Geriatr Soc 2007;55:1168--75.
Dworkin RH, White R, O'Connor AB, Hawkins K. Health care expenditure burden of persisting herpes zoster pain. Pain Medicine
2008;9:348--53.
Hornberger J, Robertus K. Cost-effectiveness of a vaccine to prevent herpes zoster and postherpetic neuralgia in older adults. Ann Intern
Med 2006;145:317--25.
Ho A, Coplan PM, Lee A, et al. Cost-effectiveness of varicella zoster vaccination in older adults. Canadian J Anesthesia 2006 (Suppl 1): 26394.
Gold MR, Siegel JE, Russell LB, MC Weinstein. Cost-effectiveness in health and medicine. New York, New York: Oxford University Press, 1996.
Schwartz B, Ortega-Sanchez IR. Economic analyses of vaccines and vaccination programs. In: Levine MM, Woodrow GC, Kaper JB, Cobon
GA, eds. New Generation Vaccines. New York, New York: Marcel Dekker, 2004.
Neumann PJ, Rosen AB, Weinstein MC. Medicare and
cost-effectiveness analysis. N Engl J Med 2005;353:1516--22.
The CEA Registry. Tufts-New England Medical Center Institute for Clinical Research and Health Policy Studies. Available at
www.tufts-nemc.org/cearegistry.
Cheney C, Ramsdell JW. Effect of medical records' checklists on implementation of periodic health measures. Am J Med 1987;83: 129--36.
Cohen DI, Littenberg B, Wetzel C, Neuhauser D. Improving physician compliance with preventive medicine guidelines. Med Care
1982;20:1040--5.
Briss PA, Rodewald LE, Hinman AR, et al. Reviews of evidence regarding interventions to improve vaccination coverage in children,
adolescents, and adults: The Task Force on Community Preventive Services. Am J Prev Med 2000;18:97--140.
Gyorkos TW, Tannenbaum TN, Abrahamowicz M, et al. Evaluation of the effectiveness of immunization delivery methods. Can J Public
Health 1994;85(Suppl 1):S14-30.
Buffington J, Bell KM, LaForce FM, et al. A target-based model for increasing influenza immunizations in private practice. J Gen Intern
Med 1991;6:204--9.
Weibel RE, Neff BJ, Kuter BJ, et al. Live attenuated varicella virus vaccine. Efficacy trial in healthy children. N Eng J Med 1984;310:1409--15.
Shinefield H, Black S, Digilio L, et al. Evaluation of a quadrivalent measles, mumps, rubella and varicella vaccine in healthy children.
Pediatr Infect Dis J 2005;24:665--9.
Shinefield H, Black S, Williams WR, et al. Dose-response study of a quadrivalent measles, mumps, rubella and varicella vaccine in
healthy children. Pediatr Infect Dis J 2005;24:670--5.
Civen RH, Maupin TJ, Xiao H, Seward JF, Jumaan AO, Mascola L. A population based study of herpes zoster in children and adolescents
post-varicella licensure, Antelope Valley 2000--2003. 38th National Immunization Conference, Memphis, TN, May 2004.
Advisory Committee on Immunization Practices Shingles Work Group
Chair: John Treanor, MD, Rochester, New York.
Members: Members: William L. Atkinson, MD, MPH, Atlanta, Georgia; Jeffrey I. Cohen, MD, Bethesda, Maryland; Robert H. Dworkin,
PhD, Rochester, New York; Sandra Gambescia, Atlanta, Georgia; Paul M. Gargiullo, PhD, Atlanta, Georgia; Anne A. Gershon, MD, New York, New
York; John W. Glasser, PhD, MPH, Atlanta, Georgia; Dalya Güris, MD, MPH, Atlanta, Georgia; Penina Haber, MPH, Atlanta, Georgia; Rafael
Harpaz, MD, MPH, Atlanta, Georgia; Beth F. Hibbs, MPH, Atlanta, Georgia; John K. Iskander, MD, MPH, Atlanta, Georgia; Samuel L. Katz, MD,
Durham, North Carolina; Philip R. Krause, MD, Bethesda Maryland; Phillip S. LaRussa, MD, New York, New York; Myron J. Levin, MD, Denver,
Colorado; Tracy A. Lieu, MD, MPH, Boston, Massachusetts; Mona E. Marin, MD, MPH, Atlanta, Georgia; Kathleen M. Neuzil, MD, MPH,
Seattle Washington; Kristin Nichol, MD, MPH, MBA, Minneapolis, Minnesota; Ismael R. Ortega- Sánchez, PhD, Atlanta, Georgia; Gregory A. Poland,
MD, Rochester, Minnesota; Sara Rosenbaum, JD, Washington, DC; Tammy A. Santibanez, PhD; William Schaffner, MD, Nashville, Tennessee; Kenneth
E. Schmader, MD, Durham, North Carolina; D. Scott Schmid, PhD, Atlanta, Georgia; Jane Seward, MBBS, MPH, Atlanta, Georgia; Heather
Stafford, Philadelphia, Pennsylvania; Ray Strikas, MD, Washington, DC; Gregory S. Wallace, MD, Atlanta, Georgia; Barbara Watson, MB ChB,
Philadelphia, Pennsylvania.
Advisory Committee on Immunization Practices Membership List, June 2007
Chairman: Jon S. Abramson, MD, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
Executive Secretary: Larry K. Pickering, MD, CDC, Atlanta, Georgia.
Members: Ban Mishu Allos, MD, Vanderbilt University School of Medicine, Nashville, Tennessee; Carol Baker, MD, Baylor College of
Medicine, Houston, Texas; Robert L. Beck, JD, Palmyra, Virginia; Janet R. Gilsdorf, MD, University of Michigan, Ann Arbor, Michigan; Harry Hull,
MD, Minnesota Department of Health, Minneapolis, Minnesota; Susan Lett, MD, MPH, Massachusetts Department of Public Health, Jamaica
Plain, Massachusetts; Tracy Lieu, MD, MPH, Harvard Pilgrim Health Care and Harvard Medical School, Boston, Massachusettes; Dale L. Morse, MD,
New York State Department of Health, Albany, New York; Julia Morita, MD, Chicago Department of Public Health, Chicago, Illinois; Kathleen
Neuzil, MD, MPH, University of Washington, Seattle, Washington; Patricia Stinchfield, Children's Hospitals and Clinics, St. Paul, Minnesota; Ciro
Valent Sumaya, MD, MPH, Texas A&M University System Health Science Center, College Station, Texas; John J. Treanor, MD, University of
Rochester, Rochester, New York; and Robin J. Womeodu, MD, University of Tennessee Health Science Center, Memphis, Memphis, Tennessee.
Ex-Officio Members: James Cheek, MD, Indian Health Service, Albuquerque, New Mexico; Wayne Hachey, DO, Department of Defense,
Falls Church, Virginia; Geoffrey S. Evans, MD, Health Resources and Services Administration, Rockville, Maryland; Bruce Gellin, MD, National
Vaccine Program Office, Washington, DC; Linda Murphy, Centers for Medicare and Medicaid Services, Baltimore, Maryland; George T. Curlin, MD,
National Institutes of Health, Bethesda, Maryland; Norman Baylor, PhD, U.S. Food and Drug Administration, Rockville, Maryland; and Kristin Lee
Nichol, MD, Department of Veterans Affairs, Minneapolis, Minnesota. Liaison Representatives: American Academy of Family Physicians, Jonathan Temte, MD, Madison, Wisconsin, and Doug Campos-Outcalt,
MD, Phoenix, Arizona; American Academy of Pediatrics, Keith Powell, MD, Akron, Ohio, and Carol Baker, MD, Houston, Texas; America's
Health Insurance Plans, Andrea Gelzer, MD, Hartford, Connecticut; American College Health Association, James C. Turner, MD, Charlottesville,
Virginia; American College of Obstetricians and Gynecologists, Stanley Gall, MD, Louisville, Kentucky; American College of Physicians, Kathleen M.
Neuzil, MD, Seattle, Washington; American Medical Association, Litjen Tan, PhD, Chicago, Illinois; American Pharmacists Association, Stephan L.
Foster, PharmD, Memphis, Tennessee; Association of Teachers of Preventive Medicine, W. Paul McKinney, MD, Louisville, Kentucky; Biotechnology
Industry Organization, Clement Lewin, PhD, Cambridge, Massachusetts; Canadian National Advisory Committee on Immunization, Monica Naus,
MD, Vancouver, British Columbia; Healthcare Infection Control Practices Advisory Committee, Steve Gordon, MD, Cleveland, Ohio; Infectious
Diseases Society of America, Samuel L. Katz, MD, Durham, North Carolina; London Department of Health, David Salisbury, MD, London, United
Kingdom; National Association of County and City Health Officials, Nancy Bennett, MD, Rochester, New York, and Jeffrey S. Duchin, MD,
Seattle, Washington; National Coalition for Adult Immunization, David A. Neumann, PhD, Alexandria, Virginia; National Foundation for Infectious
Diseases, William Schaffner, MD, Nashville, Tennessee; National Immunization Council and Child Health Program, Romeo S. Rodriquez, Mexico City,
Mexico; National Medical Association, Patricia Whitley-Williams, MD, New Brunswick, New Jersey; National Vaccine Advisory Committee, Gary Freed,
MD, Swiftwater, Pennsylvania, and Peter Paradiso, PhD, Collegeville, Pennsylvinia; Society for Adolescent Medicine, Amy B. Middleman, MD,
Houston, Texas; Pharmaceutical Research and Manufacturers of America, Damian A. Araga, Swiftwater, Pennsylvania.
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services.References to non-CDC sites on the Internet are
provided as a service to MMWR readers and do not constitute or imply
endorsement of these organizations or their programs by CDC or the U.S.
Department of Health and Human Services. CDC is not responsible for the content
of pages found at these sites. URL addresses listed in MMWR were current as of
the date of publication.
All MMWR HTML versions of articles are electronic conversions from typeset documents.
This conversion might result in character translation or format errors in the HTML version.
Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr)
and/or the original MMWR paper copy for printable versions of official text, figures, and tables.
An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S.
Government Printing Office (GPO), Washington, DC 20402-9371;
telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to
mmwrq@cdc.gov.