|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
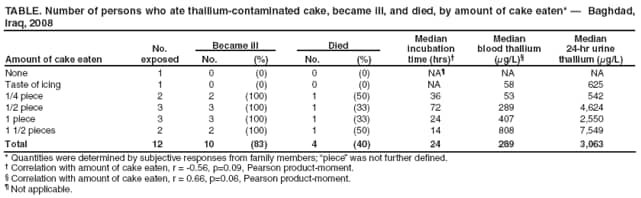
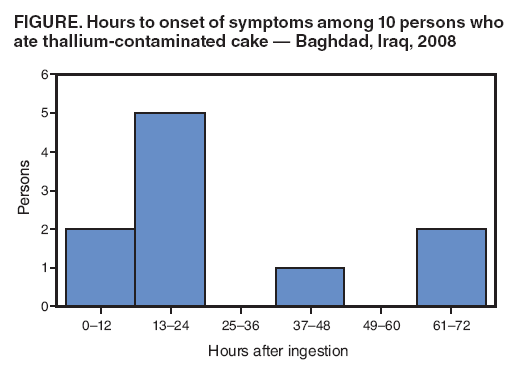
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Thallium Poisoning from Eating Contaminated Cake --- Iraq, 2008Thallium is an odorless, tasteless, heavy metal formerly used in rodenticides and still used in some manufacturing processes (e.g., electronics, pharmaceuticals, and glass). Thallium also has been used for intentional poisonings (1). Acute thallium poisoning produces gastrointestinal symptoms and signs, such as vomiting and acute abdominal pain, in the first few hours after ingestion, and initially is indistinguishable from other causes of acute gastrointestinal toxicity. However, within several days of ingestion, acute thallium poisoning often produces neurologic symptoms, such as extreme pain and acute muscle weakness ascending from the lower extremities, consistent with heavy metal toxicity (2). On January 22, 2008, 10 of 12 members in two families in Baghdad, Iraq, developed gastrointestinal symptoms; four of those 10 persons subsequently died from acute thallium poisoning, and five developed neurologic symptoms but survived. The Jordan Field Epidemiology Training Program* investigated this cluster at the request of the World Health Organization (WHO) representative in Iraq. The preliminary investigation indicated this was an intentional poisoning, and law enforcement officials began a criminal investigation. Physicians who see the sudden onset of painful peripheral neuropathy and hair loss in patients should consider the possibility of thallium poisoning. On January 22, 2008, 10 members of two families sought treatment at a health-care facility in Baghdad. All 10 of the ill patients were experiencing abdominal pain, vomiting, and dysphagia. Over the next 4 days, five of the patients developed neurologic symptoms and signs of varying severity (i.e., pain, abnormal sensations, and weakness, especially in the lower limbs). On January 26, the treating physician submitted specimens from the patients and a sample of a cake, which all 10 had eaten, to the poison testing laboratory of the Iraq Ministry of Health in Baghdad. On January 27, the WHO representative in Iraq was notified that the laboratory had detected thallium qualitatively in patient specimens and the cake. One of the patients, a child aged 11 years, died on January 30. On February 1, the nine surviving patients were evacuated to Amman, Jordan, to receive Prussian blue (ferric hexacyanoferrate) as an antidote for thallium poisoning, which was not available in Iraq. A second child, aged 2 years, died soon after arrival in Jordan, before therapy could begin. Prussian blue therapy was begun in the eight surviving patients 11 days after they had eaten the contaminated cake; however, two of the eight patients were already in coma with severe cerebral edema and subsequently died. Over the next 30 days, all six long-term survivors developed hair loss, and five of the six survivors developed muscle weakness and spasticity of the lower limbs, with differing severity. An epidemiologic investigation was initiated on February 5, 2008. Investigators learned that the fathers of the two families (family A and family B) were board members of an Iraqi sporting club. The board held a routine meeting in the club's conference room in Baghdad at midday on January 21. The cake, divided into 10 pieces, was prepared by a local bakery and delivered to the board meeting as a gift from a former board member. However, the cake arrived late, after most board members had departed. The board members who remained (the fathers of two families) divided the cake and took the halves home to their families. No cake was eaten at the board meeting; the cake was eaten at both families' homes after the evening meal on January 21. Family A was composed of seven members (father, mother, and five children); family B was composed of five members (father, mother, uncle, and two children). Ten cases of abdominal pain, vomiting, and dysphagia were identified among family members who consumed any portion of the cake on January 21. No other board members or their families reported illness, and no similar illnesses were found at the health facility in Baghdad or at nearby health facilities. The overall attack rate was 83% (10 of 12 persons): six of seven persons in family A and four of five persons in family B. Four patients died (case-fatality rate = 40%; family-specific fatality rates = 33% [two of six] for family A and 50% [two of four] for family B) (Table). Food exposure histories were collected in Jordan through interviews with family members. Ten persons who ate portions of the cake on January 21 became ill; neither of the two persons who did not eat cake became ill (relative risk = undefined, p=0.02, Fisher exact test). However, one of the two had tasted the cake icing and tested positive for thallium in blood and urine specimens. Six (60%) of the ill patients were male; four (40%) were female. The median age of the patients was 12.5 years (range: 2--40 years). The median onset of illness was 24 hours after exposure (range: 12--72 hours) (Figure). An inverse relation was suggested between the amount of cake eaten and time to onset of symptoms. More rapid onset of illness occurred in persons who ate the most cake, and in adults. Of five patients who ate at least one piece† of cake, onset of illness was a median of 16 hours after exposure; of five patients who ate half a piece of cake or less, median onset of illness was 48 hours after exposure (r = -0.56, p=0.09, Pearson product-moment). Among the four patients aged >19 years, median onset of illness was 14 hours; among the six patients aged <14 years, median onset was 24 hours (r = -0.58, p=0.08, Pearson product-moment). Fatality was not significantly associated with sex, age, the amount of cake eaten, or the time to illness onset. By 30 days after ingestion, eight (80%) patients had experienced hair loss, which had begun within 7 days after eating the cake, and five (50%) still had neurologic deficits (e.g., lower limb muscle weakness and spasticity, with differing severity). Quantitative thallium levels were determined from blood and urine specimens of nine patients on the 16th day after eating any portion of the cake. Thallium was detected in all nine patients; median blood thallium level was 289 µg/L (range: 53--1,408 µg/L; reference level expected: <2 µg/L), and median calculated 24-hour urine excretion of thallium was 3,063 µg/L (range: 542--12,556 µg/L; reference level expected: <5 µg/L) (3). Blood thallium levels were weakly correlated with the amount of cake reported eaten (r = 0.66, p=0.06, Pearson product-moment). The father of family A, who did not become ill, but had tasted icing from the cake, had elevated blood and urine thallium levels. Reported by: Z Al-Mashhadani, A Al-Fatlawy, K Abu Nawas, Jordan Field Epidemiology Training Program; M Al-Nsour, B Hijawi, A Belbeisi, Ministry of Health, Hashemite Kingdom of Jordan; R Sharqawi, I Juma', S Hamaid, E Al-Saqa, F Al-Amouri, S Hameedi, S Sbeitan, L Mohammed, Jordan Specialty Hospital; M Jaghbeer, Univ of Jordan. N Al-Gasseer, O Mekki, B Ghanem, Office of WHO Representative in Iraq; A Adel Mohsin, Inspector General in Iraq; H Badar Musa, A Saloom, A Al-Alai, Baghdad Medical City. S Thomas, A Vale, T Sheehan, S Bradberry, UK National Poisons Information Svc. R Gerber, Div of Global Public Health Capacity Development, Coordinating Office for Global Health, CDC. Editorial Note:When ingested, thallium is a systemic poison that can produce multiple organ toxicity involving the gastrointestinal, neurologic, and cardiovascular systems (2). Among the distinctive effects of thallium poisoning are hair loss and painful, usually ascending, peripheral neuropathy (e.g., extreme pain, paresthesia, and weakness in distal extremities). In 1973, WHO recommended that thallium sulfate use as a rodenticide be discontinued because of its toxicity (4), and use in the United States for this purpose has been banned since 1975 (5). Approximately 60%--70% of thallium production is used in the electronics industry, with the remainder being used in manufacturing pharmaceuticals and glass. Prussian blue, a pigment discovered in the 1700s, acts as a sequestering agent for certain heavy metal ions and as an antidote to thallium poisoning. In 2003, the U.S. Food and Drug Administration approved the use of Prussian blue in 500 mg capsules as safe and effective for treatment of known or suspected internal contamination with thallium (radioactive or nonradioactive) or radioactive cesium. Deliberate contamination of food during production and preparation is rare (6,7), but instances of intentional thallium poisoning have been reported (1). This report describes one of the largest known clusters of thallium poisoning (8--10). Initial clinical findings in this report (i.e., gastrointestinal [100%] and neurologic symptoms [50%]) are similar to findings reported from previous clusters (gastrointestinal symptoms ranged from 11%--100% in previous clusters and neurologic symptoms ranged from 50%--100%). Although, the attack rate in this report (83%) is similar to those of previous clusters (71%--100%), the case-fatality rate in this report (40%) is higher than in previous clusters (0%--20%). Differences in clinical findings and case-fatality rates might be related to dosing and timing of ingestion, vehicles used (e.g., soft drinks, marzipan candy, and coffee), or formulation of the poisons (one cluster included both arsenic and thallium). The progression of signs and symptoms in this report are similar to those of previous clusters. Multiple government agencies and private sector health-care providers assisted and worked with each other, within and between countries, during the response to this incident. Such coordination and cooperation is critical for immediate, effective response to such events, whether they arise from unintentional or intentional circumstances. The sudden appearance of the characteristic signs and symptoms of hair loss and painful peripheral neuropathy in patients should prompt clinical consideration of thallium poisoning. Because of historical precedents, investigation should include assessment for criminal intent. References
* The Jordan Field Epidemiology Training Program was begun in 1998 with funding by the U.S. Agency for International Development and support from CDC. It became independent in 2008 and operates as part of Jordan's Ministry of Health. † "Piece" was not further defined; quantities were determined by subjective responses from family members. Table
All MMWR HTML versions of articles are electronic conversions from typeset documents. This conversion might result in character translation or format errors in the HTML version. Users are referred to the electronic PDF version (http://www.cdc.gov/mmwr) and/or the original MMWR paper copy for printable versions of official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 9/18/2008 |
|||||||||
|