|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
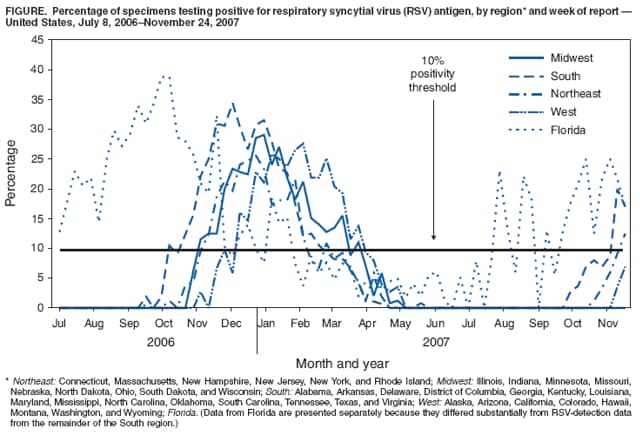
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Brief Report: Respiratory Syncytial Virus Activity --- United States, July 2006--November 2007Respiratory syncytial virus (RSV), the most common cause of severe lower respiratory tract disease among infants and young children, typically infects persons by age 2 years and can cause subsequent infections throughout life (1). RSV infection primarily manifests as bronchiolitis or pneumonia and results in approximately 75,000 to 125,000 hospitalizations in the United States each year (1). Persons at increased risk for severe disease or death include premature infants, older adults, and persons of any age with compromised respiratory, cardiac, or immune systems (2,3). RSV is transmitted from person to person via close contact, droplets, or fomites. In temperate climates, peak RSV activity typically occurs during the winter. However, year-to-year national and regional variability in the RSV season onset and offset* occurs in the United States (4). RSV circulation also varies by geographic location; for example, Florida has an earlier season onset and a longer season than the rest of the United States (5). Using data reported to the National Respiratory and Enteric Virus Surveillance System (NREVSS), this report summarizes RSV temporal and geographic trends in the United States during the weeks ending July 8, 2006--June 30, 2007, and for the first 5 months of the current reporting season (the weeks ending July 7--November 24, 2007). Appropriately timed diagnostic tests can provide data that indicate when the RSV season begins nationally and regionally, information that has been critical in determining when to begin RSV prophylaxis for infants and children at high risk for infection. NREVSS receives weekly reports from a passive voluntary network of laboratories regarding the number of specimens tested for specific viral pathogens, including RSV, and the number of positive results, stratified by test type. During July 2006--June 2007, a total of 94 clinical and public health laboratories reported RSV data. Laboratories that were included in this analysis met the following three criteria: reported >30 weeks of data, tested >15 specimens per week during the winter months, and reported >2% of specimens testing positive annually. Sixty-three (67%) laboratories representing 36 states met these criteria and reported a total of 126,617 RSV antigen-detection tests, of which 21,470 (17.0%) were positive. The national RSV season onset began during the week ending November 11, 2006, and continued for 19 weeks until the season offset (week ending March 17, 2007). Data were summarized by region† (Midwest, South [excluding Florida], Northeast, and West); data from Florida are presented separately because they differed substantially from RSV-detection data from the remainder of the South (5) (Figure). The 2006--07 RSV season onset occurred during the week ending November 11, 2006, in the Midwest (12 laboratories reporting); the week ending November 18 in the Northeast (eight laboratories reporting); and the week ending December 16 in the West (14 laboratories reporting). The season offset occurred during the week ending February 10, 2007, in the Northeast; the week ending March 17 in the Midwest; and the week ending March 31 in the West. The RSV season onset in the South (excluding Florida) (27 laboratories reporting) began during the week ending October 28, 2006, and continued until the week ending February 24, 2007 (18 weeks). The RSV season onset in Florida (two Miami laboratories reporting) began during the week ending July 1, 2006, and continued until the week ending January 27, 2007 (31 weeks). For the 2007--08 season, the number of reporting laboratories and geographic coverage has increased substantially as a result of a data-sharing agreement with Surveillance Data, Inc. (SDI), a private company that conducts RSV surveillance.§ On the basis of preliminary reports from the week ending July 7, 2007, to the week ending November 24, a total of 179 laboratories in 46 states and the District of Columbia reported 69,230 RSV tests and 5,173 (7.5%) positive results by antigen detection to NREVSS. Reports received through November 24 indicate that although the national RSV season onset has not yet occurred, the regional season onset occurred during the week ending November 17 in the South (58 laboratories reporting, excluding Florida) and during the week ending November 24 in the Northeast (23 laboratories reporting). As of November 24, reports from the Midwest (48 laboratories reporting) and West (37 laboratories reporting) did not indicate onset of the RSV season. Florida continued to have a unique onset (week ending August 4 [13 laboratories reporting]). Weekly updates indicating RSV national, regional, and state trends are available from the NREVSS website (6); data from Florida laboratories are available from the Florida Department of Public health website (7). No vaccine or effective therapy is available for RSV. Infants and children at risk for severe RSV infection can receive immune prophylaxis with monthly doses of a humanized murine anti-RSV monoclonal antibody during the RSV season (8). Specific immune prophylaxis guidelines are available from the American Academy of Pediatrics (8,9). Reported by: National Respiratory and Enteric Virus Surveillance System collaborating laboratories. CA Panozzo, MPH, AL Fowlkes, MPH, E Schneider, MD, LJ Anderson, MD, Div of Viral Diseases, National Center for Immunization and Respiratory Diseases, CDC. References
* As defined by NREVSS, RSV national and regional season onset is the first of 2 consecutive weeks during which the median percentage of specimens testing positive for RSV antigen is >10%. RSV season offset is the last of 2 consecutive weeks during which the median percentage of positive specimens is >10%. † Northeast: Connecticut, Massachusetts, New Hampshire, New Jersey, New York, and Rhode Island; Midwest: Illinois, Indiana, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota, and Wisconsin; South: Alabama, Arkansas, Delaware, District of Columbia, Georgia, Kentucky, Louisiana, Maryland, Mississippi, North Carolina, Oklahoma, South Carolina, Tennessee, Texas, and Virginia; West: Alaska, Arizona, California, Colorado, Hawaii, Montana, Washington, and Wyoming; Florida. § SDI conducts RSV surveillance with support from MedImmune, Inc. (Gaithersburg, Maryland). In fall 2006, CDC and SDI signed a memorandum of understanding to share RSV surveillance data to make the most complete RSV dataset available. The memorandum outlines the voluntary participation of laboratories, type of data shared, frequency of reporting, and approval and acknowledgements for data publication. The relationship between CDC and SDI is limited to data sharing, as outlined in the memorandum. CDC does not make recommendations regarding the administration of RSV immune prophylaxis. For additional information, contact NREVSS by e-mail at nrevss@cdc.gov.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 12/5/2007 |
|||||||||
|