|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
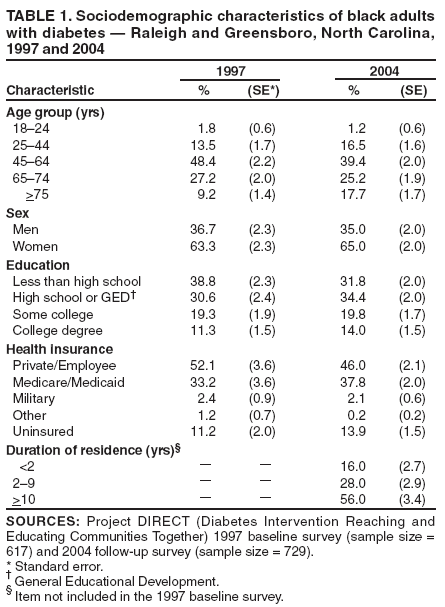
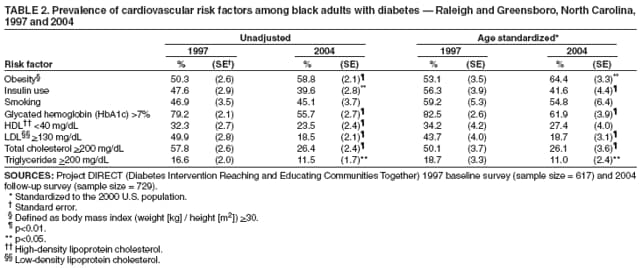
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Improvement in Lipid and Glycated Hemoglobin Control Among Black Adults with Diabetes --- Raleigh and Greensboro, North Carolina, 1997--2004Previous studies have indicated that, in the United States, black persons with diabetes have lower levels of glycemic and lipid control (1,2) and are at increased risk for diabetes-related complications (3) than white persons with the disease. Clinical trials have demonstrated that glycemic and lipid control can reduce the risk for microvascular and macrovascular complications among adults (4,5). In addition, recent studies of national survey data have indicated a secular trend of gradual improvements in blood pressure, cholesterol levels, and smoking rates among U.S. persons with diabetes (6,7). These studies have demonstrated an increase in the proportion of persons who meet recommended levels for blood pressure, glycated hemoglobin (HbA1c), and cholesterol (6,7). Whether black persons in the United States have benefited from these overall improvements is unclear. Surveys conducted among black adults in Raleigh and Greensboro, North Carolina, as part of Project DIRECT (Diabetes Intervention Reaching and Educating Communities Together), provided an opportunity to examine trends in diabetes control and risk for complications (8). Project DIRECT is a community-based intervention aimed at improving self-care, access to care, and quality of care for residents with diabetes (9). The analyses described in this report examined whether glycemic and lipid control improved in both communities from 1997 to 2004, a period of rapid advances in clinical understanding of how to control diabetes and its complications. This report summarizes the results of those analyses, which indicated improvements in the proportion of black adults with diabetes who reported that they were meeting recommended levels of HbA1c, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, triglycerides, and total cholesterol. However, a substantial number of these persons smoked and were above recommended glycemic and lipid levels at follow-up. Therefore, continued education of the public is important in improving quality of care and reducing risk factors for persons at high risk for diabetes and cardiovascular disease. As part of Project DIRECT, cross-sectional, population-based health surveys were conducted in person in two predominately black communities, one in southeast Raleigh and one in Greensboro, North Carolina, in 1997 (baseline) and 2004 (follow-up). The target population for each survey consisted of civilian, noninstitutionalized, English-speaking residents of the selected areas who were aged >18 years. The baseline survey used a multistage area probability sample design to select addresses for screening. The follow-up survey used a systematic random sample of mailing address lists within selected census tracts of the two communities. In the baseline and follow-up surveys, participants who answered "yes" to the question, "Have you ever been told by a doctor that you have diabetes?" were identified as persons with a previous diagnosis of diabetes. These participants were asked to complete the diabetes module, which examined levels of diabetes care, access to care, and preventive health-care practices. Women who reported being told they had diabetes during pregnancy only were classified as not having diabetes. Baseline survey participants with self-reported diabetes and all black respondents in the follow-up survey were asked to complete a laboratory examination. In 1997, a total of 2,639 households were screened, and 2,300 persons agreed to participate (response rate: 84.4% in Raleigh, 88.9% in Greensboro). Of the 2,300 participants, 617 had diabetes, and 407 agreed to participate in an examination. In the follow-up survey, 3,540 households were screened, and 3,083 persons agreed to participate (response rate: 78.9% in Raleigh, 83.5% in Greensboro). Of the 3,083 participants, 729 had diabetes, and 435 agreed to participate in an examination. A trained phlebotomist conducted the health examinations, which included measurements of height and weight to determine body mass index (BMI), defined as weight (kg) divided by height (m2), and fasting blood draws. Blood samples were transported to a central laboratory to assess HbA1c and lipid levels (HDL, LDL, total cholesterol, and triglycerides). The following criteria were used to classify persons as having glycemic, lipid, and BMI measures outside the ranges recommended by the American Diabetes Association: HbA1c >7%, HDL cholesterol <40 mg/dL, LDL cholesterol >130 mg/dL, total cholesterol >200 mg/dL, triglycerides >200 mg/dL, and BMI >30 (10). Smoking and insulin use were also assessed. Data were weighted to reflect the age, sex, and racial/ethnic composition of the study population based on the 2000 U.S. Census population. However, the results in this report are for black adults only. Prevalence estimates and estimated variances for the baseline and follow-up survey results were calculated; the two-sided Student's t-test was used to test the hypothesis that proportions were equal in the two surveys. Sociodemographic data were collected in the baseline and follow-up surveys (Table 1). The proportion of the population self-reporting diabetes who were obese (BMI >30) increased significantly (p<0.05) from the baseline to the follow-up survey (50.3% to 58.8%) (Table 2). However, improvements were reported in HbA1c and lipid levels. The proportion of black adults not meeting recommended HbA1c levels declined from 79.2% to 55.7%. The proportion not meeting recommended LDL cholesterol levels declined from 49.9% to 18.5%, and the proportion not meeting recommended total cholesterol levels declined from 57.8% to 26.4%. Significant decreases also were found in the proportion of persons not meeting recommended levels of triglycerides (16.6% to 11.5%) and HDL cholesterol (32.3% to 23.5%). The one risk factor that did not improve was smoking; prevalence remained at approximately 46%. In addition, the proportion of persons using insulin significantly decreased, from 47.6% to 39.6% (p<0.01). These results were then age standardized to the 2000 U.S. Census population, which yielded consistent results, although differences in HDL cholesterol levels were no longer statistically significant. Except for the secular trends described in this report, no overall significant differences in glycemic or lipid levels or in BMI were found between residents in southeast Raleigh and Greensboro. Reported by: SA Rutledge, PhD, EW Gregg, PhD, G Beckles, MD, DE Williams, MD, PhD, Project DIRECT Evaluation Study Group, Div of Diabetes Translation, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that the proportion of persons with diabetes from two predominately black communities in North Carolina who met the recommended glycemic and lipid levels increased from 1997 to 2004. These findings parallel national data (6,7). Improvements in lipid levels nationally have been attributed to multiple factors, including increased awareness and education, lipid testing, declining saturated fat and cholesterol content in the diet, and the proliferation of highly efficacious lipid-lowering drugs (6). Similarly, controlling glycemic levels has been the focus of major awareness campaigns directed at patients (e.g., the "Be Smart About Your Heart: Control the ABCs of Diabetes" campaign by the National Diabetes Education Program [NDEP]), and the aim of quality-improvement efforts in diabetes care. Measures to prevent or control risk factors through interventions targeting patients, health-care providers, and health-care systems might account for some of the improvements observed. In addition, improvements might be attributable to national public health programs such as NDEP and the National Cholesterol Education Program (NCEP). In contrast, the increasing proportion of persons who are obese and have diabetes is of concern and parallels trends from national surveys. This finding suggests that, despite apparent improvements in risk-factor control among persons with diabetes, this disease and its consequences will continue to be a threat until rates of obesity and other risk factors are reduced in the U.S. population. For example, despite improvements in risk-factor control among Project DIRECT study participants, approximately 55% remained above recommended HbA1c levels, approximately 26% were above recommended total cholesterol levels, and 23% were above recommended HDL cholesterol levels. The data indicate no change in smoking prevalence. The high proportion of smokers is a public health concern because of their increased risk for macrovascular and microvascular complications. The findings in this report are subject to at least two limitations. First, the use of mailing lists for the follow-up survey excluded residents who requested removal from the list or who used post office boxes. However, the possible incomplete coverage that resulted from using this method was corrected for by adding housing units missing from the sampling frame. Second, inclusion of data from southeast Raleigh, the site of Project DIRECT's community-based intervention project, might have influenced changes in glycemic and lipid control between the baseline and follow-up study. However, the findings in this report are consistent with those obtained when data from the community of Greensboro were analyzed separately. Continued education of the public through initiatives of NCEP, NDEP, and other programs remains important in the measures to reduce risk factors and improve quality of care for persons at high risk for diabetes and cardiovascular disease. NDEP is a joint program of CDC and the National Institutes of Health, which are charged with reducing the burden of diabetes and its complications in the United States. One NDEP initiative, "Small Steps. Big Rewards. Prevent Type 2 Diabetes," is designed to increase awareness and knowledge of diabetes in black communities and other populations at high risk. Additional information is available at http://www.ndep.nih.gov/campaigns/SmallSteps/SmallSteps_50ways.htm. CDC provides additional resources and technical assistance to diabetes control and prevention programs throughout the United States and its territories to improve diabetes education, quality of diabetes care, and early detection of diabetes complications. References
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
**Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 11/21/2006
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|