|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
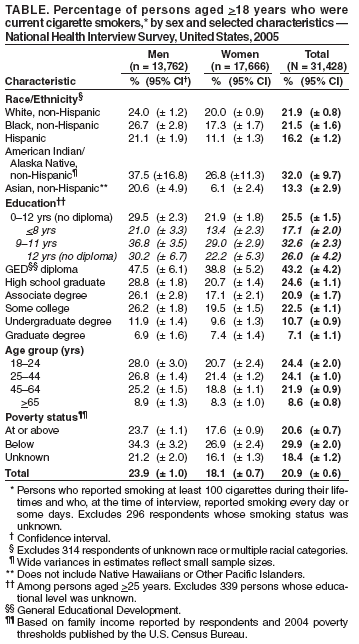
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Tobacco Use Among Adults --- United States, 2005Four of the Healthy People 2010 objectives* regarding tobacco use are to reduce the prevalence of cigarette smoking to 12.0%, cigar smoking to 1.2%, use of smokeless tobacco to 0.4%, and to increase cessation attempts among adult smokers to 75.0% (1). To assess progress toward achieving these four objectives, CDC analyzed self-reported data from the 2005 National Health Interview Survey (NHIS). This report summarizes the results of these analyses, which indicated lagging progress on all four objectives. In 2005, approximately 20.9% of U.S. adults were current cigarette smokers, the same percentage as in 2004 (2), suggesting that the 8-year decline in smoking prevalence among adults in the United States might be stalling. In addition, the findings indicated that, in 2005, an estimated 2.2% of U.S. adults were current cigar smokers, 2.3% used smokeless tobacco, and 42.5% of current cigarette smokers had stopped smoking for at least 1 day in the preceding 12 months because they were trying to quit (Figure). To meet the Healthy People objectives for 2010, full implementation of effective, comprehensive tobacco-control programs that address both initiation and cessation of tobacco use is needed in all states and U.S. territories. The 2005 NHIS adult core questionnaire, which contained questions on cigarette smoking and cessation attempts, was administered by in-person interview to a nationally representative sample of 31,428 persons from the noninstitutionalized U.S. civilian population aged >18 years. The same respondents were administered a supplemental questionnaire on cancer that contained questions regarding cigar smoking and use of smokeless tobacco (i.e., chewing tobacco and snuff). The response rate for both the adult core sample and supplemental questionnaire was 69.0%. Data were adjusted for nonresponse and weighted to provide national estimates of cigarette and cigar smoking, use of smokeless tobacco, and cessation attempts. Confidence intervals (CIs) were calculated using statistical software to account for the survey's multistage probability sample design. To measure cigarette smoking, respondents were asked, "Have you smoked at least 100 cigarettes in your entire life?" and "Do you now smoke cigarettes every day, some days, or not at all?" Current cigarette smokers had smoked at least 100 cigarettes during their lifetimes and reported smoking every day or some days. Current cigar smokers had smoked at least 50 cigars during their lifetimes and reported smoking cigars every day or some days. Current users of smokeless tobacco had used chewing tobacco or snuff at least 20 times during their lifetimes and reported using chewing tobacco or snuff every day or some days. Among current cigarette smokers, making at least one cessation attempt in the preceding year was defined as a "yes" response to the question, "During the past 12 months, have you stopped smoking for more than one day because you were trying to quit smoking?" In 2005, an estimated 20.9% (45.1 million) of U.S. adults were current cigarette smokers; of these, 80.8% (36.5 million) smoked every day, and 19.2% (8.7 million) smoked some days. The prevalence of current cigarette smoking varied substantially across population subgroups (Table). Current smoking was higher among men (23.9%) than women (18.1%). Among racial/ethnic groups, American Indians and Alaska Natives had the highest prevalence (32.0%), followed by non-Hispanic whites (21.9%), and non-Hispanic blacks (21.5%). Asians (13.3%) and Hispanics (16.2%) had the lowest rates. By education level, smoking prevalence was highest among adults who had earned a General Educational Development (GED) diploma (43.2%) and those with 9--11 years of education (32.6%); prevalence generally decreased with increasing education. Adults aged 18--24 years (24.4%) and 25--44 years (24.1%) had the highest prevalences. The prevalence of current smoking was higher among adults living below the poverty level (29.9%) than among those at or above the poverty level (20.6%) (Table). Certain populations had already surpassed the 2010 target of 12% for current cigarette smoking prevalence. These included Hispanic (11.1%) and Asian (6.1%) women, women with undergraduate (9.6%) or graduate (7.4%) degrees, men with undergraduate (11.9%) or graduate (6.9%) degrees, men aged >65 years (8.9%), and women aged >65 years (8.3%) (Table). Among current cigarette smokers, an estimated 42.5% (95% CI = +1.7; 19.2 million) had stopped smoking for at least 1 day during the preceding 12 months because they were trying to quit. Among the estimated 42.5% (91.8 million) of persons who had smoked at least 100 cigarettes during their lifetimes, 50.8% (46.5 million) did not smoke currently. In 2005, prevalence of current cigar smoking was 2.2% (CI = +0.2) and current smokeless tobacco use was 2.3% (CI = +0.3). Prevalence of cigar smoking and use of smokeless tobacco were higher among men (4.3% and 4.5%, respectively) than women (0.3% and 0.2%). Reported by: P Mariolis, PhD, VJ Rock, MPH, K Asman, MSPH, R Merritt, MA, A Malarcher, PhD, C Husten, MD, T Pechacek, PhD, Office on Smoking and Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. Editorial Note:The findings in this report indicate that the prevalence of cigarette smoking among U.S. adults did not change from 2004 to 2005. The adult prevalence might represent a stall in the decline in current cigarette smoking during the preceding 8 years and mirrors a lack of decline in smoking among adolescents since 2002 (3). Influencing factors might include smaller annual increases in the retail price of cigarettes (4) and a 26.5% reduction in funding for comprehensive state programs in tobacco control and prevention from 2002 to 2006 (5). Additionally, tobacco-industry advertising and promotional expenditures, primarily focused on price-discounting strategies, more than doubled from $6.7 billion in 1998 to $15.1 billion in 2003 (6). The rate of decrease in cigarette smoking among adults is not sufficient to meet the 2010 objective of 12%, and the rates of improvements are also not sufficient to meet the objectives for cigar smoking, use of smokeless tobacco, and attempts at smoking cessation. In addition, prevalence remains high among certain segments of the population. For example, in 2005, the prevalence was 43.2% among persons with a GED diploma and 32.6% among persons with education levels of 9--11 years. Effective interventions have been identified for decreasing initiation and increasing cessation, but they have not been implemented adequately (7,8). Recommended interventions include increases in the unit price for tobacco, mass media campaigns in combination with other interventions, and community mobilization campaigns to restrict access of minors to tobacco products in conjunction with enactment and enforcement of stronger retail sales laws and retailer education (8). Additional recommended interventions include reducing out-of-pocket costs to smokers for effective cessation therapies, multicomponent interventions (e.g., patient education, individual or group counseling, or nicotine replacement therapies) that include telephone quitlines, and health-care system changes (e.g., health-care provider reminder systems) (8). The findings in this report are subject to at least three limitations. First, estimates for cigarette smoking are based on self report and are not validated by biochemical tests. However, self-reported data on current smoking status have been determined to have high validity when compared with measured serum cotinine levels (9). Second, the NHIS questionnaire is administered in English and Spanish only, which might result in imprecise estimates for racial/ethnic populations unable to respond to the survey because of language barriers. Third, the small NHIS samples for certain populations (e.g., American Indians/Alaska Natives) result in single-year estimates with large confidence intervals. The lack of progress in reducing tobacco use and increasing cessation attempts among U.S. adults underscores the need for increasing measures to establish sustained, comprehensive, evidence-based tobacco-control programs that address both initiation and cessation. Full implementation of these programs at CDC-recommended levels of funding would accelerate progress toward meeting the 2010 objectives and decreasing the health burden and economic impact of tobacco-related diseases (7,8). References
* Objectives 27-1a (cigarette smoking), 27-1b (smokeless tobacco), 27-1c (cigar smoking), and 27-5 (cessation attempts among adult smokers). Table
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 10/25/2006 |
|||||||||
|