|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
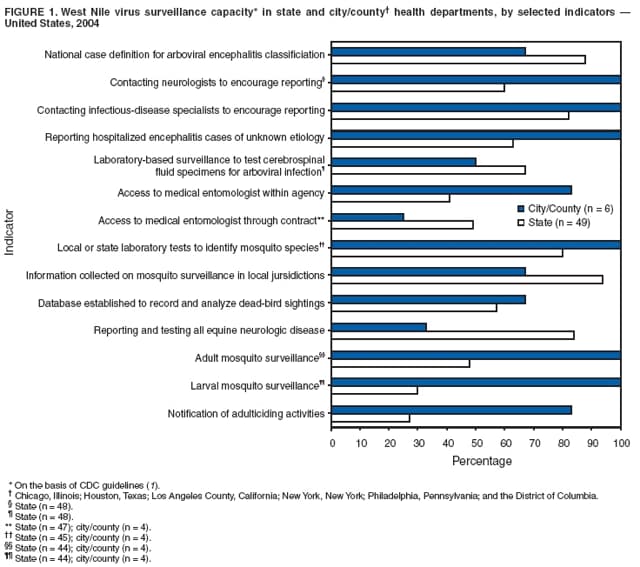
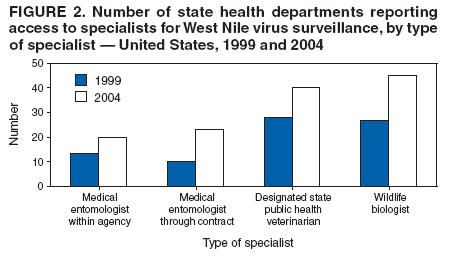
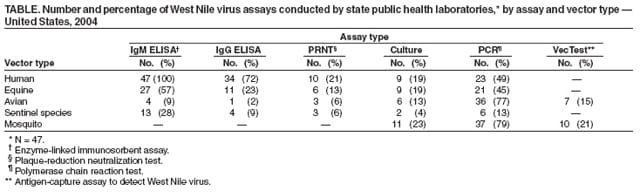
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Assessing Capacity for Surveillance, Prevention, and Control of West Nile Virus Infection --- United States, 1999 and 2004Please note: An erratum has been published for this article. To view the erratum, please click here. Indigenous human disease caused by West Nile virus (WNV) was first identified in the United States in August 1999 in the greater New York City area (1,2). By the end of 2004, human WNV disease had been reported in all states except Washington, Hawaii, and Alaska (3--8), and WNV transmission to humans had been documented by five routes: mosquito bites (principally from Culex spp.), blood transfusions, organ transplantation, transplacental transfer, and breastfeeding (1). During 1999--2005, a total of 19,525 cases of WNV disease in humans and 771 deaths were reported in the United States. In 2000, CDC first published guidelines for WNV surveillance, prevention, and control and created ArboNET, an electronic surveillance and reporting system. Beginning in 1999, WNV surveillance and prevention activities had been initiated in selected states and large cities through the CDC Epidemiology and Laboratory Capacity (ELC) cooperative agreements for emerging infectious diseases and subsequently expanded to all 50 states, six large cities/counties,* and Puerto Rico. In 2005, to assess the capacity of state and large-city/county health departments to conduct WNV surveillance, prevention, and control activities, the Council of State and Territorial Epidemiologists (CSTE), with assistance from the Association of Public Health Laboratories (APHL) and CDC, surveyed WNV programs in the 50 states and six large-city/county health departments. This report describes the results of that assessment, which indicated that all participating states and cities had well-developed surveillance and control programs for human, avian, equine, or mosquito WNV. Using CDC guidelines for WNV surveillance, prevention, and control (1), CSTE developed survey questions to assess human, avian, equine, and mosquito WNV infection and disease surveillance, laboratory capacity, and prevention activities. Respondents were instructed to answer the questions on the basis of their program activities during 2004 unless otherwise noted. Forty-nine (98%) of 50 states and all six city/county health departments responded to the survey. State Surveillance ActivitiesForty (82%) of 49 state programs reported contact with infectious-disease specialists by telephone, fax, mail, or electronic health alerts to encourage disease reporting; 29 (60%) of 48 reported contacting neurologists; and 28 (57%) of 49 reported contacting critical-care specialists. Thirty-one (63%) and 27 (55%) of 49 states, respectively, required reporting of encephalitis and meningitis cases of unknown etiology requiring hospitalization. Thirty-two (67%) of 48 state programs reported implementing a laboratory-based surveillance system to test cerebrospinal fluid (CSF) specimens for arboviral infection (Figure 1); the median number of CSF specimens tested in state public health laboratories (48 states) during 2004 was 117 (mean: 310 specimens; range: 0--2,600 specimens). State respondents were asked about their access to specialists (e.g., wildlife biologists, medical entomologists, and veterinarians) for both 1999 and 2004. These specialists are integral to WNV surveillance and control programs. Of the participating 49 states, 45 (92%) reported adequate access to expertise in wildlife biology, 20 (41%) had adequate access to medical entomologists within a public health agency, and 23 (49%) had access through contract or other formal arrangement. In addition, 40 (82%) had adequate access to a designated state public health veterinarian, an increase from 28 states in 1999 (Figure 2). Forty-six (94%) of 49 state respondents reported that they either conducted mosquito surveillance themselves, collected information about mosquito surveillance conducted by other agencies in their jurisdictions, or both (Figure 1). On average, nearly 62% of each state's jurisdiction was reported covered by mosquito surveillance. Forty-one (84%) of 49 state respondents had surveillance systems that included reporting of equine neurologic disease, 28 (57%) of 49 tracked dead-bird sightings, and 36 (80%) of 45 collected information about mosquito-infection rates by species. The median reporting interval, including collection of specimens, laboratory confirmation, and surveillance program notification, was 1 week for both human (range: 2--28 days) and bird specimens (range: 1--30 days). The median interval from report of a suspected human case to the surveillance program to report of a probable or confirmed case by the program to CDC was 16.5 days (range: 2--45 days). All six city/county programs and 46 (98%) of 47 states indicated that ELC funding for WNV surveillance also had enhanced surveillance for other mosquito-borne diseases. City/County Surveillance ActivitiesSurvey findings also demonstrated that WNV surveillance, prevention, and control programs in the six city/county health departments generally were well-developed, with features including outreach to specialists, reporting of equine neurologic disease, tracking of dead-bird sightings, collection of mosquito-infection rates, reporting of intervals from collection of human specimens to laboratory confirmation to surveillance program (median: 5.5 days), and testing for human infection (Figure 1). However, emphasis on different components of WNV surveillance, prevention, and control programs varied between state health departments and city/county health departments because of differences in roles and responsibilities. For example, mosquito control was primarily conducted by local agencies and contractors; local health departments more frequently conducted larval (100% versus 30%) and adult (100% versus 48%) mosquito surveillance than state health departments. Local health departments also more frequently provided public notification of adulticiding† activities (83% versus 27%). Laboratory TestingCDC guidelines recommend Biosafety Level 3 (BSL-3) practices, containment equipment, and facilities for all manipulations of WNV cultures and animal BSL-3 for experimental animal and vector studies (1). Forty-one (87%) of 47 state respondents reported that their public health laboratories had BSL-3 capability in 2004; eight (17%) of 47 reported BSL-3 capability for animal testing. All responding states (47 of 47) that provided laboratory testing data performed serologic testing for case confirmation by using enzyme-linked immunosorbent assay (ELISA) for WNV-specific IgM on human specimens, and 79% (37 of 47) performed WNV-specific polymerase chain reaction tests on mosquito specimens (Table). Plaque-reduction neutralization testing (PRNT), a confirmatory assay, was performed by a minority of state laboratories on specimens from human (10 of 47 [21%]), equine (six of 47 [13%]), avian (three of 47 [6%]), or other animal species (three of 47 [6%]). Overall, 14 (28%) of 49 states reported that their laboratory used PRNT. This assay was used to confirm all positive ELISA results by seven (50%) of the 14 states; PRNT was used more selectively by the other seven states for reasons not ascertained by the survey. Twenty-three (64%) of 36 states not performing PRNT reported that confirmatory testing was performed at CDC.§ Prevention ActivitiesAll or nearly all state programs delivered WNV prevention messages concerning use of DEET (N, N-diethyl-m-toluamide) (49 of 49 [100%]), residential mosquito control (47 of 49 [96%]), and other personal protective measures¶ (49 of 49 [100%]), whereas notification of adulticiding activities was delivered by 27% (13 of 49) of states. Adulticiding activities commonly are conducted by local agencies and contractors rather than by state health agencies. States used various methods to provide WNV prevention information in 2004, including posting information on agency websites (48 of 49 [98%]), issuing press releases (47 of 49 [96%]), and distributing informational brochures (44 of 49 [90%]). Less commonly used methods included door-to-door outreach in selected locations (11 of 49 [22%]) and participation in community clean-ups (four of 49 [8%]). All six city/county health agencies promoted WNV prevention in 2004 by using press releases; active distribution of informational brochures; town, community, or neighborhood meetings; and posting information on agency websites. Reported by: J Lemmings, MPH, L Robinson, MPH, Council of State and Territorial Epidemiologists, Atlanta, Georgia. R Hoffman, MD, Univ of Colorado Health Sciences Center, Dept of Preventive Medicine and Biometrics, Denver; E Mangione, MD, Colorado Dept of Public Health and Environment. R Humes, MS, Assoc of Public Health Laboratories, Silver Spring, Maryland. Editorial Note:The findings of the CSTE survey demonstrate that the capacity of WNV surveillance systems, technical expertise, laboratory capacity, and prevention programs have developed substantially since 1999. This progress can be attributed primarily to congressionally appropriated funds and technical guidance from CDC. The capacities that state and local health departments chose to emphasize or develop were based on the needs of their particular jurisdictions; however, establishment of this national program has enhanced viral laboratory capacity, veterinary disease surveillance capacity, and surveillance for vector-borne diseases other than WNV disease. For example, in 2004, states indicated improved access to medical entomologists and wildlife biologists compared with 1999. In addition, more state health departments currently have a designated state public health veterinarian. Finally, nearly all responding states had enhanced their capacity to conduct surveillance for other mosquito-borne diseases. The findings in this report are subject to at least one limitation. Because the six city/county health departments included in this survey are agencies that receive supplemental funding from CDC for WNV surveillance, prevention, and control, the extent to which these city/county health departments are representative of other city/county health departments is unclear. These findings illustrate the presence of well-developed WNV surveillance and control programs for human, avian, equine, or mosquito populations within state and local health departments. Because a universally applicable arbovirus surveillance system does not exist, surveillance systems within any given jurisdiction should be tailored according to the probability of arbovirus activity and available resources (1). Appropriate and timely response to surveillance data enables prevention of human and animal disease associated with WNV and other arboviruses. Response activities must include effective mosquito control and public education without delay if an increasing intensity of virus activity is detected by bird- or mosquito-based surveillance systems. WNV surveillance data collected in bird and mosquito populations help health officials predict and prevent human and domestic animal infections (1). Work by CDC and states to address newly emerging and reemerging infectious diseases (9,10) resulted in establishment of ArboNET within a national program to meet the emergence of WNV (1). On the basis of the findings described in this report, CSTE has recommended that WNV surveillance and control activities continue, but that the surveillance infrastructure be expanded to include other vector-borne and arboviral diseases. References
* Chicago, Illinois; Houston, Texas; Los Angeles County, California; New York, New York; Philadelphia, Pennsylvania; and the District of Columbia. † Application of pesticides to kill adult mosquitoes. § Confirmatory testing is performed by CDC for selected specimens considered high priority and beyond the capacity of the state public health laboratory or collaborating laboratory (1). ¶ Includes protective clothing, use of repellent on skin, and awareness of peak mosquito biting hours.
Figure 1
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Date last reviewed: 2/16/2006 |
|||||||||
|