 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Cancer Survivorship --- United States, 1971--2001Because of advances in early detection and treatment, cancer has become a curable disease for some and a chronic illness for others. Underscoring this change, persons with diagnoses of cancer increasingly are described as "cancer survivors" rather than "cancer victims" (1,2). Cancer survivors include all living persons who ever received a diagnosis of cancer (1). To highlight how the population of cancer survivors has changed in the United States, the National Cancer Institute and CDC studied cancer data collected during 1971--2001. This report summarizes the results of that study, which determined that the number of persons living with cancer increased from 3.0 million (1.5% of the U.S. population) in 1971 to 9.8 million (3.5%) in 2001. A national health objective for 2010 is to increase to 70% the proportion of cancer patients who are living >5 years after diagnosis (objective no. 3-15), an objective already achieved for children with cancer but not yet for adults. The growing number of persons living with cancer poses challenges for researchers to understand the physical, psychosocial, and economic effects of surviving cancer and for public health practitioners to develop evidence-based programs to promote the health and well-being of cancer survivors. This report uses incidence and follow-up data from registries in the Surveillance, Epidemiology, and End Results (SEER) Program of the National Cancer Institute to estimate the number of persons alive after a diagnosis of cancer and to monitor the progress in cancer survivorship (3). In addition, survival rates for persons receiving a diagnosis of cancer during 1991--2000 were compared with those receiving a cancer diagnosis during 1974--1976, the earliest dates for which SEER maintained data on survival; data collection for SEER began on January 1, 1973. To overcome the limited duration of data collection in all but the Connecticut registry (which began collecting data in 1935), estimates were adjusted to obtain lifetime or complete counts by using a statistical model that accounts for cases diagnosed before the start of the SEER program (4). The estimated number of cancer survivors was calculated by using data from SEER-9 registries to estimate the proportion of persons, by age, sex, and race, who were alive on January 1, 2001, and had a diagnosis of cancer during 1975--2000, taking into account loss to follow-up (4). These estimates were projected to U.S. population estimates, and data for all races combined were estimated by summing the counts for whites/unknown, blacks, and other races (5). Finally, the number of persons with a diagnosis of cancer no matter how long since the diagnosis was 1) estimated by adjusting the limited-duration data based on statistical modeling of incidence and survival, controlling for age and sex (6), and 2) validated by using 1940--1997 data from the historical Connecticut registry. For all cancers combined, the number of survivors in the United States has increased steadily during the last three decades. In 1971, an estimated 3.0 million persons were living with cancer, representing approximately 1.5% of the population. In 2001, an estimated 9.8 million persons were cancer survivors, approximately 3.5% of the population (Figure 1). In the absence of other competing causes of death, an estimated 64% of adults whose cancer was diagnosed during 1995--2000 could expect to be alive 5 years after diagnosis, compared with 50% for those whose cancer was diagnosed during 1974--1976. Among children (i.e., persons aged <14 years), 79% of cancer survivors during 1991--2000 were expected to be alive at 5 years and approximately 75% at 10 years, compared with 56% expected to live >5 years after diagnosis during 1974--1976. Among all cancer survivors in 2001, an estimated 14% had received a cancer diagnosis >20 years ago (Figure 2). More females than males were survivors, although more males than females received cancer diagnoses. In 2001, men had a higher proportion of lung cancer, for which survival chances are poor, whereas women had higher proportions of more readily detectable and treatable cancers (e.g., breast and gynecologic). Among cancer survivors in 2001, the most common primary cancer type was female breast cancer (22%), followed by prostate cancer (17%), colorectal cancer (11%), and gynecologic cancer (10%) (Figure 3). In 2001, an estimated 60% of all newly diagnosed cancers occurred among persons aged >65 years, who represented 61% of all cancer survivors. Thirty-three percent of cancer survivors were aged 40--64 years, 5% were aged 20--39 years, and <1% were aged <19 years. Reported by: J Rowland, PhD, A Mariotto, PhD, N Aziz, MD, G Tesauro, MSW, EJ Feuer, PhD, Div of Cancer Control and Population Sciences, National Cancer Institute. D Blackman, PhD, P Thompson, Div of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion; LA Pollack, MD, EIS Officer, CDC. Editorial Note:Increases in the number of persons surviving for longer periods after a diagnosis of cancer have resulted from 1) earlier diagnoses through increased screening, 2) more effective treatment, 3) prevention of secondary disease and cancer recurrence, and 4) decreases in mortality from other causes. This increase has led to a broader definition for cancer survivors. Cancer also is associated with aging. As the U.S. population ages, increased effort will likely be needed to plan for the care and optimal health of older persons, many of whom will become cancer survivors. The findings in this report are subject to at least four limitations. First, higher survival rates do not always result in lower cancer mortality rates (7); living longer with cancer might reflect how early the cancer was diagnosed rather than an improvement in outcome. Second, projection of race- and age-specific proportions from SEER to the U.S. population does not account for other prognostic factors (e.g., socioeconomic status and smoking). Third, persons with multiple tumors were categorized according to their first tumor; a person with melanoma and later breast cancer is counted as a survivor from melanoma but not from breast cancer. Estimators of the number of persons with cancer using different methods of counting multiple tumors are available (5). Finally, the estimates do not include broader health-status data that might indicate whether a survivor was cured, in active therapy, living with a chronic illness or disability, or dying from cancer. Methods that relate these factors to the trajectory of disease are being studied (8,9). The findings raise critical issues for public health practitioners. A growing need exists to promote health, prevent secondary disease, and ensure the social, psychological, and economic well-being of long-term cancer survivors and their families. Public health initiatives typically have addressed the early detection and prevention of cancer, and the change in cancer survivorship in part reflects the success of these efforts. Acknowledging the growing numbers of cancer survivors, public health practitioners are expanding efforts to address cancer survivorship and transform research findings into practice. Public health organizations and their partners are developing programs to support survivors and their families across the continuum of cancer treatment, health promotion, and survival. Long-term surveillance that monitors the health and social well-being of survivors after 5 years could provide a knowledge base for cancer survivorship. Development of clinical guidelines could help health-care practitioners provide follow-up to survivors. Policymakers could be educated about economic concerns faced by survivors, such as employment and insurance discrimination. The Office of Cancer Survivorship at the National Cancer Institute supports research that seeks to identify, examine, and prevent or control adverse long- and short-term effects associated with cancer. This office also disseminates information, such as the Facing Forward Series (available at http://www.cancer.gov/cancerinformation/life-after-treatment), to enhance the quality of life of survivors. CDC is supporting states and tribal organizations in developing and incorporating survivorship priorities into their comprehensive cancer-control plans. Advocacy organizations (e.g., Lance Armstrong Foundation and National Coalition for Cancer Survivorship) promote education, awareness, and community programs that offer innovative after-treatment services and support for survivors. Recommendations from these and other organizations are included in the recently published National Action Plan for Cancer Survivorship: Advancing Public Health Strategies (available at http://www.cdc.gov/cancer/survivorship/index.htm) (2), an Institute of Medicine report on Childhood Cancer Survivorship (10), and Living Beyond Cancer: Finding a New Balance from the President's Cancer Panel (available at http://pcp.cancer.gov). Recommendations include establishing a representative registry of survivors, continuing research on the chronic and late effects of cancer, exploring programs that enable survivors to access and navigate complex health-care systems and coordinate care, creating clinical guidelines for follow-up care, developing public education programs on survivorship, and evaluating the effects and outcomes of these efforts. References
Figure 1 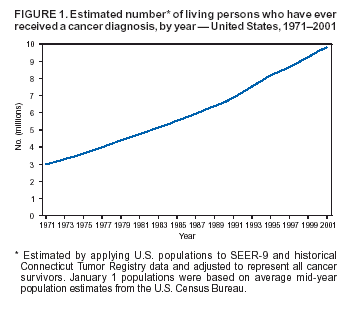 Return to top. Figure 2 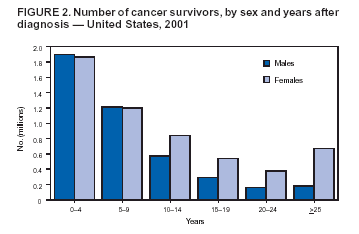 Return to top. Figure 3 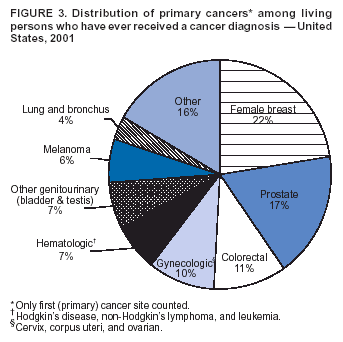 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 6/23/2004 |
|||||||||
This page last reviewed 6/23/2004
|