 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Outbreak of Severe Rotavirus Gastroenteritis Among Children --- Jamaica, 2003In late May 2003, the Jamaican Ministry of Health (MoH) identified a sharp increase in the number of acute gastroenteritis (AGE) cases reported throughout the country (Figure), accompanied by increases in AGE-associated hospital admissions and deaths among children. The greatest increase in AGE cases was observed among children aged <5 years in the southeastern parish of Kingston and St. Andrew. During June--July, 12 AGE-associated deaths were reported among children aged <8 years. MoH began an investigation to determine the etiology of the outbreak, ascertain risk factors for illness and death, and identify appropriate control measures. This report presents the preliminary results of that investigation, which determined that the AGE cases were associated with rotavirus and deaths might have been reduced by appropriate AGE case management, indicating a need for additional education of caregivers regarding AGE treatment. The increase in AGE cases was detected by Jamaica's National Sentinel Surveillance System (NSSS), which receives weekly reports that include the number of patient visits for AGE among children at 55 sentinel sites. In addition, review of admissions at two Kingston and St. Andrew hospitals identified an increase in the number of children hospitalized for AGE. Mandatory investigation and reporting to MoH found a concurrent increase in the number of diarrheal deaths among children. Interviews with primary caregivers suggested that eight of the 12 deaths were attributable to diarrhea. These eight deaths occurred among children aged 4 months--3 years (mean: 17 months). All eight children had watery diarrhea and vomiting that began 1--5 days before death. All had visited a public or private health-care provider at least once for treatment. Five children had received oral rehydration therapy (ORT) for their diarrheal illness; three received no ORT during their clinic visits. Three children were treated with antibiotics, two with antidiarrheals, and three with antiemetic injections. Testing for Salmonella, Shigella, Vibrio cholerae, and Escherichia coli O157:H7 on 43 stool specimens collected during June--July as part of NSSS surveillance identified four Shigella spp. and nine Salmonella spp. isolates. This was an expected finding for that time of the year. However, rotavirus was identified by latex agglutination in 21 (49%) of the initial 43 stool specimens and by enzyme-linked immunosorbent assay in 33 (50%) of an additional 66 stool specimens collected from children aged <5 years as part of the MoH investigation. Further testing at CDC identified rotavirus in five of seven stool specimens from persons aged >5 years. Testing of 32 stool specimens was negative for norovirus, sapovirus, and astrovirus; however, adenovirus was identified in three specimens, all of which also had evidence of rotavirus. Initial characterization of 23 rotavirus samples obtained as part of the MoH investigation indicated the presence of three common serotypes; no vaccine strain was identified. An epidemiologic investigation of this rotavirus-associated outbreak continues to identify risk factors for severe illness and death. As of November 12, no food or water source had been identified. Preventive efforts have focused on advising parents and physicians of the benefits of ORT for children with AGE. Reported by: D Ashley, MD, E Hedmann, MD, K Lewis-Bell, MD, E Ward, MD, Jamaican Ministry of Health; J Bryce, MD, National Public Health Laboratory, Kingston, Jamaica. RM Turcios, MD, D Tuller, MA Widdowson, VetMB, JS Bresee, MD, S Adams, S Monroe, PhD, JR Gentsch, PhD, RI Glass, MD, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; TK Fischer, MD, EIS Officer, CDC. Editorial Note:In Jamaica, rotavirus is usually confined to winter months (1), occurs among children aged <3 years, and is no longer associated with substantial mortality. Identification of rotavirus as the etiologic agent of this large outbreak of severe AGE seemed improbable because the outbreak occurred during the summer, included children aged >3 years, and resulted in multiple deaths. However, laboratory tests confirmed rotavirus as the etiologic agent, and identified multiple common rotavirus strains. Environmental exposures are being considered as explanations for this unusual outbreak. Ongoing studies are examining heavy rainfalls that occurred in late May and might have flooded latrines in crowded urban areas, causing fecal contamination of water sources. Communitywide outbreaks of rotavirus attributed to fecally contaminated water have been reported but are uncommon (2). This outbreak underscores the importance of surveillance for rotavirus disease. Rotavirus remains a major cause of diarrheal deaths worldwide (3), many of which might be prevented by aggressive use of ORT (4) and vaccines (5). The investigation of the outbreak in Jamaica suggested that AGE-associated deaths might be attributable to inappropriate case management. Certain children did not receive adequate ORT treatment, nor was home use of ORT emphasized. Certain children received antiemetic and antidiarrheal injections, which are not part of standard diarrhea management. Additional education of physicians, parents, and other caregivers regarding ORT can reduce the severity and mortality from diarrhea during AGE outbreaks (6). References
Figure 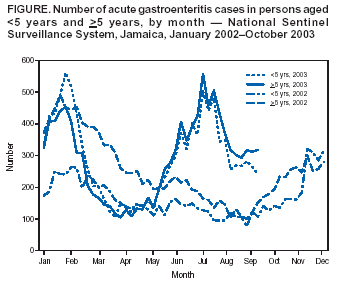 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 11/13/2003 |
|||||||||
This page last reviewed 11/13/2003
|