|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
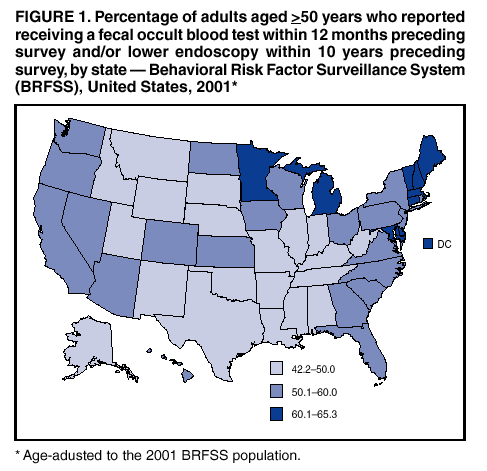
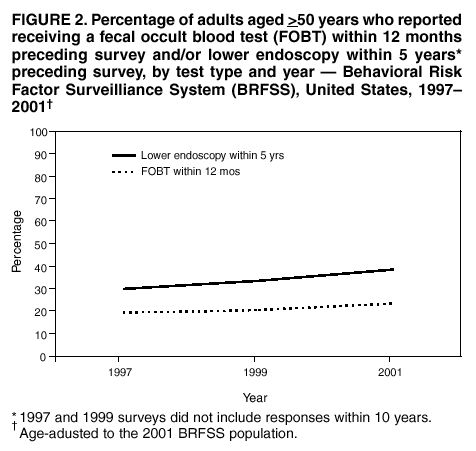
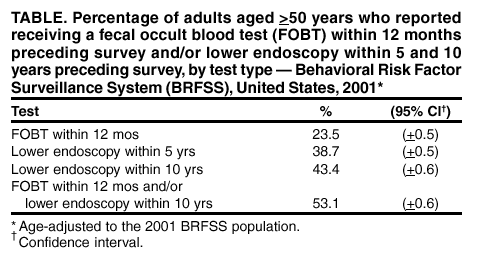
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Colorectal Cancer Test Use Among Persons Aged >50 Years --- United States, 2001Colorectal cancer is the second leading cause of cancer-related death in the United States (1). The lifetime risk for having colorectal cancer diagnosed is 6% (2). Screening measures decrease the incidence and mortality of colorectal cancer by detecting early disease and removing precancerous lesions (3). The U.S. Preventive Services Task Force recommends routine cancer screening for U.S. adults aged >50 years with one or a combination of the following screening options: annual home fecal occult blood testing (FOBT), sigmoidoscopy every 5 years, colonoscopy every 10 years, or double contrast barium enema every 5 years (3). To estimate rates and evaluate trends for colorectal cancer test use among U.S. adults aged >50 years, CDC analyzed data from the 2001 Behavioral Risk Factor Surveillance System (BRFSS) on the use of FOBT and sigmoidoscopy/colonoscopy and compared the data for 2001 with those for 1997 and 1999. This report summarizes the results of that analysis, which indicate that despite small increases in the self-reported use of colorectal cancer tests, screening rates remain low. Efforts to increase awareness and encourage regular colorectal cancer screening should continue. BRFSS is a state-based, random-digit--dialed telephone survey of the civilian, U.S. noninstitutionalized population aged >18 years. In 2001, all 50 states, the District of Columbia, Puerto Rico, the Virgin Islands, and Guam participated in BRFSS. Respondents aged >50 years, the age group for which colorectal cancer screening is recommended, were asked whether they ever had used "a special kit at home to determine whether the stool contains blood" (FOBT), whether they ever had "a tube inserted through the rectum to view the bowel for signs of cancer or other health problems" (sigmoidoscopy/colonoscopy), and when these tests were last performed. For this report, both sigmoidoscopy and colonoscopy are described as "lower endoscopy." Previous reports have examined lower endoscopic surveillance within 5 years as a measure of compliance with screening guidelines (4). Because BRFSS could not differentiate between sigmoidoscopy and colonoscopy, for this survey, the surveillance period was 10 years to include those undergoing colonoscopy. Any respondents reporting lower endoscopy within 10 years were considered to have been screened within the recommended period. Percentages were estimated for persons aged >50 years who had reported FOBT ever and within the 12 months preceding the survey, lower endoscopy ever and within 5 and 10 years preceding the survey, and FOBT within 12 months and/or lower endoscopy within 10 years preceding the survey. For the 2001 BRFSS, the median state response rate was 51.1% (range: 33.3%--81.5%) using the CASRO method (5). A total of 87,729 persons aged >50 years responded. Responses coded as "don't know/unsure" or "refused" were excluded from analysis (3%--4%). Proportions, standard errors, and 95% confidence intervals were calculated by using SAS v8 and SUDAAN. Data were weighted to the age, sex, and race/ethnicity distribution of the adult population in each state by using intercensal estimates and age standardized to the 2001 BRFSS population. Estimates for the percentage of adults aged >50 years who self-reported receiving either FOBT within 12 months or lower endoscopy within 5 years (1997 and 1999 surveys did not include responses within 10 years) were compared for 1997, 1999, and 2001. In 2001, an estimated 44.6% of adults aged >50 years had ever had FOBT, and 47.3% had ever had a lower endoscopy. An estimated 23.5% had FOBT within 12 months; 43.4% had lower endoscopy within 10 years; 53.1% had one or both tests within the periods described (Table). By state, the estimates for FOBT within 12 months ranged from 6.8% in Alabama to 34.5% in Maine; for lower endoscopy within 10 years, estimates ranged from 28.4% in the Virgin Islands to 58.5% in Minnesota. The estimates for reporting either FOBT within 12 months and/or lower endoscopy within 10 years varied by state from 42.2% in Oklahoma to 65.3% in the District of Columbia (Figure 1). The percentage of persons aged >50 years who had received FOBT within 12 months was 19.4% in 1997, 20.4% in 1999, and 23.5% in 2001. For lower endoscopy within 5 years, the proportions were 29.9%, 33.3%, and 38.7%, respectively (Figure 2). Reported by: L Seeff, MD, M Nadel, PhD, D Blackman, PhD, Div of Cancer Prevention and Control, National Center for Chronic Disease Prevention and Health Promotion; LA Pollack, MD, EIS Officer, CDC. Editorial Note:The findings in this report indicate that colorectal cancer test use among U.S. adults remains low. Approximately half of U.S. adults aged >50 years have not received the recommended screening. The findings in this report are subject to at least five limitations. First, the percentages reported overestimate colorectal cancer screening rates because 1) BRFSS could not differentiate test use specifically for screening from tests performed for diagnostic purposes and 2) persons who received sigmoidoscopy outside the recommended 5-year screening interval, but within 10 years, were considered compliant with screening guidelines. As a result, colorectal cancer screening rates are probably lower than the estimates in this report. Second, BRFSS excludes residents of institutions and persons who do not own telephones. Third, estimates from BRFSS were based on self-reports and were not validated; however, previous studies document moderate-to-good concordance between the self-reporting of colorectal cancer tests and medical records (6,7). Fourth, the response rate of 51.1% is low and has been low in previous years (62.1% in 1997 and 55.2% in 1999) (5). Health-care--seeking behaviors might differ among respondents and nonrespondents. Finally, data on the use of barium enema, another option for colorectal cancer screening, were not provided in BRFSS. However, barium enema is recommended less often than FOBT or sigmoidoscopy (8). Colorectal cancer test screening rates are much lower than breast and cervical cancer test screening rates (mammography and Papanicolaou smear, respectively) (9). This shortfall warrants increased public and health-care provider awareness and supportive health-care systems that emphasize and ensure accessibility to colorectal cancer screening. In July 2001, Medicare reimbursement was approved for colonoscopy screening for persons with average risk for colorectal cancer; this measure might increase future screening rates. To promote colorectal cancer screening, CDC will launch its annual "Screen for Life: A National Colorectal Cancer Awareness Campaign" (http://www.cdc.gov/cancer/screenforlife), which encourages persons aged >50 years to discuss screening for colorectal cancer with their doctor and to select appropriate test(s). For health-care providers, CDC also has produced an education program, "A Call to Action: Prevention and Early Detection of Colorectal Cancer" (http://www.cdc.gov/cancer/colorctl/calltoaction). In addition, CDC has supported a measure of colorectal cancer screening for the Health Plan Employer Data and Information Set (HEDIS), a set of standardized performance measures that permits comparison of managed care organizations. The measure has been approved provisionally for inclusion in HEDIS in 2004. To address issues related to mass screening, CDC's Survey of Endoscopy Capacity will examine the national distribution of lower endoscopes and trained health-care providers. References
Acknowledgment This report is based on data contributed by state BRFSS coordinators.
|
Use of trade names and commercial sources is for identification only and does not imply endorsement by the U.S. Department of
Health and Human Services. |
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices.
Page converted: 3/13/2003
|
|
|||||
|
HOME |
ABOUT MMWR |
MMWR SEARCH |
DOWNLOADS |
RSS
|
CONTACT
|
|||||
|
|
|||||
|
This page last reviewed 3/13/2003