 |
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Influence of Homicide on Racial Disparity in Life Expectancy --- United States, 1998Life expectancy (LE) is an important indicator of the health of populations. Since the early 1900s, when estimates of LE began to be tabulated in the United States, the LE of blacks has been lower than that of whites (1). Homicide, which disproportionately affects blacks, particularly young males, contributes to this difference in LE. To examine the associations between homicide, LE, and race, CDC analyzed 1998 mortality files from the National Center for Health Statistics (NCHS). This report summarizes the results of that analysis, which indicate, that in 1998, the LE for blacks was approximately 6 years shorter than for whites and that, after heart disease and cancer, homicide was the next largest contributor to the 6-year discrepancy. Violence prevention strategies (e.g., programs for youth offenders) have been implemented for the general population. More research is needed to determine an approach to target the male black population and to reduce LE disparity. NCHS mortality files for 1998 (2) and the multiple-decrement life table (3) were used to examine differences between whites and blacks. These methods were used to partition the contribution to LE at birth by selected causes of death using the International Classification of Diseases, Ninth Revision, (ICD-9) codes* for the four major race-sex groups (black-males, black-females, white-males, white-females) in the United States. The contribution in years for each cause of death to the black/white differential and statistical tests of difference (Z-scores) were determined using Survival software (4), with whites as the referent group. Causes of death used were based on the leading causes of death in 1998 for the total population and for both racial populations. Other causes of death were categorized as "all other causes." In the United States during 1998, whites lived 6.2 years longer than blacks. Among the leading causes of death that contributed to the difference were heart disease (1.7 years; 27.4%), cancer (1.2 years; 19.4%), homicide (0.6 years; 9.7%), stroke (0.5 years; 8.1%), and "all other causes" (1.9 years; 30.6%). The LE differential was 6.4 years for males and 4.4 years for females. Among males, some of the leading causes of death that contributed to the LE differential were heart disease (1.2 years; 19.0%), cancer (1.0 years; 15.6%), and homicide (0.9 years; 14.1%) (Figure 1), and among females were heart disease (1.2 years; 27.3%), cancer (0.5 years; 11.4%), and perinatal disease (e.g., birth trauma, birth asphyxia, ectopic pregnancy, and maternal death) (0.4 years; 9.1%). Stroke and human immunodeficiency virus (HIV) accounted for 0.3 years (6.8%) and 0.3 years (6.8%), respectively, of the LE differential among females and 0.4 years (6.3%) and 0.6 years (9.4%), respectively, among males. Homicide among black females contributed 0.2 years (4.5%) to the LE differential (Figure 1). Reported by: L Potter, PhD, Children's Safety Network, Education Development Center, Inc., Boston, Massachusetts. Etiology and Surveillance Br, Div of Violence Prevention, Office of Statistics and Programming, National Center for Injury Prevention and Control; National Center for Health Statistics; and an EIS Officer, CDC. Editorial Note:The findings in this report document racial disparities in LE, which were attributable mainly to blacks having a shorter LE than whites for each examined cause of death (except suicide). For the total U.S. population in 1998, homicide ranked 13th among causes of death (5), accounting for <1% of all deaths. However, homicide accounted for approximately 10% of the LE differential. This finding suggests that causes of death that rank low for the total population may be important targets to address in attempting to eliminate the LE gap between these populations. During 1985, the U.S. Department of Health and Human Services conducted the first analyses using health indicators that documented the health status of minority populations and found that approximately 60,000 excess deaths (i.e., the difference between the number of deaths observed in a racial/ethnic group and the number of deaths that would have occurred in that group if it had the same death rate as the non-Hispanic white population) occurred among blacks each year in the United States (6). Health disparities between blacks and the general population have been attributed to less access to health care and to health-care coverage. Risk factors for violence include living at or below the poverty level, living in single parent households, and having poor academic performance and/or exposure to neighborhood violence (e.g., gangs) (7). The 1998 publication of The Initiative to Eliminate Racial and Ethnic Disparities in Health indicated a commitment to eliminating longstanding racial/ethnic disparities in health status by 2010. The initiative focuses on six key areas of health that disproportionately affect multiple racial/ethnic minority groups at all ages (8): infant mortality, cancer screening and management, cardiovascular disease, diabetes, HIV, and vaccination coverage. The findings in this report are consistent with previous findings that show homicide to be a leading contributor to the difference in LE between blacks and whites (9) and underscore the need to include homicide among the key areas. The findings in this report are subject to at least three limitations. First, incorrect diagnoses or errors can result in inaccuracies in death records. Second, although approximately 99% of deaths in the United States are reported systematically (5), denominator data (population estimates) that refer to race or color may be inaccurate (5). Third, several assumptions (e.g., that life expectancy is aged 85 years) that could be technically flawed were made in constructing the life table model in this analysis (3). Preventing homicide requires integrated approaches from multiple disciplines, including criminal justice, education, social services, community advocacy, and public health. Strategies for preventing violence among youth (e.g., social-cognitive, mentoring, and family-based approaches) have been described in Best Practices to Prevent Violence by Children and Adolescents: A Sourcebook for Community Action (10) and in the Surgeon General's Report on Youth Violence (7). These prevention programs and strategies could be implemented by educators, public health practitioners, and law enforcement agencies to target black males. Reducing the racial LE differential in homicide will improve the health of blacks in the United States and thus reduce racial disparities in health. References
*Codes 042--044; 140--208; 390--398, 402, 404--429; 430--438; 760--779; E950--E959; E810--E825, E958.5, E988.5; E960--E978. Figure 1 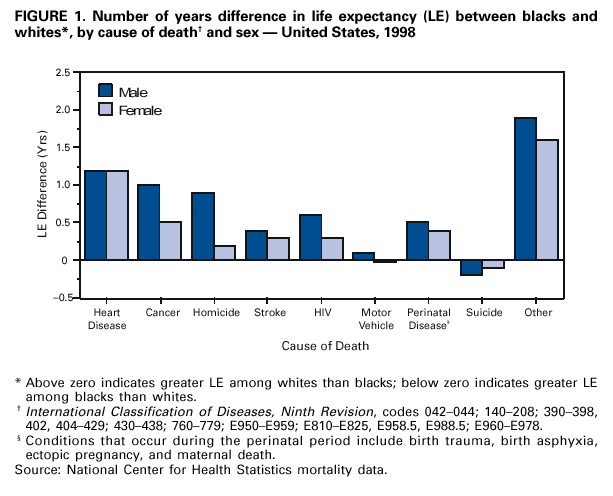 Return to top.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 9/14/2001
|