|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
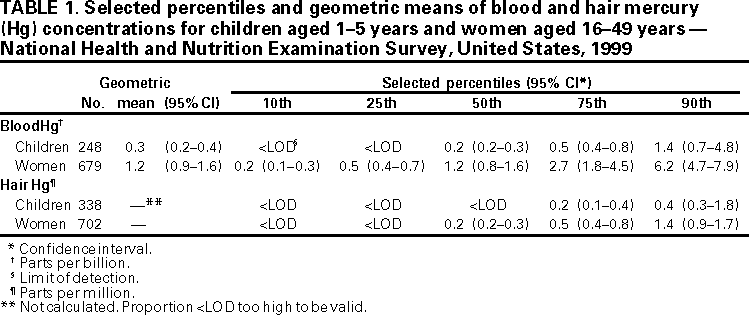
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Blood and Hair Mercury Levels in Young Children and Women of Childbearing Age --- United States, 1999Mercury (Hg), a heavy metal, is widespread and persistent in the environment. Exposure to hazardous Hg levels can cause permanent neurologic and kidney impairment (1--3). Elemental or inorganic Hg released into the air or water becomes methylated in the environment where it accumulates in animal tissues and increases in concentration through the food chain. The U.S. population primarily is exposed to methylmercury by eating fish. Methylmercury exposures to women of childbearing age are of great concern because a fetus is highly susceptible to adverse effects. This report presents preliminary estimates of blood and hair Hg levels from the 1999 National Health and Nutrition Examination Survey (NHANES 1999) and compares them with a recent toxicologic review by the National Research Council (NRC). The findings suggest that Hg levels in young children and women of childbearing age generally are below those considered hazardous. These preliminary estimates show that approximately 10% of women have Hg levels within one tenth of potentially hazardous levels indicating a narrow margin of safety for some women and supporting efforts to reduce methylmercury exposure. CDC's NHANES is a continuous survey of the health and nutritional status of the U.S. civilian, noninstitutionalized population with each year of data constituting a representative population sample. A household interview and a physical examination were conducted for each survey participant. During the physical examination, blood was collected by venipuncture for all persons aged >1 year and hair samples, consisting of approximately 100 strands, were cut from the occipital position of the head of children aged 1--5 years and women aged 16--49 years. Whole blood specimens were analyzed for total Hg and inorganic Hg for children aged 1--5 years and women aged 16--49 years by automated cold vapor atomic absorption spectrophotometry in CDC's trace elements laboratory. The detection limit was 0.2 parts per billion (ppb) for total Hg and 0.4 ppb for inorganic Hg (4). Hairs of 0.6 inches (1.5 cm) closest to the scalp (approximately 1 month's growth) were analyzed for total Hg concentration using cold vapor atomic fluorescence spectroscopy (5). The limit of detection for total Hg in hair varied by analytic batch; the maximum limit of detection (0.1 parts per million [ppm]) was used in these analyses. Blood Hg levels less than the limit of detection were assigned a value equal to the detection limit divided by the square root of two for calculation of geometric mean values. The geometric mean total blood Hg concentration for all women aged 16--49 years and children aged 1--5 years was 1.2 ppb and 0.3 ppb, respectively; the 90th percentile of blood Hg for women and children was 6.2 ppb and 1.4 ppb, respectively (Table 1). Almost all inorganic Hg levels were undetectable; therefore, these measures indicate blood methylmercury levels. The 90th percentile of hair Hg for women and children was 1.4 ppm and 0.4 ppm, respectively. Geometric mean values were not calculated for hair Hg values. Reported by: Center for Food Safety and Applied Nutrition, Food and Drug Administration. US Environmental Protection Agency. National Energy Technology Laboratory, Dept of Energy. National Marine Fisheries Laboratory, National Oceanic and Atmospheric Administration. National Center for Health Statistics; National Center for Environmental Health, CDC. Editorial Note:The NHANES1999 blood and hair Hg data are the first nationally representative human tissue measures of the U.S. population's exposure to Hg. Previous estimates of methylmercury exposure in the general population were based on exposure models using fish tissue Hg concentrations and dietary recall survey data (1). The NRC review provided guidance to the Environmental Protection Agency (EPA) for developing an exposure reference dose for methylmercury (i.e., an estimated daily exposure that probably is free of risk for adverse effects over the course of a person's life) (3). The NRC report recommended statistical modeling of results from an epidemiologic study conducted in the Faroe Islands near Iceland, where methylmercury exposures are high because of the large amount of seafood eaten by the local population. Results of this study were used to calculate a benchmark dose (BMD), an estimate of a methylmercury exposure in utero associated with an increase in the prevalence of abnormal scores on cognitive function tests in children. The lower 95% confidence limit of the BMD (BMDL*) was recommended to calculate the EPA reference dose. The NRC committee recommended a BMDL of 58 ppb Hg in cord blood (corresponding to 12 ppm Hg in maternal hair) (3). In the NHANES 1999 sample, there were no measurements of blood values >58 ppb or hair values >12 ppm. A margin-of-exposure analysis (i.e., an evaluation of the ratio of BMDL to estimated population exposure levels) showed ratios of <10 when comparing BMDL with NHANES 1999 estimates of the 90th percentile for blood and hair Hg levels in women of childbearing age. Margin-of-exposure measures of this magnitude indicate a narrow margin of safety (3) and suggest that efforts aimed at decreasing human exposure to methylmercury should continue. The findings in this study are subject to at least three limitations. First, the ratio of Hg in cord and maternal blood is uncertain. The NRC committee summarized some studies that suggest that cord blood values may be 20%--30% higher than corresponding maternal blood levels. However, other studies suggest that the ratio is closer to 1:1 (3); therefore, the NHANES values may not be directly comparable to BMDL recommended by NRC. Second, NHANES cannot provide estimates of Hg exposure in certain highly exposed groups (e.g., subsistence fishermen and others who eat large amounts of fish). Published data from studies of highly exposed U.S. populations indicated that some persons attain Hg tissue levels above BMDL (1). Third, the sample size of NHANES 1999 was small and the 1999 survey was conducted in only 12 locations. More data are needed to confirm these findings. The long-term strategy for reducing exposure to Hg is to lower concentrations of Hg in fish by limiting Hg releases into the atmosphere from burning mercury-containing fuel and waste and from other industrial processes. On the basis of data from EPA's National Toxics Inventory, air emissions of Hg decreased approximately 21% during 1990--1996, largely because of regulations for waste incineration (7). EPA expects this trend to continue as regulations are implemented for waste incineration and chlorine production facilities and are developed for electric power utilities (8,9). Fish is high in protein and nutrients and low in saturated fatty acids and cholesterol and should be considered an important part of the diet. The short-term strategy to reduce Hg exposure is to eat fish with low Hg levels and to avoid or to moderate intake of fish with high Hg levels. State-based fish advisories and bans identify fish species contaminated by Hg and their locations and provide safety advice (http://www.epa.gov/ost/fish†). The Food and Drug Administration advises that pregnant women and those who may become pregnant should not eat shark, swordfish, king mackerel, and tile fish known to contain elevated levels of methylmercury. Information is available at http://www.fda.gov/bbs/topics/ANSWERS/2001/advisory.html †. U.S. population estimates of Hg tissue levels by race/ethnicity, region, and fish consumption will become available after 2 additional years of NHANES data collection. NHANES will provide the opportunity to measure tissue Hg levels and to monitor the effectiveness of continuing efforts to reduce methylmercury exposure in the U.S. population. References
*A BMD of 85 ppb Hg in cord blood or 17 ppm Hg in maternal hair was estimated to result in an increase in the proportion of abnormal scores on the Boston Naming Test for children exposed in utero from an estimated background prevalence of 5% to a prevalence of 10% (6). BMDL recommended by NRC is the lower 95% confidence bound of the BMD. † References to sites of nonCDC organizations on the World-Wide Web are provided as a service to MMWR readers and do not constitute or imply endorsement of these organizations or their programs by CDC or the U.S. Department of Health and Human Services. CDC is not responsible for the content of pages found at these sites. Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 3/1/2001 |
|||||||||
This page last reviewed 5/2/01
|