|
|
|
|
|
|
|
| ||||||||||
|
|
|
|
|
|
|
||||
| ||||||||||
|
|
|
|
|
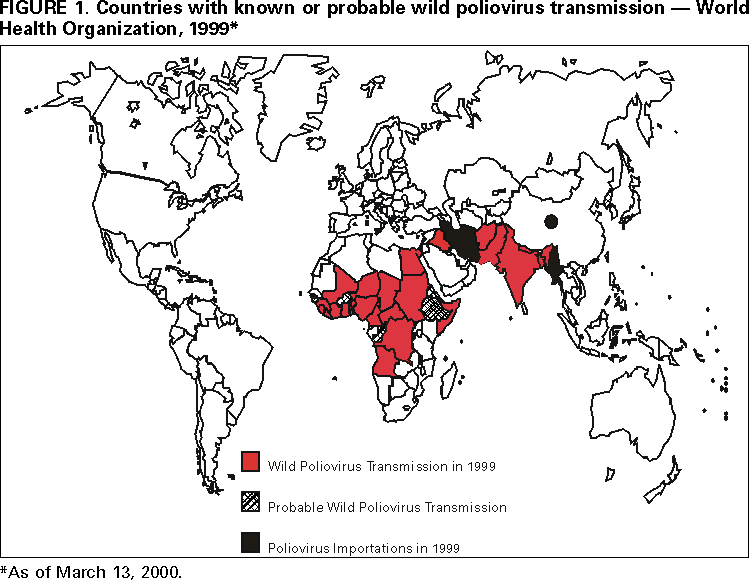
Persons using assistive technology might not be able to fully access information in this file. For assistance, please send e-mail to: mmwrq@cdc.gov. Type 508 Accommodation and the title of the report in the subject line of e-mail. Progress Toward Global Poliomyelitis Eradication, 1999In 1988, the World Health Assembly resolved to eradicate poliomyelitis globally by the end of 2000 (1). Since then, substantial progress has been made in implementing polio eradication strategies (2), and during 1999 these activities were accelerated to reach the global target. The number of countries where polio is endemic decreased, and the number and quality of vaccination rounds increased. Acute flaccid paralysis (AFP) surveillance improved, and political commitment and the global partnership for polio eradication strengthened. This report updates progress toward achieving the polio eradication goal during 1999. PROGRESS IN IMPLEMENTING STRATEGIESRoutine Vaccination During 1990--1997, reported coverage with three doses of oral poliovirus vaccine (OPV3) was approximately 80% globally. In 1998, OPV3 coverage decreased to 72%, reflecting the decline in coverage in four World Health Organization (WHO) regions (African, Eastern Mediterranean, European, and South-East Asian). Supplementary VaccinationIn 1999, approximately 470 million children aged <5 years in 83 countries were vaccinated during National Immunization Days* (NIDs) or Subnational Immunization Days† (SNIDs). The number of NID rounds in priority countries (i.e., those considered major global virus reservoirs or affected by conflict) increased (e.g., Afghanistan, Democratic Republic of Congo [DR Congo], and India). In India, approximately 1 billion OPV doses were distributed during four NID and two SNID rounds during October 1999--March 2000. Three rounds of NIDs in DR Congo reached approximately 8 million children in 1999. House-to-house vaccination was used increasingly during 1999 NIDs and SNIDs both in high-risk areas during "intensified NIDs" (e.g., in India) and exclusively in large-scale SNIDs in Nigeria and Pakistan. In Nigeria, house-to-house SNIDs reached 20%--40% (depending on the state) more children aged <5 years compared with the last fixed-post NID round. Mopping-up VaccinationAlthough additional SNIDs were conducted in border and other high-risk areas, few large-scale house-to-house vaccination activities (mopping-up campaigns) were conducted in 1999. An intense mopping-up campaign was conducted in southeast Turkey and in neighboring provinces in Iran, Iraq, and Syria, targeting the last known foci of transmission in the entire European Region and bordering countries in the Eastern Mediterranean Region. AFP SurveillanceAFP surveillance requires detection, investigation, and reporting of AFP cases among children aged <15 years. AFP is monitored by two main performance indicators: 1) the reported AFP rate not attributable to polio (i.e., nonpolio AFP rate) to assess the sensitivity of AFP reporting (target: nonpolio AFP rate of <1 cases per 100,000 population aged <15 years); and 2) the completeness of specimen collection (target: two adequate stool specimens§ from <80% of persons with AFP). In 1999, 30,003 AFP cases (Table 1) were reported globally (24,657 in 1998), and the number of cases reported from the African Region tripled during 1998--1999. Average specimen collection rates were maintained or improved in four of the six WHO regions; the decreased rate in the African Region reflected a major polio outbreak in Angola (3). The American Region was certified polio-free in 1994; three WHO regions have surpassed or are approaching certification level standards (e.g., achieving a nonpolio AFP rate of <1 cases per 100,000 population aged <15 years, with adequate stool specimens from <80% of persons with AFP). Laboratory NetworkIn December 1999, the Global Polio Laboratory Network comprised 126 national (or subnational), 16 regional, and six specialized laboratories; 108 (73%) laboratories were fully accredited, 16 (11%) were provisionally accredited, 14 (9%) were reviewed but not accredited, and 10 (7%) were pending review (4). Globally, the laboratory network processed an estimated 50,000 stool specimens for viral isolation during 1999; approximately 3000 polioviruses were isolated. Serotyping, intratypic differentiation, and genomic sequencing were performed on most wild isolates. IMPACT OF STRATEGIES ON POLIO INCIDENCEDuring 1998--1999, the number of known or suspected countries where polio is endemic decreased from 50 to 30 (Figure 1). Type 2 poliovirus is almost extinct, with the only known remaining foci existing in northern India (5). Genetic sequencing data from reservoir countries confirm that additional chains of type 1 and type 3 polio transmission have been broken and virus sublineages have become extinct. From 1998 to 1999, reported polio cases increased 10% (from 6349 to 6970), reflecting the improved AFP reporting from Africa and the wild poliovirus type 3 outbreak in Angola (3). Poliovirus circulation in the African Region is confined largely to the Horn of Africa and western and central Africa (6). Polio cases reported from the South-East Asian Region decreased from 4775 (1998) to 3330 (1999). This decline was attributed to decreased transmission in central and southern India; however, endemicity remains high in northern India and Bangladesh. In 1999 in the Eastern Mediterranean Region, 814 polio cases were reported (555 cases in 1998). Following the certification of the American Region as polio-free in 1994, the Western Pacific Region in 2000 will be the second WHO region to be certified formally as polio-free (7). PREPARING FOR THE POST-ERADICATION ERAThe criteria for certification of polio-free status (first by WHO region, then globally), defined by the Global Commission for the Certification of Poliomyelitis Eradication, requires that no indigenous wild poliovirus be found through optimal AFP surveillance for at least 3 years. Regional and national polio certification commissions are reviewing progress toward polio eradication in all WHO regions. A plan for increasing biocontainment of wild polioviruses to a small number of high biosafety laboratories has been prepared and initial implementation has begun in several WHO regions. Reported by: Vaccines and Biologicals Div, World Health Organization, Geneva, Switzerland. Respiratory and Enteric Viruses Br, Div of Viral and Rickettsial Diseases, National Center for Infectious Diseases; Vaccine Preventable Disease Eradication Div, National Immunization Program, CDC. Editorial Note:Since 1988, substantial progress in polio eradication has been reported from all six WHO regions (2). In 1999, progress made in accelerating global polio eradication included 1) passage of a resolution by all WHO member states to support accelerated polio eradication; 2) implementation of four NIDs in India (approximately 140 million children reached in each round) and two additional SNIDs in eight northern Indian states; 3) vaccination of millions of children in countries affected by conflict; 4) a dramatic increase in AFP surveillance quality; and 5) expansion of the global polio eradication partnership to include the World Bank, the Bill and Melinda Gates Foundation, the United Nations Foundation, and the Aventis Pasteur company. A multisector approach is needed in many countries to improve the quality of supplementary vaccination activities to ensure that every child is reached. Although more children are being vaccinated, many are unreached because of poor planning, inadequate social mobilization, and civil conflict. During 2000, efforts have been targeted at overcoming these obstacles, including augmentation of country-level technical and administrative capacity. The continuing surveillance achievements in Afghanistan, Somalia, and Sudan demonstrate that high-quality surveillance can be implemented even in the most difficult circumstances. The success of the United Nations Secretary General and other partners in establishing "days of tranquility" for NIDs during 1999 in DR Congo demonstrated the feasibility of working successfully in conflict-affected areas. Sustaining political commitment is essential in stopping polio and is critical in implementing high-quality eradication activities in remaining countries where polio is endemic. Some countries, particularly in the African Region, have stopped NIDs despite surveillance sensitivity that remains well below certification standards. Although substantial progress toward global polio eradication has been made during 1999, the interruption of virus transmission by the end of 2000 or as soon as possible will be feasible only if extraordinary efforts are taken in priority countries where polio is endemic, including 1) conducting extra NID rounds during the rest of 2000 and in 2001; 2) improving the quality of NIDs to reach all children, particularly children who have never received vaccine; 3) improving and maintaining AFP surveillance; 4) procuring sufficient vaccine to allow completion of polio eradication activities during 2000 and 2001; 5) expanding efforts to establish days of tranquility and truces to allow vaccination of children in countries affected by conflict; 6) meeting the projected financial shortage in external resources required through 2005¶; and 7) strengthening and maintaining political commitment. References
* Mass campaigns over a short period (days to weeks) in which two doses of oral poliovirus vaccine (OPV) are administered to all children, usually aged <5 years, regardless of vaccination history, with an interval of 4--6 weeks between doses. † Focal mass campaigns in high-risk areas over a short period (days to weeks) in which two doses of OPV are administered to all children in the target age group, regardless of vaccination history, with an interval of 4--6 weeks between doses. § Two stool specimens, collected 24 to 48 hours apart within 14 days of onset of paralysis, that arrive in the laboratory in good condition. ¶ The polio eradication initiative is supported by the national governments. External support is provided by the global polio eradication partnership (WHO; United Nations Children's Fund [UNICEF]; Rotary International; CDC; U.S. Agency for International Development; and the governments of Japan, the United Kingdom, Denmark, Germany, and others). New partners include the World Bank, the Bill and Melinda Gates Foundation, the United Nations Foundation, and the Aventis Pasteur Company.
Disclaimer All MMWR HTML versions of articles are electronic conversions from ASCII text into HTML. This conversion may have resulted in character translation or format errors in the HTML version. Users should not rely on this HTML document, but are referred to the electronic PDF version and/or the original MMWR paper copy for the official text, figures, and tables. An original paper copy of this issue can be obtained from the Superintendent of Documents, U.S. Government Printing Office (GPO), Washington, DC 20402-9371; telephone: (202) 512-1800. Contact GPO for current prices. **Questions or messages regarding errors in formatting should be addressed to mmwrq@cdc.gov.Page converted: 4/27/2000 |
|||||||||
This page last reviewed 5/2/01
|